Article Text

Abstract
Objective How to organise an appropriate team to provide quality dental care during the Olympic Games has become an important consideration for each successive host country. The aims of this study were to document dental services provided at the Olympic Games and to provide data for planning future events.
Set-up of the dental care department There were six dental chairs in six independent treatment rooms, one technical laboratory, a sterilising room and an x-ray room equipped with one digital panoramic screening machine and one intraoral x-ray machine in the polyclinic in the Olympic Village in Beijing. Shifts comprised 80 dentists and 28 nurses who were organised into three shifts working from 08:00 until 23:00.
Results In the 2008 Olympic Games, there were 1607 cases involving 1126 patients requiring dental care: 795 cases from 516 athletes; 483 cases from 370 coaches and other staff; and 99 cases from volunteers. Endodontic treatments, permanent fillings, oral hygiene, mouthguards and treatment of pericoronitis were the most frequent procedures in dental care. The Mouthguard Service was extremely popular and well utilised. 122 athletes received new custom-made mouthguards in Beijing.
Conclusions As the utilisation of the dental service grows, and the burden of providing care for such a large cohort increases, a well-organised dental team becomes increasingly important. More general-practice dentists were needed in the team. Different kinds of specialist were suggested for working in the team—for example, oral and maxillofacial surgeons, sport dentists for mouthguards and endodontists.
Statistics from Altmetric.com
Background
The Olympic games is a worldwide sports event which hosts more than 10 000 athletes from over 200 countries who come together in one host country to take part in the games over a period of 2 weeks. Injuries and cases of heat-related illness, even sudden death, among participants in the Olympic Games are the main focus of medical research concerning Olympic Games.1 However, it is found that more and more participants seek dental care during the Olympic Games.2,–,4 Besides physiotherapy, dental care becomes the second busiest service provided in the polyclinic of the Olympic Village (OLV).5 It is very important to estimate how many athletes and/or coaches may need dental care during the period of the Games; which days are the peak time of the dental care during the period; and what kind of dental treatment might be required. All of this information is useful for the host country that will organise the upcoming Olympic Games.4 6 7 With this information, the International Olympic Committee (IOC) and organising committee can estimate how many dentists may be needed and what kind of specialists would be required. As there are many questions, how to organise a suitably sized dental team is always a question that should be answered prior to the Olympic Games.8 9 The aim of this study is to document dental services provided at the Olympic Games in 2008 in Beijing and to provide data for planning future events.
Set-up of the Dental Care Department at the 2008 Olympic Games in Beijing
There were six dental chairs in six independent treatment rooms in the polyclinic in the OLV in Beijing. There was also an x-ray room equipped with one digital panoramic screening machine and one x-ray machine. The x-rays were printed out as a film or sent to the different rooms to display on a monitor for the patient to view. One technical laboratory, a store room for all the dental materials and a sterilising room were on the same floor. A reception desk was located between the treatment rooms and x-ray room. In Beijing, the OLV was open from 20 July 2008, 19 days before the opening ceremony, until 27 August 2008 (40 days all total). Dental care in the polyclinic was open from 08:00 until 23:00. During this period, 80 dentists and 28 nurses were organised into three shifts. All the dentists and nurses were from 12 university hospitals in Beijing. A computer network (LAN) connected all six treatment rooms, reception desk, x-ray room and the office of the chief dentist.
Data collection
There were four groups that received dental service in the polyclinic:
all the athletes who were registered as ‘athletes’;
coaches, team doctors and other staff in each national delegation were recorded as ‘others’;
dignitaries of the IOC and NOC were recorded as ‘VIP’;
volunteers who worked in the OLV were recorded as ‘volunteer.’
There were three kinds of documents for each participant:
reception card (RCd) included ID number, age, sex, sporting events, nationality and registration time for dental treatment;
patient's file (PF) of two parts: part 1, a brief-PF, in English, which recorded the findings of the examination, related treatment plan and suggestions; and part 2, a PF of treatment (PF-t), in Chinese, that recorded information about the treatment procedure;
medical encounter form (Med-E) provided by IOC, recorded diagnosis and the treatment(s).
