Article Text

Abstract
Both structural and non-structural components can contribute to shoulder instability. Classification and therefore management must recognise these factors to achieve functional stability. This paper discusses a classification system proposing three types of shoulder instability recognising the structural and non-structural components and that a continuum exists between pathologies. Structural causes can be addressed with surgical intervention, but non-structural causes such as altered neuromuscular control within the rotator cuff should be addressed conservatively. The purpose of this article is to describe the types of instability and guide appropriate management, helping to avoid surgery in inappropriate cases and ensure that effective rehabilitation has been achieved.
Statistics from Altmetric.com
Introduction
Shoulder instability is a symptomatic abnormal motion of the glenohumeral joint (GHJ), which can present as pain or a sense of displacement (subluxation or dislocation).1 The shoulder is the most mobile joint in the body and therefore susceptible to instability.2 3 Approximately 10% of all athletic injuries are shoulder injuries.4 Ninety-six per cent of shoulder dislocations are attributed to a traumatic event, and 4% are atraumatic due to minor injury or repetitive use. Following injury, patients may develop both structural and non-structural components of instability, which must be recognised if management is to be successful.
Classification
For symptoms to occur, there has to be a disturbance of one or more of the following factors, in isolation or together:
the capsulolabral complex and its proprioceptive mechanism;
the rotator cuff;
the surface arc or area of contact between the glenoid and humeral head;
the central/peripheral nervous system.
The pathologies causing instability comprise structural (rotator cuff, surface area of contact, capsulolabral complex) and non-structural (central and peripheral nervous system) elements.1 The structural elements may be congenitally abnormal, comprise abnormal collagen, acquired microtraumatic lesions over time (atraumatic structural) or be damaged by extrinsic force (traumatic structural). The non-structural elements can be congenitally abnormal or acquired over time as perturbations of neuromuscular control.
The concept of instability (which may change over time) being caused by a combination of structural (traumatic and atraumatic) and neurological system disturbances has led to the classification of instability as a continuum of pathologies, which can be graphically displayed as a triangle (figure 1).1 The polar pathologies are labelled type I (traumatic instability), type II (atraumatic instability) and type III (neurological dysfunctional or musclepatterning). Polar groups I and II and the axis I–II, representing the spectrum between the two poles, correspond to the TUBS-AMBRI classification.5 This allows for a spectrum of structural shoulder pathology but does not admit those shoulders in which there is a neurological/muscle patterning cause for the instability. Direction of instability is not as relevant to effective management as whether the instability is structural, non-structural or both.

Stanmore classification of shoulder instability.
Clinical Assessment
An accurate history and thorough examination is the foundation on which to manage patients. It is important to elicit the mechanism of injury and in particular the level of external trauma applied at the onset of the condition. Significant extrinsic trauma points the clinician to consider a structural element to the instability (I–II axis of the triangle), while non-significant trauma, insidious onset or volitional ability to recreate the displacement indicates a more non-structural cause (II–III axis).
Examination
As the clinical syndrome of instability can be due to a disturbance of the capsulolabral complex, muscular control and central/peripheral nervous systems, a thorough clinical examination of the shoulder must also include general posture, tests for global laxity, scapular dyskinesis, proprioception and stability in the entire kinetic chain. Specific tests for laxity of the shoulder (eg, the sulcus test) are not diagnostic for instability unless the patient has recognisable symptoms during the provocative manoeuvres. Of greater diagnostic value are the anterior and posterior instability tests and tests used to detect rotator cuff integrity to help find a structural element to the instability.6
Polar group I (traumatic structural instability)
Polar I (traumatic-structural) essentially will present with positive apprehension, most commonly in an anterior direction, and associated weakness in the rotator cuff, particularly the subscapularis with deficits on either the belly press or modified lift off tests.6 Global posture, single leg balance and scapular control are often undisturbed, indicating that the instability is primarily due to a disruption in the capsulolabral complex. As cases travel toward either the type II or III poles, patients begin to exhibit signs of poor scapular control, abnormal muscle activation, altered trunk stability and balance, indicating non-structural comorbidity.
Imaging is useful in those cases suspected to have a structural cause (types I and II). This can be achieved by magnetic resonance arthrography (MRA) and/or diagnostic arthroscopy. These are complementary, not alternative, techniques. MRA is useful to look for capsular detachments, bony defects and the bulk and quality of rotator cuff muscles, particularly subscapularis and infraspinatus. Arthroscopy is useful to look for the subtleties of internal lesions of occult instability, such as bicipital and deep surface cuff lesions, soft tissue Broca defects, internal impingement and external impingement lesions.
