Article Text

Abstract
Objective: To assess the impact of the laparoscopic inguinal release procedure with mesh reinforcement on athletes with groin pain.
Design: Prospective cohort study.
Setting: Private sector.
Patients: Professional and amateur sportsmen/women undergoing the inguinal release for groin pain.
Main outcome measurements: Change in patient’s symptoms, functional limitation and time to resuming sporting activity following surgery.
Results: 73 sportsmen/women underwent laparoscopic inguinal release in the study period, 37 (51%) of whom were professionals. 95% were male with a median age of 30 years. Following operation, patients returned to light training at a median of 1 week, full training at 3 weeks (professionals—2 weeks) and playing competitively at 4 weeks (professionals—3 weeks). 74% considered themselves match-fit by 4 weeks (84% of professionals). Following surgery, there was a highly significant improvement in frequency of pain, severity of pain and functional limitation in both the whole cohort and professional group. 88% reported a return to full fitness at follow-up, with 73% reporting complete absence of symptoms. 97% of the cohort thought the operation had improved their symptoms.
Conclusions: This study shows that the laparoscopic inguinal release procedure may be effective in the treatment of a subgroup of athletes with groin pain.
Statistics from Altmetric.com
Groin pain is a common complaint among sportsmen and women, particularly those participating in sports involving kicking, rapid accelerations and deceleration, and sudden change in direction.1 An extensive list of differential diagnoses exist, including muscle strains, stress fractures, intra-articular hip pathology, intra-abdominal causes and lumbosacral spinal disease.2 Sportsman’s groin or sportsman’s hernia are commonly used terms which encompass unexplained groin pain in athletes and are used to describe a syndrome of weakness of the posterior inguinal wall without a clinically recognisable hernia.345 Various explanations exist for this disorder, including avulsion of the conjoint tendon from the pubic tubercle, weakening of transversalis fascia, tears in internal oblique, tearing of external oblique or its aponeurosis causing superficial inguinal ring dilation, and abnormalities of rectus abdominis insertion.3467 Some authors feel that deficiency of the posterior inguinal wall is the most common operative finding in these patients.8 We believe that a true sportsman’s hernia does not exist and that the pathology relates to an enthesopathy of one of the attachments around the pubic tubercle, which may be analogous to tennis elbow. The majority of operative interventions thus far for this condition have attempted to support the posterior wall of the inguinal canal, using a standard mesh hernia repair,910111213 a modified hernia repair,14 Bassini repair31516 or more recently laparoscopic totally extraperitoneal (TEP)17181920 and transabdominal preperitoneal (TAPP)8202122 mesh hernia repair.
What is already known on this topic
Groin pain is a common complaint among athletes.
Various operative interventions to support the posterior wall of the inguinal canal have been utilised, with mixed results.
Many of these patients are tender over the insertion of the inguinal ligament; therefore release of the ligament was hypothesised to improve symptoms.
What this study adds
Symptoms in a subgroup of athletes with groin pain may relate to an enthesopathy of the attachments of the ligaments to the pubic tubercle.
Laparoscopic release of these ligaments combined with mesh repair to prevent future herniation may improve their symptoms without any compromise to their functional ability.
We have previously described our initial experience with laparoscopic inguinal ligament release followed by mesh reinforcement to prevent future herniation.23 This procedure was devised based on the observation that the majority of patients referred to our practice were tender over the insertion of the inguinal ligament. Similar to a tenotomy of adductor24 or forearm extensor tendons,25 it was hypothesised that a release of the inguinal ligament would alleviate patients’ symptoms. In our initial series of 28 patients followed up after the procedure, we demonstrated a significant improvement in pain severity, frequency and functional limitation, with 92% returning to normal activity levels. This was a retrospective study that focussed on a cohort of amateur sportsmen and manual workers. To confirm the benefit of this procedure in elite sportsmen, we performed a prospective study of a separate cohort of patients undergoing the procedure in the private sector consisting of predominantly high-performance athletes.
Methods
Study method
Data were collected prospectively on professional sportsmen/women undergoing a laparoscopic inguinal tenotomy between July 2004 and November 2007 at the Leicester Spire Hospital (BUPA). The majority of patients were referred by orthopaedic surgeons or physiotherapist. Only patients providing written consent to taking part in data collection were included.