Visiting office procedures
Every participant seeking dental care in the polyclinic was first registered at the dental reception desk. The receptionist created a RCd for the patient. At the same time, a PF was created. The RCd was attached to the PF. The PF was kept at the front desk during the patient's visit. The patients were escorted into the treatment room by a nurse. During this procedure, the nurse kept the PF. After the dental examination or treatment, the dentist filled out the brief findings in the PF in English by hand and completed the Med-E in the computer. The PF was returned to the receptionist by the nurse after the patient's treatment. Every patient was given a copy of the PF. The detail information of treatments was recorded in a PF-t and was kept by the receptionist and then transferred to the office of the chief dentist. The Med-E was sent to the IOC office from the LAN. Each office visit was recorded as one case on the RCd, PF and Med-E, no matter how many teeth were treated.
All these procedures were developed as a guideline for dental services at the Beijing Olympic Games to assist the dental team for the 2008 Olympic Games.6
Analysis of different types of dental treatment was based on teeth numbers recorded on PF-t. For example, endodontic treatment for one tooth might have required two visits by the athlete. The number of endodontic treatments for this athlete was recorded as one, and the number of recorded visits was two. Also, if the dentist filled two teeth for an athlete in one visit, the treatment was recorded as two, and the visits recorded as one.
The total number of participants who required dental care was based on the number of PFs. For example, if a participant came in for dental care three times, the number of RCds and Med-Es was recorded as three cases, and the PF-t also showed as three visits. However, the participant had only one PF, no matter how many times he/she visited. Thus, the number of PFs actually reflects the number of patients who received dental care.
Results
The numbers of patients by identification (athletes, others, VIP or volunteer) are listed in table 1. According to PF (rank 3 of table 1), there were 1607 cases from 1126 participants for dental care. Of these, there were 795 cases from 516 athletes; 483 cases from 370 coaches and other staff, and 99 cases from volunteers. There were 115 cases without a registration number, but their treatment was recorded in the PF. The difference of numbers among RCd, Med-E and PF is shown in table 1.
Dental service in the 2008 Olympic Games
Analyses of different types of dental treatments are represented in table 2. Permanent filling, root-canal treatment, hygiene, treatment for pericoronitis of impacted teeth and provision of new mouthguards were the most frequent procedures in dental care at the Beijing Olympic Games. There were 155 participants who had a dental examination and oral health education. There were 47 cases of tooth extractions. Trauma of soft tissue (in four cases) and trauma of teeth (two cases) were treated. Temporomandibular disorder (TMD) was found and treated in two athletes. Urgent treatment for abscess was undertaken in six cases. Loss of orthodontic clips was found in three cases.