Polar group II (atraumatic structural instability)
Polar II patients will commonly exhibit a positive anterior apprehension test with signs of increased capsular laxity: excessive external rotation and a sulcus sign. There may also be an associated glenohumeral internal rotation deficit (GIRD). This combination of excessive external rotation and a GIRD is often seen in the overhead athlete secondary to overuse, and creates the syndromes of internal impingement. The abnormal anterior translation of the GHJ within this group can be due to a combination of several factors: excessive anterior capsular laxity, scapular dyskinesis, tight posterior capsule, muscular imbalance (increased ratio of internal rotator/external rotator strength) and congenital labral pathology.7
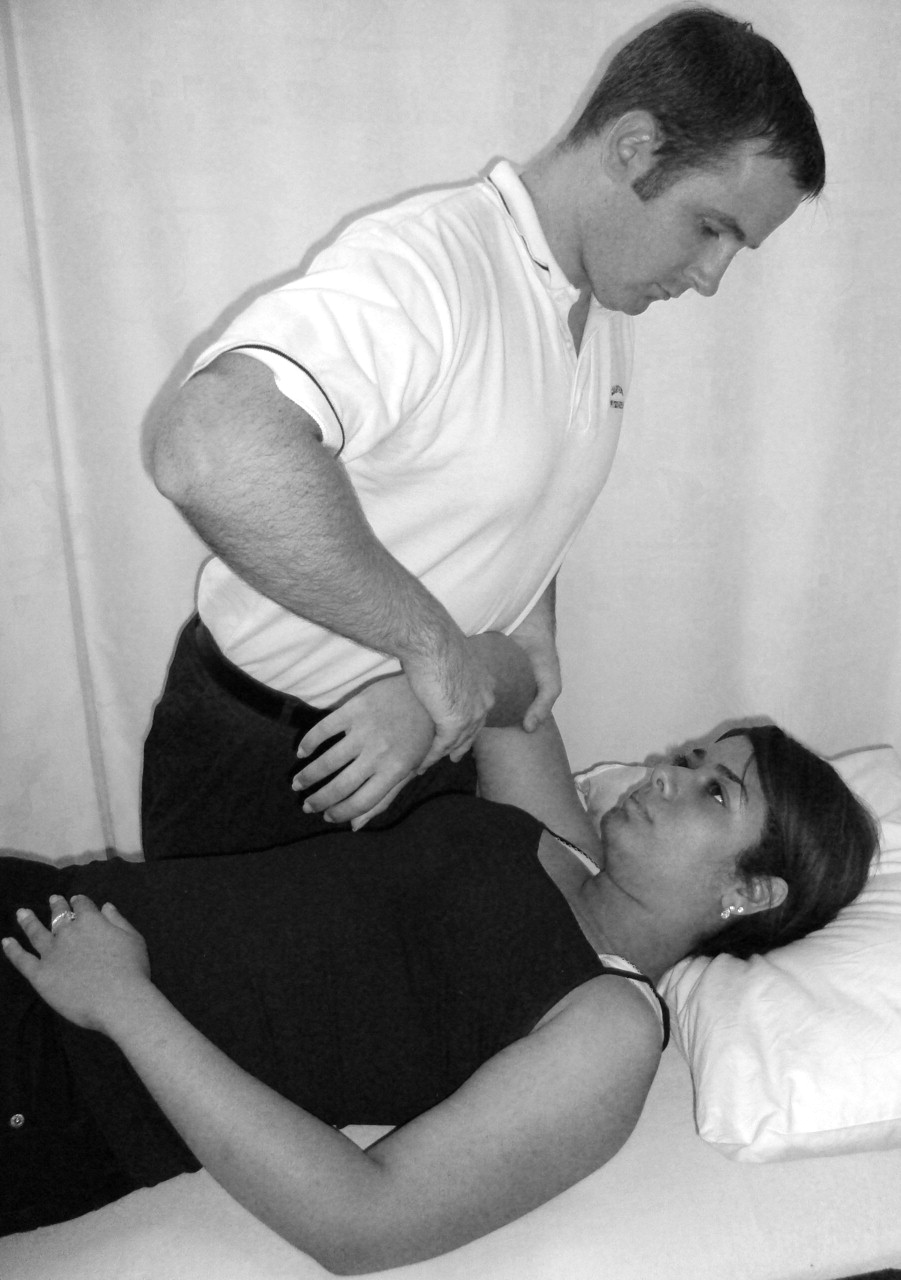
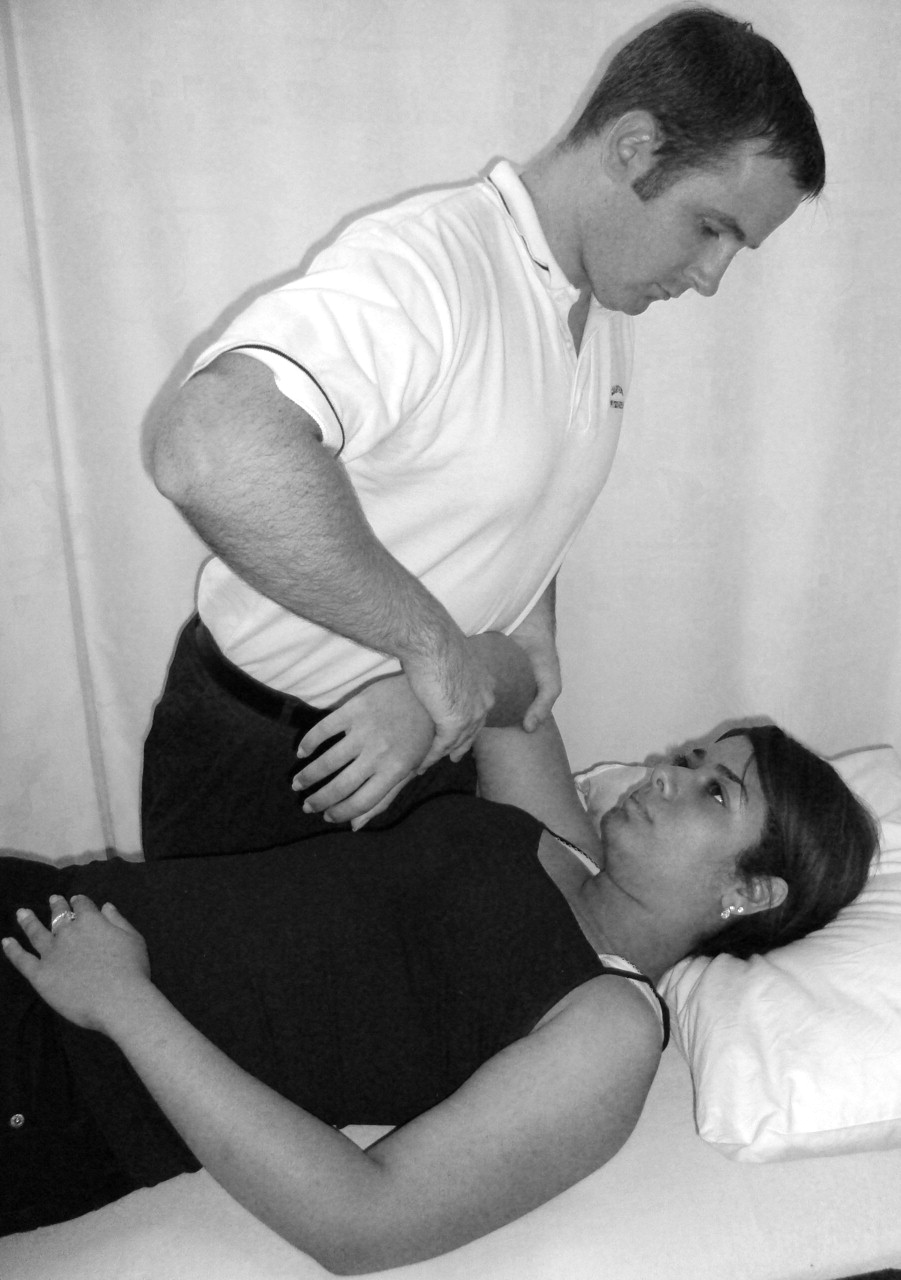
Assessing active and passive glenohumeral rotation at 90° abduction will help to detect scapular instability, tight posterior structures and rotator cuff insufficiency. The dynamic rotary stability test can be used to assess the rotator cuff's ability to maintain the humeral head on the glenoid through the arc of rotation.8 The test can be performed sitting or lying by monitoring translation of the humeral head and observing any abnormal scapular movements, indicating abnormal muscular control (figure 2).

Dynamic rotary stability test.
A GIRD secondary to tight posterior structures is detected by testing passive internal rotation with the scapula stabilised. A deficit of more than 25° of internal rotation in the throwing arm compared with the non-throwing side indicates a significant restriction which alters the centring of the humeral head, further creating anterior capsular laxity.7
Dynamic observation for scapular winging both in ascent and descent is essential as well as observing for any scapular winging in weight-bearing positions.9 Scapular dyskinesis following repetition may indicate fatigue in the external rotators. If this is corrected by the patient resisting an external rotation pressure exerted by the examiner, this may indicate that the primary problem is within the endurance of the external rotators, while the scapula instability is secondary to this.10 Clinical experience suggests that scapular dyskinesis in weight-bearing positions tends to indicate this is secondary to overactivation of the pectoral muscles and decreased trunk stability.