A preoperative “tick-box” questionnaire was completed by all patients. Patients were asked when the pain occurred, the severity of pain and how much limitation the pain had on their work and lifestyle activities. They were also asked to rate their current level of fitness. The questionnaire also included an evaluation of use of analgesia, physiotherapy and rest before referral.
Patients were contacted after a minimum of 3 months after surgery by telephone (authors CDM and CDS). Patients were asked the same questions as the preoperative questionnaire in terms of pain occurrence, severity, limitations and current level of fitness. They were also asked about postoperative recovery in terms of time taken to resume general mobility, light training, full training and playing sport competitively. They were also asked about postoperative analgesia requirement and physiotherapy use. Finally, they were asked if they thought the procedure had been beneficial and if they would recommend the procedure to a colleague/team member with similar symptoms. Patients were informed that data were confidential and would not be fed back to their clubs without their permission in order to prevent under-reporting of symptoms and to ensure the reliability of the data.
Patient selection
Patients considered for operative treatment filled the following criteria. All patients must have had groin pain with no improvement following rest or limitation of sporting activity, physiotherapy, injection or previous surgery. Patients with symptoms for at least 6 weeks were considered for surgery. Only patients with localised tenderness over the insertion of the inguinal ligament and superficial ring with no overt evidence of a hernia were listed. Careful clinical examination is essential to select only those patients with inguinal ligament pathology. Clinical examination included palpation when the patient was in a supine position. To enhance this symptoms, patients were also asked to cough while the inguinal ligament attachment was palpated for tenderness. To elucidate this further the pubic tubercle was palpated and the athletes asked to flex the ipsilateral hip and adduct against resistance. In addition, the pain had to be reproduced on straining with the Valsava manoeuvre of sitting up against resistance. Imaging was not routinely used in preoperative assessment.
Surgical technique
All operations were undertaken by a single, experienced consultant laparoscopic surgeon (DML). Pneumoperitoneum was established via the umbilicus using the safe, open technique developed in Leicester. A small incision is made in the subumbilical skin followed by blunt dissection down to the cicatrix. A small incision is made in the cicatrix, which is then dilated, and a blunt 10 mm port inserted, through which the telescope is passed. Two other 5 mm ports are inserted under direct vision. The operator and assistant setup is identical to that routinely used for a transabdominal preperitoneal mesh repair (TAPP).26 Routine inspection of the hernial orifices is undertaken. The peritoneum is incised, and the whole inguinal region exposed so that the medial end of the inguinal ligament and its surrounding structures can be carefully examined. The femoral canal is also exposed carefully and an assessment made of the attachment of the inguinal, lacunar and pectineal ligaments. The ilio-pubic tract is divided, and the inguinal ligament and lacunar ligaments detached from the pubic tubercle using hook diathermy. Excess scar tissue (if present) from previous groin surgery is divided, and any old suture material removed. The pectineal ligament, if thickened, is divided also. Following this, a 15 by 12 cm synthetic mesh is positioned to cover the whole inguinal region and the medial edge secured using a laparoscopic stapler. The mesh repair has to be routinely undertaken following detachment of the inguinal ligament to prevent herniation. The peritoneum is then reattached to prevent any part of the mesh being exposed to the abdominal contents. The three small skin incisions are closed with absorbable vicryl and the wounds infiltrated with local anaesthetic. An ilio-inguinal nerve block using levobupivacaine is performed in all cases. Patients undergo routine postoperative monitoring and are discharged the same day if well, or the following day if they have had a long way to travel.
Return to full activity is encouraged as soon as possible following surgery. Patients are advised to undertake stretching exercises of the groin, incorporating bent knee lunges, and quadriceps stretch of the operated side. Training for sport is strongly encouraged after 1 week postsurgery and return to regular sporting activity after 2 weeks.
Statistical analysis
All statistical analyses were performed using SPSS version 12.0 (SPSS, Chicago). Categorical variables were compared using the χ2 test, and continuous variables compared using the Mann–Whitney test. A p value of <0.050 was considered significant.