Dental treatments in the 2008 Olympic Games
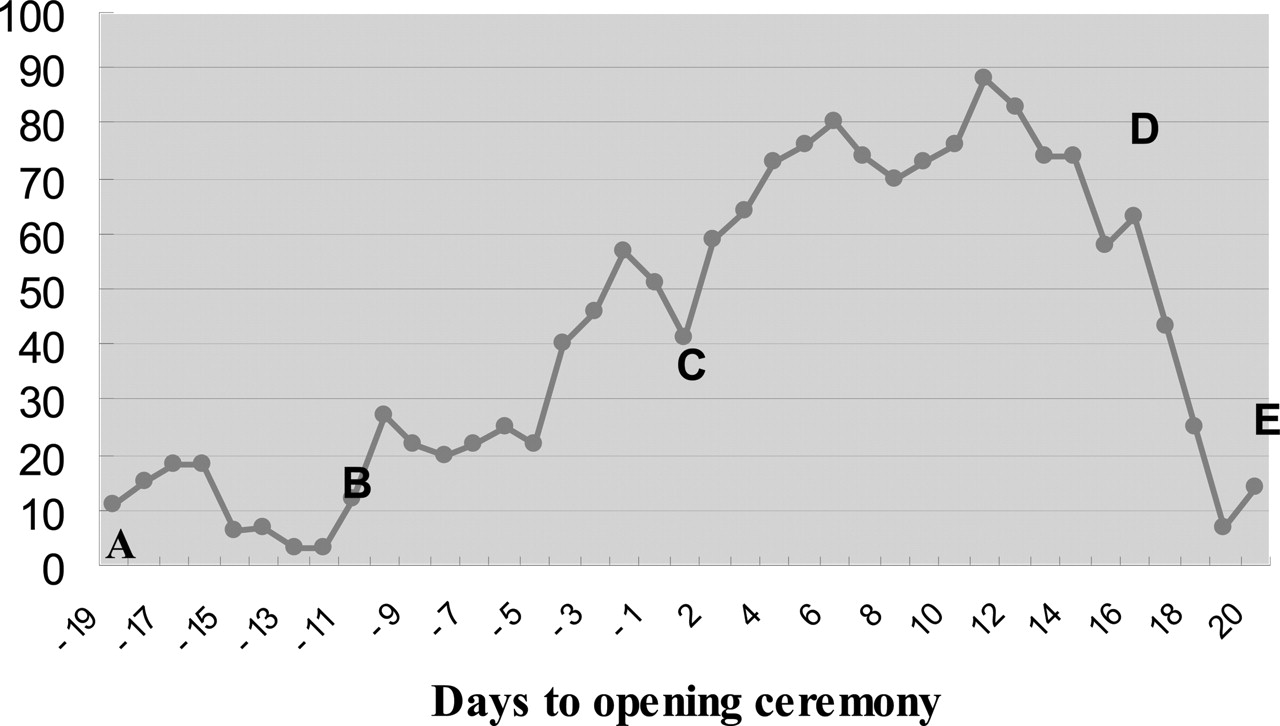
The number of patients treated during each day of the 2008 Olympic Games is outlined in figure 1. The preopening of the OLV (period AB in figure 1) is indicated from 19 to 13 days before the opening ceremony. During this period, there were no athletes or other members of the national team in the Village. There were about 20 participants who received dental care per day in the period prior to the opening of the OLV. The athletes and delegations entered the OLV 12 days before the 2008 Olympic Games opened. It was found that the peak time for dental care was from 3 days before the opening ceremony (−3 days) until 1 day before the closing ceremony (day 16) of the 2008 Olympic Games.
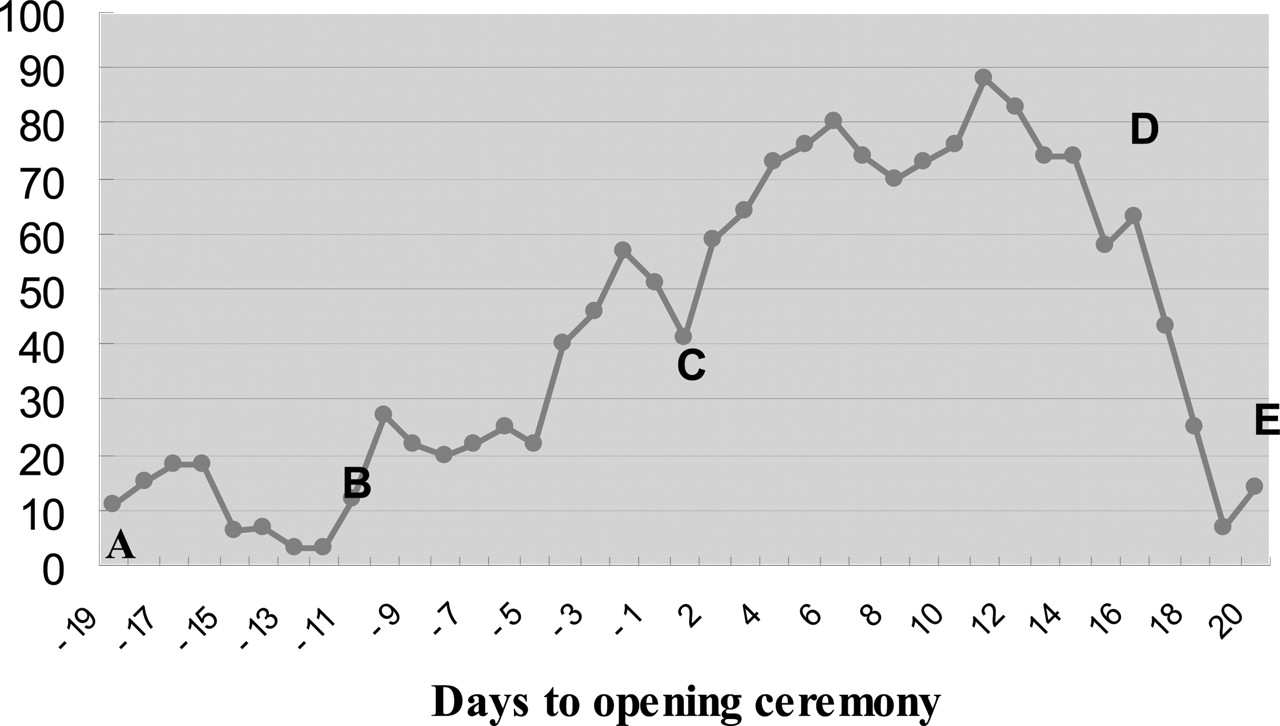
Peak-time analysis of dental services in 2008 Olympic Games. (A) Preopening of Olympic Village—19 days before opening ceremony (−19). (B) Official opening of the Olympic Village—12 days before opening ceremony (−12). (C) Opening ceremony of 2008 Olympic Games on 8 August, −day 1. (D) Closing ceremony of Beijing Olympic Games on the 17th day after the opening ceremony, 24 August 2008. (E) Closing of the Olympic Village on the 20th day after the opening ceremony.
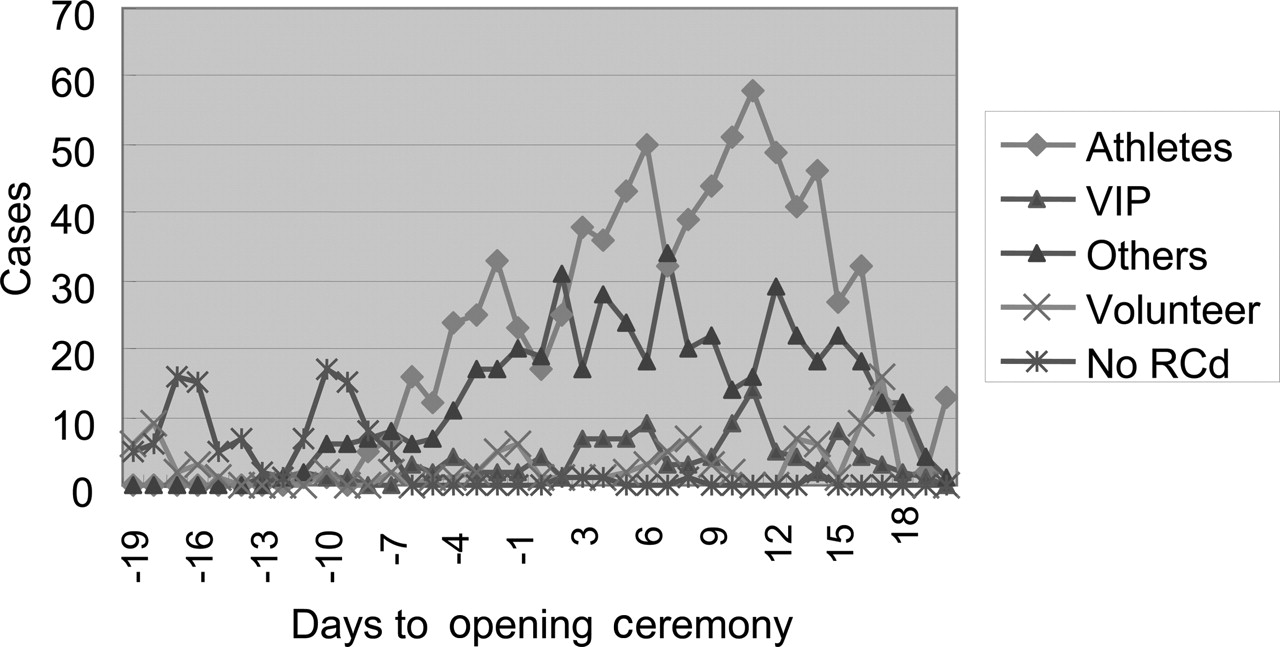
A comparison of the participants by identification is provided in figure 2. All the numbers in this diagram indicate daily cases. The red line shows the changing of daily cases of athletes. The brown line indicates the cases of coaches, team doctors and others in delegations. The purple and green lines illustrate the cases of VIP and volunteers. The blue line shows cases of the participants without a registration card.