Lastly, global assessment of posture and the kinetic chain should be completed. Perturbation of either may create muscular imbalances more proximally at the shoulder girdle but also contribute to abnormal proprioception along the chain affecting central control.11 Patients may present deceptively with good posture but if further challenged in different positions, for example, single leg balance or four point kneeling, problems with trunk and scapular stability become more apparent.12 In addition, postures may vary dependent on sport. For example, swimmers may stand with more protracted downwardly rotated scapulae indicating an imbalance of the pectoral muscles over the scapular stabilising muscles. The corkscrew test can be clinically useful and quick to assess problems in lower-limb and trunk stability, which may then warrant further detailed evaluation. The test is assessed by asking the patient to perform a single leg squat, if the patient is seen to ‘corkscrew,’ that is, twisting at the knee and hip the test is positive, it is useful to test both sides, dysfunction is more commonly seen on the contralateral leg to the throwing shoulder.13
Polar group III (muscle patterning instability)
Muscle-patterning instability comprises aberrant activation of large muscles and simultaneous suppression of the rotator cuff. Thus far, dynamic electromyography (EMG) at a specialist unit has characterised latissimus dorsi, pectoralis major and anterior deltoid among the large muscles, and only infraspinatus of the rotator cuff. Muscle-patterning instability can be clinically obvious in polar group III but may be occult, requiring dynamic EMG for confirmation in type II/III and III/II instabilities.14 15 If abnormal muscle activation appears clinically obvious, either at the onset of motion or during the motion, then the diagnosis has a muscle patterning component (type III). If there is no clinically or electrophysiologically proven aberrant muscle activation then the condition is labelled type II.
Polar III cases are not often seen in general orthopaedic clinical practice, but the prevalence of abnormal muscle patterning as a cause for all types of recurrent shoulder instability at a specialist shoulder unit was 45% of cases.14 The unit also found that type II (structural) cases, where conservative treatment had failed to resolve symptoms and went on to have successful surgery, were those that had corrected preoperatively any abnormal muscle activation or had no demonstrated abnormal muscle patterning on dynamic EMG.16 Ongoing abnormal muscle activation can be sufficient to sublux or displace the shoulder, as a result destroying any surgical repair. Failure to recognise abnormal muscle patterning can therefore be a cause for surgical failure..14 16
Polar III patients will often have a history of ‘party tricking’ the shoulder. This will often occur in the midranges of movement or with the arm dependent by the side indicating a muscular control problem. This volitional ability to displace the shoulder may develop later into an involuntary problem. The dislocations themselves are often painless, but the patients can experience aching, paraesthesia and numbness in the arm. Some cases will develop persistent displacement of the shoulder, indicating ongoing abnormal muscle activation.
It is useful to observe the direction of displacement and any associated abnormal muscle activation. It is also important to observe the resting position of the GHJ prior to movement, to be sure it is not already displaced under the effect of abnormal resting tone in surrounding muscles. A persistently inferiorly displaced GHJ can prove difficult to manage, because this indicates gross inhibition of rotator cuff and deltoid tone, which is likely to be centrally driven (figure 3).

Persistent inferior displacement of the GHJ.
There is often laxity to the GHJ in all directions and generalised hypermobility. Patients typically adopt the sway back posture, a tendency to hyperextend the hips and knees and cause forward displacement of the pelvis.17 This tendency to hang at the extreme of their hypermobile range results in poor core stability and may increase the use of more superficial torque muscles such as latissimus dorsi, having a resultant effect at the shoulder girdle.10 A secondary thoracic kyphosis may develop to compensate for the sway posture. As a result, the scapula adopts a protracted, laterally tilted position.18 The glenoid cavities face downwards and forwards, such that the humeral head ‘hangs’ from the glenoid, further challenging the joint reaction compression force.
Patients with muscle-patterning instability usually present with posterior instability.14 19 20 The dominant pattern of elevation of the arm is in internal rotation (associated with over activity in latissimus dorsi and/or pectoralis major), with resultant or associated inhibition of infraspinatus, lower trapezius, serratus anterior and posterior deltoid. As a result, posterior displacement of the GHJ occurs in ascent with an associated ‘reverse-scapular’ action, as the scapula is prevented from protracting and upwardly rotating in the normal way.20 As the arm descends, there may be an audible click or clunk as the GHJ relocates.
The therapist can assess abnormal tone through palpation and observation of either pectoralis major and minor or latissimus dorsi. Strengthening programmes to the rotator cuff may not always be fruitful in the presence of abnormal tone in these muscles. Poor core stability can influence the superficial torque action of larger global muscles such as latissimus dorsi, creating instability at the shoulder girdle. If posture is corrected, then any strengthening programs performed at the shoulder are more likely to target the appropriate muscles.13 Similar tests used in the type II group to evaluate stability in the kinetic chain should therefore also be used in this group.
Management
Management is guided by weighting the structural and nonstructural causes of instability to gain functional stability. If normal neuromuscular control is to be achieved, there must be integration of the peripheral somatosensory, visual and vestibular afferent input with improved motor control through spinal reflex, brain stem and cognitive programming.21 Principles of rehabilitation will therefore apply across the three groups of instability but there may be more focus on different elements for the polar groups.