Results
Demographics
Seventy-three sportsmen/women provided written consent to be included in the study, with a median age of 30 years (range 16–50 years). Ninety-five per cent (n = 70) were male. Forty-two were footballers, with 16 professionals, four semiprofessionals and 22 amateurs. Twenty-one were rugby players, with 18 professionals and three amateurs. The remainder included two professional cricket players, five athletes, one amateur cyclist, one semiprofessional tennis player and one professional horse rider. Nine rugby players, five footballers and the horse rider had competed at international level. Eleven patients (15%) had previously had surgery on the symptomatic groin. Previous operations were six Gilmore procedures, six inguinal hernia repairs (two laparoscopic) and two adductor tenotomies.
Preoperative
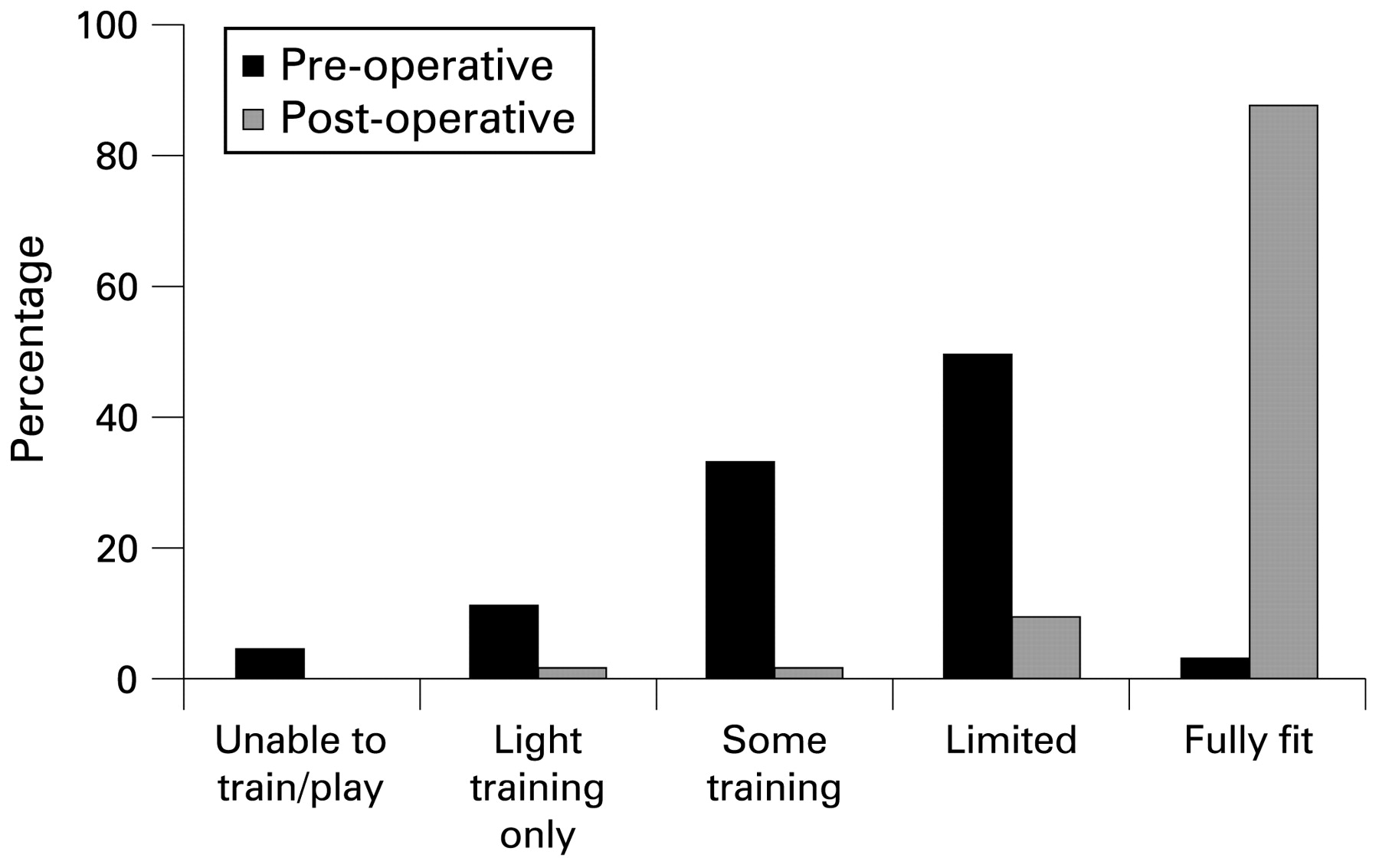
The median duration of pain in all patients was 5 months (range 1.5–24 months). Table 1 reports the main precipitants of pain. The majority experience pain frequently after playing sport (86%) or after light training (70%) (table 1). Forty-four per cent reported pain on coughing or sneezing, and 58% reported pain on getting out of the car or bed. The majority reported pain to interfere with their ability to play sports (95%) or train (86%), and 55% reported pain to interfere with their job. Figure 1 shows the functional limitation, with the majority achieving only limited fitness (49%). It should be noted that two patients (one footballer, one rugby player) still classified themselves as essentially fully fit but were still troubled sufficiently by symptoms to want operative intervention. Most patients (70%) had tried physiotherapy preoperatively, with no improvement in their symptoms, and 52% required regular analgesia (paracetamol, codeine, tramadol or non-steroidal anti-inflammatory drugs).

Functional limitation pre- and postoperatively (p<0.001).
Preoperative characteristics and symptomatology of sportsmen/women undergoing surgery
Postoperative recovery
There were no perioperative complications or long-term complications such as haematoma, serous formation or wound infection.
Postoperatively, patients were mobilising freely at a median of 1 day (range 1–4 days) and were able to perform household chores at a median of 2 days (range 1–5 days). Returning to light training took a median of 1 week (range 0.5–6 weeks) and full training 3 weeks (range 0.5–12 weeks). Patients had returned to playing sport competitively by a median of 4 weeks postoperatively (range 1–12 weeks), although it should be noted that three operations were performed in the “off” season. Seventy-four per cent were able to undertake full training and considered themselves match-fit by 4 weeks. Regular analgesia was required after the first postoperative day in 48% of patients for a median of 2 days (range 2–28 days).
At follow-up, 73% of patients reported no symptoms. Of the remaining patients, two reported symptoms frequently after playing, four reported symptoms frequently after training, 10 occasionally after playing, four occasionally after training, one on coughing/sneezing and one getting out of the car/bed (fig 2). Postoperative pain severity score was a median of 0 (range 0–8) for the entire group (fig 3). Two patients reported no change in severity of symptoms, but reduced frequency of occurrence, and two patients reported no change in