Role of surgery
Traumatic anterior structural instability is the most common clinical presentation with a reported recurrence of the instability between 88% and 95% in patients under the age of 20.1 If there is a structural disruption of the capsulolabral complex (eg, a Bankart or SLAP lesion) and the patient is young and returning to contact sport, then surgery is often recommended to avoid reoccurrence.22 This is now more commonly performed arthroscopically, and accelerated rehabilitation programmes postoperatively are returning the athlete back to their sport within 4 months without increasing the risk of failure.23
For polar II patients and those who lie on the II–III axis surgery should only be considered if there is a demonstrable structural component to the instability, that is, bone, cartilage or labral abnormality and after any underlying muscle patterning problem has been corrected. Eighty per cent of type II patients will respond well to a successful programme of rotator cuff strengthening, scapular stability and kinetic chain exercises, often taking up to 6 months. Only those who fail a conservative approach and have associated rotator cuff or capsule-labral pathology should be considered for surgery.14 24 Surgery is contraindicated in a pure polar III group where there is no structural cause. If treatment is unsuccessful in this group, then modification of lifestyle and coping strategies to deal with symptoms are necessary.
Early management: protective phase
Initial management for type I instability is to protect soft tissue structures to allow healing and reduce inflammation. However, this must be balanced against the risk of stiffness, maladaptive postures, muscle wasting and loss of proprioception. Type II and III groups where onset is more insidious do not require periods of immobilisation but need to avoid activities that exacerbate the symptoms of instability, which in turn may encourage faulty or abnormal patterns of movement.
The rotator cuff muscles play a relevant role in the dynamic stability of the GHJ. These muscles are ideally placed to draw the humeral head on to the glenoid and maintain its axis of rotation: the presetting action of the rotator cuff provides the concavity compression required for stability prior to movement.8 25,–,28 Often after injury, this presetting can be lost, particularly if capsuloligamentous structures have been disrupted, thereby altering afferent feedback leading to changes in muscle firing patterns.29
Closed chain exercises facilitate the presetting rotator cuff function enhancing joint stability, stimulating muscular coactivation and proprioception.30,–,33 Initially, rotator cuff exercise should be performed with a fixed base of support and the weight-bearing action on a table or wall encouraging muscular coactivation and scapula stability without increasing shear forces across the shoulder joint.32,–,35
Early submaximal isometric exercises for the rotator cuff should be performed as pain allows and to the exclusion of inappropriate muscle activity for patients with type I or II instability. Subscapularis plays a role in providing anterior GHJ stability.36 But as it acts as an internal rotator, its early activation needs to be isolated from pectoralis major. The belly press test, used to test the integrity of subscapularis can be modified for this purpose.37 The patient places the hand onto a pillow placed on the belly, with the elbow out to the side and the unaffected hand monitors activation of pectoralis major and any anterior translation of the GHJ. The patient is encouraged to appropriately set and align the scapula as they push gently into the pillow (submaximal contraction) maintaining the elbow position and avoiding recruitment of pectoralis major as if pushing from the back of the shoulder. They are encouraged to hold the contraction for 5–10 s and repeat as comfort allows. The use of a pressure biofeedback unit can be helpful to gauge the amount of pressure being applied to monitor progress and provide feedback on the level of pressure that should be exerted (figure 4).

Belly press test with use of the pressure biofeedback.
Type III patients and some type II with excessive capsular laxity are unable to gain selective cuff recruitment on the background of poor core stability and fixation of the global large muscles. These patients respond better when postural tone is increased such as sitting on a Swiss ball, standing on one leg or standing on a wobble board.10 38 Increasing tone within the postural muscles then reduces the action of muscles such as latissimus dorsi and places the scapula and GHJ in normal positions to then encourage the deep stabilising muscles to work. For those type III patients with posterior instability, isometric external rotation is required for stability.
In some type III cases, inhibition of overactive muscles is not always achieved by working at the core, and patients have to be selectively taught to relax muscles. This can be achieved with use of biofeedback equipment or encouraging the patient to feel the abnormal tone in the muscle and to try and move the hand or arm without the inappropriate muscle working. The patient should be encouraged to do this several times repeatedly in the day in order to relearn a movement pattern.
Early feedback of posture and shoulder girdle position is important for all groups to avoid inappropriate patterning and strengthening. Postural tape and mirrors can be invaluable in providing correct sensory feedback facilitating correct muscle activation (figure 5).39,–,41 Facilitation of the scapula via tactile feedback through protraction/retraction/elevation/depression enables the patient to dissociate the scapula from the trunk and appreciate where their scapula is in space.38

Use of tape for postural feedback.
Intermediate phase
Following early cuff activation and good postural alignment, exercises to promote muscle balance and endurance should then be encouraged through the full range of movement. Patients who have developed a GIRD secondary to tight posterior capsule must regain the passive range to internal rotation to achieve balanced external and internal rotation strength, predominantly type II instability. Self stretching can be difficult for exercises such as the sleeper-stretch; a more effective stretch is performed by the therapist with the arm in 90° flexion adding in components of internal rotation and adduction applying a downward, caudal translation through the elbow, similar to a posterior draw stress (figure 6). This must clearly be avoided if there is a risk of posterior instability and should be graded as pain allows.
Posterior capsule stretch.
Once good passive range is achieved, the cuff should then be encouraged to activate through the range for all types of instability. The dynamic rotary stability test already mentioned earlier could be useful to start early rotator cuff rehabilitation with the limb supported. The patient can place the nonaffected hand on the front of the shoulder for proprioceptive feedback, trying to maintain good scapula and GHJ control. Light weights can be added. The use of a weighted stick is often useful to act as a moment force encouraging the activation of biceps, another important GHJ stabiliser (figure 7). By placing the weight medial to the hand and maintaining the level of the stick as the arm is internally and externally rotated, either concentric or eccentric biceps activity is encouraged. Such exercises are particularly useful in managing the atraumatic group. Progression of rotator cuff exercises can then be performed in prone or side lying against the effect of gravity (figure 8). Prone lying can be advantageous when strengthening the cuff, as it tends to inhibit the action of pectoralis major and latissimus dorsi. Achieving good active control to internal and external rotation in this position will ensure that the rotator cuff exhibits no lag signs during formal testing.

Rotator cuff and biceps strengthening with a weighted stick.

Strengthening external rotators.
Rehabilitation of the rotator cuff should focus on repetitions rather than increased load: a yellow cliniband is often sufficient for rotator cuff strengthening. In a study where the electromyography activity of infraspinatus and deltoid was analysed during resisted isometric external rotation, low loads of between 10% and 40% maximal voluntary isometric contraction were found to optimise the relative contribution of the infraspinatus.42 This is important particularly to avoid type I and type II patients developing a muscle patterning problem. If exercises are overloaded at inappropriate stages of the rehabilitation, patients may have a tendency to activate inappropriate muscles, for example, a subject with traumatic anterior instability may compensate by using pectoralis major rather than subscapularis, thus creating a risk of developing recurrent instability of a type I/III character.