symptoms following surgery. Only one patient had not returned to playing sport at follow-up. Importantly, no patient reported deterioration in symptoms following surgery. The median change in pain scores between pre- and postoperation was 7 (0–10). Eighty-eight per cent of patients had returned to full fitness following the operation (fig 1). There was a highly significant improvement in frequency of pain, severity of pain, and functional limitation following surgery (p<0.001, p = 0.005, p<0.001, respectively). Overall, 97% of patients reported that the operation had improved their symptoms and would recommend the procedure to a colleague/team mate.

Frequency of symptoms in all patients preoperatively and at follow-up (p<0.001).
{kind=link}
{kind=link}
{kind=link}
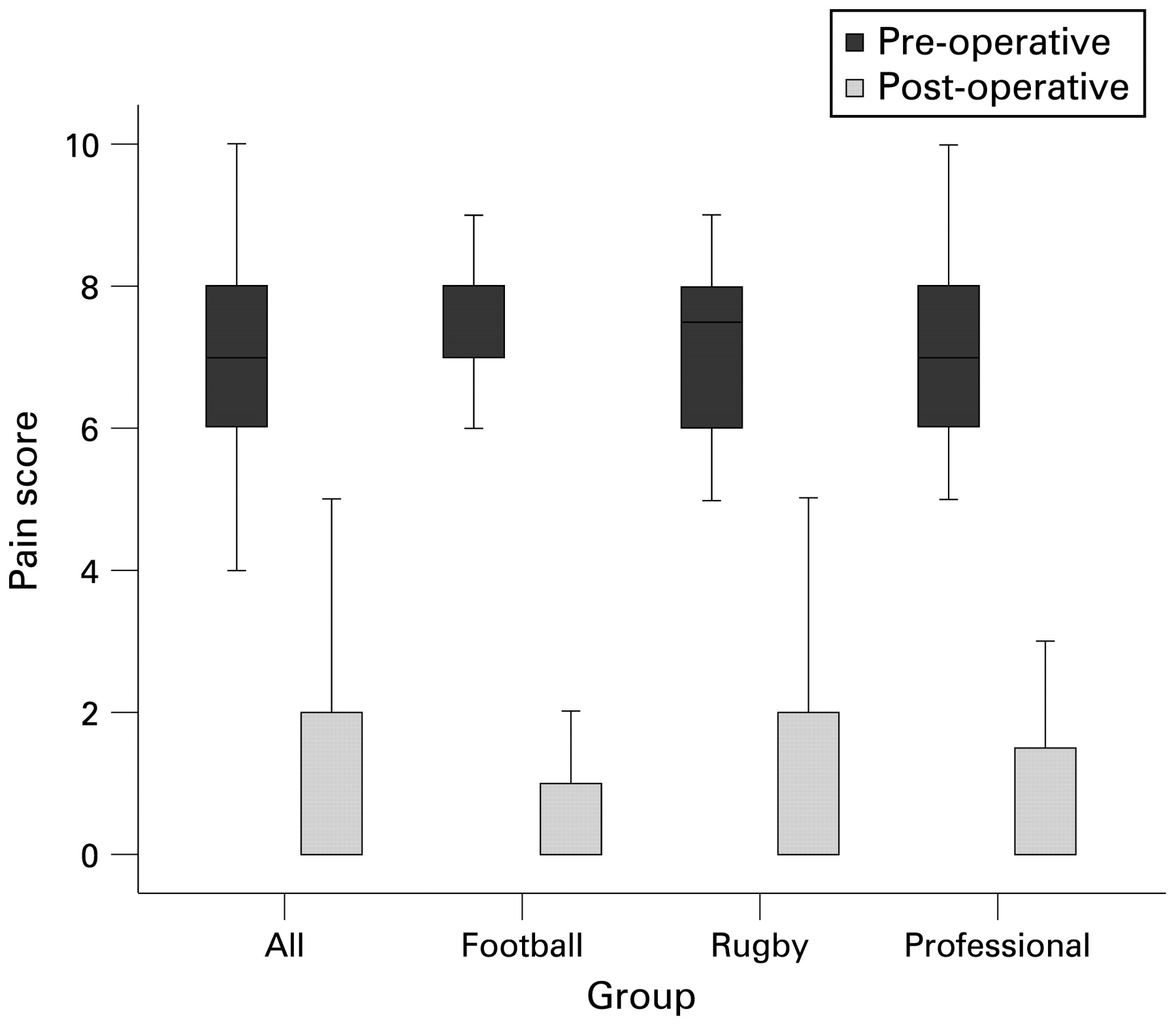
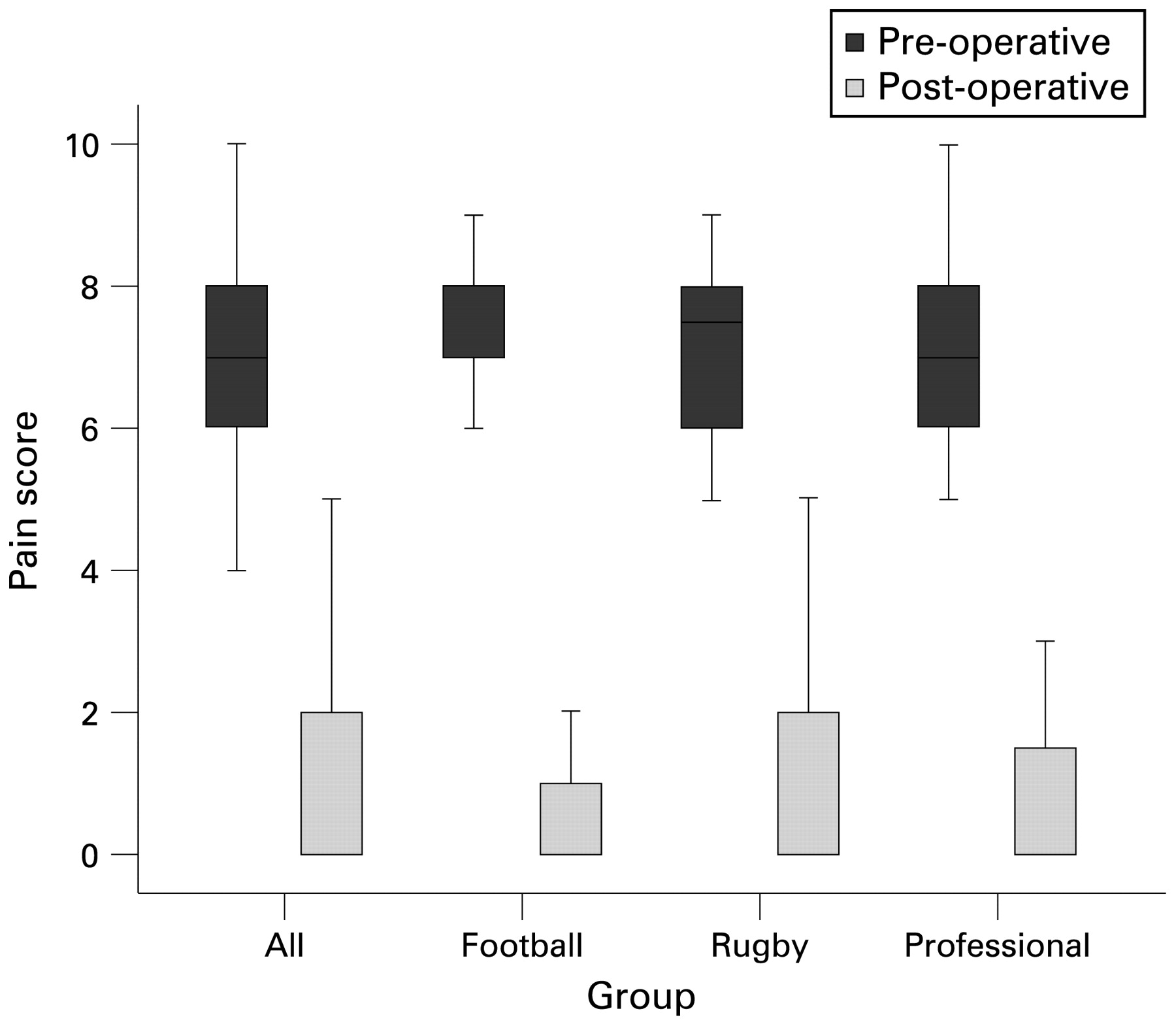
Symptom severity score pre- and postoperatively in all patients (p = 0.005), football players (p<0.001), rugby players (p<0.001) and professional sportsmen (p<0.001).
Footballers
The preoperative characteristics for footballers are given in table 1. Postoperatively, light training was resumed at a median of 2 weeks (range 0.5–6 weeks), full training at 3 weeks (1–12 weeks) and competitive playing at 4 weeks (1.5–12 weeks). Seventy-four per cent of patients reported no symptoms at follow-up, and 88% reported return to full fitness. There were highly significant improvements in frequency of pain, severity of pain and functional limitation following surgery (p<0.001 all cases).
Rugby players