Although it is often correct to teach isotonic cuff exercises with the arm in adduction to the body to avoid over recruitment of deltoid for patients with impingement, in patients with an inferior element of instability (type II and III) it may be more preferable to encourage recruitment of deltoid with the rotator cuff. Hence, resistance in slight abduction is applied to assist better superior relocation of the humeral head. In addition, avoiding adduction of the shoulder may further inhibit the action of pectoralis major and latissimus dorsi. Another effective exercise to encourage recruitment of the external rotators through range is for the patient to stand sideways to a wall and slide the effective arm up the wall resisting external rotation. In type III patients, the use of biofeedback can help the patient to recruit infraspinatus in a pattern of external rotation while reducing the electromyographic activity of latissimus dorsi (figure 9).

Biofeedback to infraspinatus and latissimus dorsi.
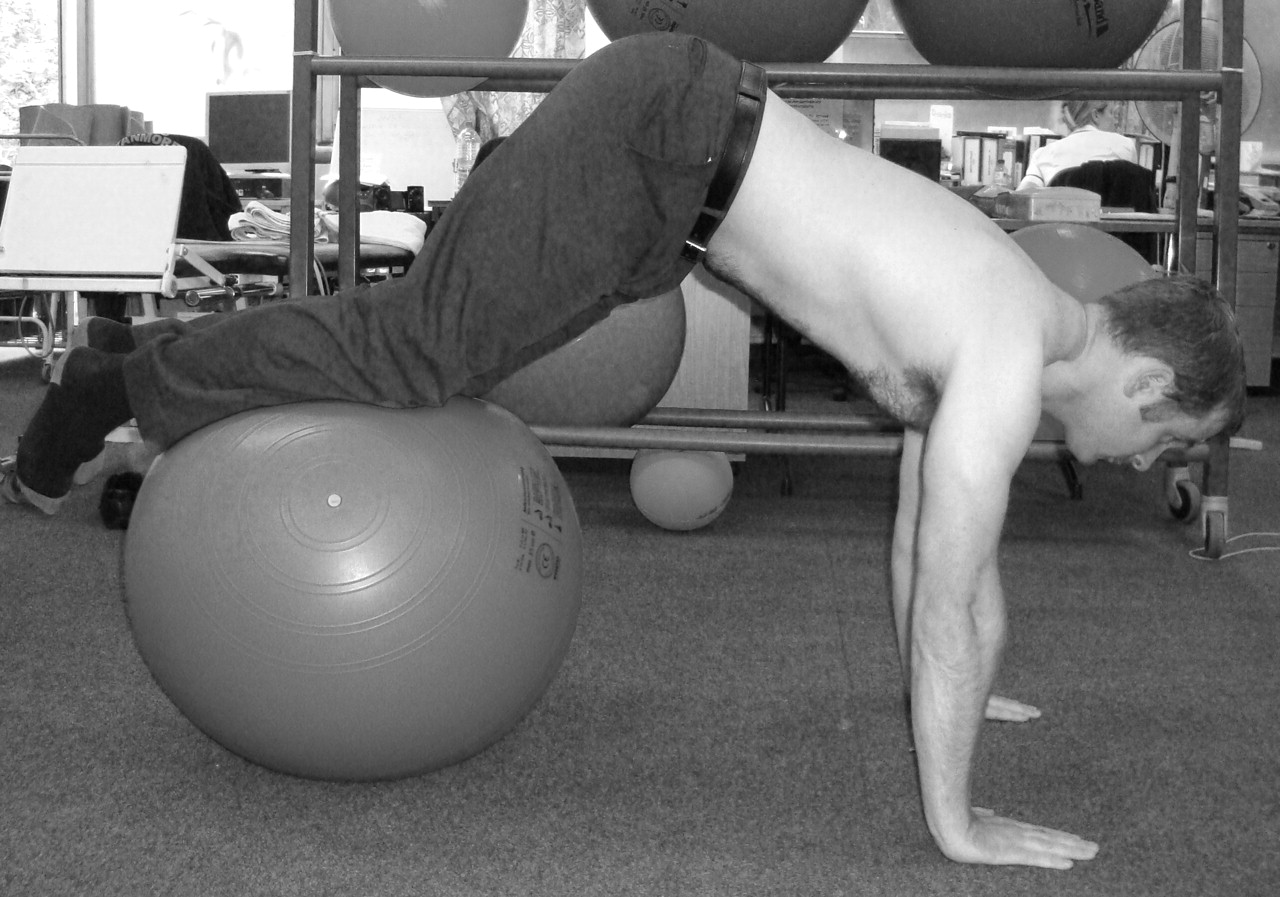
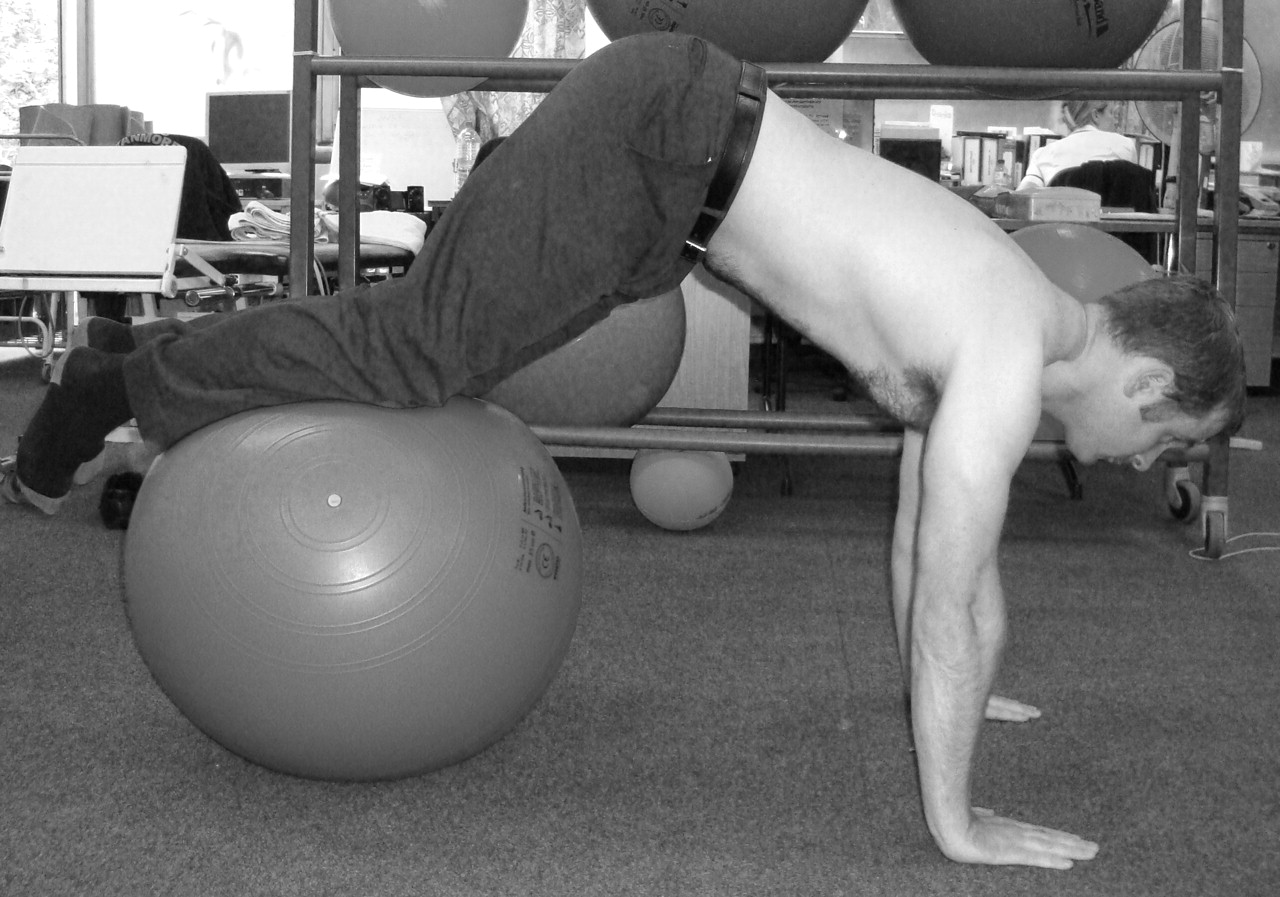
Closed chain exercises can now also be progressed to weight bearing on unstable surfaces such as a Swiss ball, thus enhancing neuromuscular control at a reflex level (figure 10).38 Exercises can be interchanged by placing the unstable base either end of the kinetic chain. Placing the unstable base directly under the upper limbs may enhance neuromuscular control; the altering perturbation will challenge proprioception and improve joint position sense. It should be noted that studies have found little difference in upper-extremity muscle activity when using an unstable base.43 44 Consequently, an unstable base under the upper limbs for improving strength is debatable, but it may benefit joint proprioception. Progression of closed chain exercises in the type III instability must be approached with caution, as these patients may still have a tendency to overfixate with inappropriate muscles if core stability is still poor. Placing the ball under the lower limbs rather than the upper limbs to enhance core stability is more suitable: an example of a relevant activity is the squat thrust exercise (figure 11).

Closed chain exercises on a Swiss ball.
Squat-thrust exercise.
Advanced phase: functional rehabilitation
End-stage rehabilitation focuses on continued strength and endurance, and must be about retraining patterns of movement biased towards functional tasks. Repetition, speed and load may be varied in relation to the desired task, facilitating feedforward processing.21 Dynamic stabilisation can be challenged by performing pushups or tricep dips on a ball, throwing and catching a ball. Plyometric drills can help to transfer energy from the legs and trunk to the upper limbs such as two-hand chest passes, overhead soccer throw and side-to-side throws.30 Light-weight Swiss balls or bouncing balls off trampets can be used to increase speed and endurance, and medicine balls can be used for strength training. Proprioceptive neuromuscular facilitation is useful to gain stability and control into functional patterns, strengthening through range. Global upper-limb strengthening can be incorporated with kinetic chain exercises such as stepups and single leg squats to train patterns of movement rather than isolated muscles.
An exercise found to be clinically effective for aiding proprioception is the side lying plank: the affected arm points towards the ceiling at 90° to the body, and the patient is encouraged to balance a ball or place and hold the hand in space with the eyes closed, thus helping to retrain joint position sense (figure 12). Activities should now be more sportspecific with goal-orientated tasks, as these have been shown to be effective in cognitive motor retraining.45 Examples can be throwing at a specific target, bouncing a ball around an obstacle course or shooting into a basketball/netball hoop. It is vital that the patient regains five key components prior to returning to their sport; flexibility, strength, balance, proprioception and of course confidence. If confidence is still lacking, the athlete is at risk of compensating with abnormal movement faults, increasing their risk of reinjury and instability.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Side-lying plank exercise.
The length of a rehabilitation programme will vary between individuals’ and the type of instability. Type I instability can be successfully rehabilitated following surgical intervention with return to sport averaging 4 months: this is dependent on the type of surgery (open or arthroscopic) and the integrity of the repair. Type II and III patients require on average 6 months of rehabilitation, acknowledging that recurrence can occur with changes in training or involvement in a new sport where the neuromuscular system is rechallenged. In addition, younger individuals (predominantly in the type III group) can experience growth spurts that alter posture and therefore neuromuscular control, thus increasing the risk of instability. Such individuals have good outcomes if managed quickly with corrective posture and scapula positioning.
Lastly, the specific technique of the sporting activity should be analysed in association with coaches wherever possible, to determine if the sport technique was itself a predisposing cause of the instability. Assessing and utilising the entire kinetic chain in a throw action or a swimming stroke is less likely to promote inappropriate muscle activation at the shoulder girdle and prevent recurrent symptoms. Video footage is now accessible and useful to achieve this in the clinical setting.
Conclusion
Both structural and non-structural elements of instability exist; these are interlinked, and a combined approach to management is required for a successful outcome. The Stanmore classification allows for a continuum between pathologies over time and can direct both surgeons and therapists to the roles surgery or conservative management may have. For those cases with a clear structural component and normal neuromuscular control (type I, type I/II), surgery is often required for the patient to return to high-level sport. Type II cases may present with structural changes demonstrated on arthroscopy, but these may be secondary to non-structural causes and therefore should initially be managed conservatively, focusing on rotator cuff control and endurance. Patients with signs of abnormal muscle activation (types II/III and III/II) must be managed with core stability exercises and good postural alignment prior to selective rotator cuff activation. Only when the inappropriate activation is corrected can surgery be considered. Surgery is contraindicated in polar III cases: there is an increased risk of degenerative disease and failure of rehabilitation if surgery is performed.
References
Footnotes
-
Patient consent Obtained.
-
Competing interests None.
-
Provenance and peer review Commissioned; not externally peer reviewed.
Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.