The preoperative characteristics for rugby players are given in table 1. Postoperatively, light training was resumed at a median of 1 week (range 0.5–6 weeks), full training at 2 weeks (1–8 weeks) and competitive playing at 4 weeks (2–10 weeks). Seventy-six per cent of patients reported no symptoms at follow-up, and 90% reported return to full fitness. There were highly significant improvements in frequency of pain, severity of pain and functional limitation following surgery (p<0.001 all cases).
Professional sportsmen
The preoperative characteristics for the professional sportsmen are given in table 1. Postoperatively, light training was resumed at a median of 1 week (range 0.5–6 weeks), full training at 2 weeks (0.5–8 weeks) and competitive playing at 3 weeks (1–10 weeks), but again it should be noted that three players had operations performed in the “off-season.” Seventy-eight per cent of this group reported no symptoms at follow-up, with only one person (2.7%) continuing to experience pain frequently after playing sport. Eighty-four per cent of the 37 professional sportsmen were able to undertake full training and considered themselves match-fit by 4 weeks. All except one patient (97%) reported a return to full fitness at follow-up, and all of these reported that the operation had improved their symptoms and that they would recommend it to a colleague/team mate with similar symptoms. There were highly significant improvements in frequency of pain, severity of pain and functional limitation following surgery (p<0.001 all cases).
Discussion
There is no consensus in the literature concerning the surgical management of sportsmen with chronic groin pain. Various surgical approaches to groin pain have been described, including inguinal hernia repair, with or with mesh insertion,3910111213141516 laparoscopic TEP17181920 and TAPP8202122 hernia repairs, rectus abdominus muscle reattachment627 and adductor tenotomy.152427 The results of this study compare favourably with results in the literature—overall 97% of patients in this cohort reported improvement in symptoms with the procedure, with 99% having returned to sporting activity. The literature reports rates of 63–95% returning to sporting activity following surgical intervention. Our patients returned to playing competitively a median of 4 weeks following surgery. This is shorter than the many studies in the literature, ranging from 4 weeks to 6 months following surgery.
Laparoscopic hernia surgery has been shown to be associated with short hospital stay, improved postoperative pain and improved convalescence.18192021222324252627282930 It also has the theoretical advantage that the posterior position of the mesh behind the conjoint tendon and pubic bone should create a stronger repair than open surgery with anterior mesh placement. Several series have explored the benefits of laparoscopic hernia repair as a treatment modality in athletes with chronic groin pain.8171819202122 Postoperative results range from 100% returning to sporting activities at 4 weeks to 93% within 3 months. In the current series, 74% had returned to “match-fitness” within 4 weeks of operation. Our series of 73 patients is larger than most previously reported laparoscopic series; four of these series report cohorts of 15 patients or less.18202122 Differing mixes of sports (ie, football, rugby, Australian rules football, etc) and variations in definitions used hamper reporting and make comparing results between series unreliable—we used return to competitive level as an outcome, whereas others use return to any sporting activity. This is an important consideration when interpreting our prospective data in relation to other published reports. Genitsaris et al reported a large retrospective series of 131 professional athletes who underwent bilateral TAPP for groin pain, with 97% returning to sporting activity within 3 weeks.8 Van Veen et al reported a series of 55 athletes, 38 of whom were professional, who underwent laparoscopic TEP.17 Eighty-eight per cent returned to sporting activity within 8 weeks, and 100% within 3 months. Paajanen et al reported 41 professional athletes undergoing laparoscopic TEP, with 100% having returned to sporting activity at 1 month.19 Two of the smaller reported series report only professional athletes.1821
Professional athletes have improved access to postoperative care including physiotherapy and training programmes, as well as a financial incentive to return to competitive level, and so are more likely to achieve good results. The results of the current study are comparable with the literature, with 84% of the 37 professional sportsmen in the current series returning to sporting activity within 4 weeks. There is a possibility that due to financial incentives, professional athletes may under-report symptoms following surgery. However, all participants were informed in this study that any information supplied by them would be confidential and not fed back to their clubs without their permission. Although this should have helped to improve the reliability of the data, we accept that this cannot be ensured and remains a limitation of this study. However, the majority of other series in the literature utilise similar assessment of outcome making our results comparable.3910111214151617181920212227 Pain-free return to sporting activity is perhaps a more relevant outcome measure; in this study, 73% of patients (78% of professional athletes) were pain-free at follow-up, but few series in the literature report this outcome, giving no means for comparison. Three professional athletes had operations performed in the “off-season.” While this has the potential to introduce bias into the results, it is overall only a small number and is unavoidable within the setting of this study.
Assuming that modern trends in regular exercise and keeping fit continue, this will inevitably mean that the number of non-professional sportsmen presenting with groin pain will increase. This study confirms our previous study23 from the public sector that a laparoscopic inguinal release may benefit a significant number of these patients. It is still not known if the addition of inguinal tenotomy is beneficial or if the results observed are solely due to mesh reinforcement. It is evident from the literature that laparoscopic hernia repair alone certainly does not benefit all patients with chronic groin pain. Indeed, several patients in the current study had already undergone previous hernia repair without benefit. Further intervention to release their ligaments improved their symptoms. A randomised-controlled trial of laparoscopic hernia repair versus hernia repair and release would be necessary to resolve this.
In conclusion, this study shows that the release procedure may be effective in the treatment of certain athletes with groin pain. We therefore believe that the symptoms in a subgroup of athletes with groin pain relate to the attachment of the ligaments to the pubic tubercle and that laparoscopic release of these ligaments is a promising operation to improve their symptoms without any compromise to their functional ability.
REFERENCES
Footnotes
Competing interests None.
Patient consent Obtained.