{kind=link}
{kind=link}
Different participants searching for dental services in the Beijing Olympic Games.
Discussion
For the host city of the Olympic Games, previous data are very important but not easy to gather exact data
In October 2006, the IOC and the Beijing Olympic Organization Committee began to organise the Dental Health Services of the 2008 Olympic and Paralympic Games. Historically, the host city for the Olympic Games always hopes to offer high-quality medical services for the athletes and other participants. On the other hand, the IOC and organising committee must try not to disturb the medical care services of the host city. In Beijing, one dentist services 6000 people. In order not to overextend a dentist's time and stamina, it is very important to organise a suitably sized dental team for the Olympic Games. The first issue we faced was how to determine the exact number of dental services provided in the 2004 Olympic Games. According to a publication in 2005, there were only about 500 participants seeking dental care in 2004 and about 28 dentists and nurses on the dental team.4 However, the medical and scientific committee of the IOC stated that there were actually nearly 1200 cases from about 700 people who received dental care from about 80 dentists and dental nurses in 2004. The numbers were not the same. After many discussions between the IOC and the Beijing Organization Committee, it was decided that 80 dentists with six dental chairs would be needed to provide dental services for approximately 1600 cases in 2008.6 In May 2008, only 2 months before the Beijing Olympic Games, the final result of the 2004 Olympic dental services was published.10 There were 1400 cases from 650 participants treated by the dental care system of the 2004 Olympic Games. Interestingly, the final number of dental care cases in 2008 (1607 cases, table 1) is similar to that which we had estimated before the Olympic Games.
It should be recognised that the need for dental services may not be easily controlled because dental treatments for one tooth may need two or more visits. Among these numbers, the number of patients may not be as important as the number of cases. The case number is the key to estimating the amount of work by a dentist. For this reason, three documents, RCd, PF and medical encounter, were created per patient in this study. In this way, it was very easy for the dentists, reception nurses and chief dentist to evaluate the work performed during the Olympic Games.
For dental services provided in 2008, all important files (such as RCd, PF and Med-E) were always in the nurse's hands, kept by the receptionist or in the computer. These files always transferred with the patients. In this way, the files were not easily lost. RCd, PF and medical encounter were the main files used to count the case numbers of the patients. It is understandable that the numbers in three files (three rows of table 1) should be the same. However, the case number of medical encounters was over 200 cases less than the numbers from RCd and PF. The reasons for this difference are:
During the period of the preopening of the OLV (‘A–B’ area in figure 1), the system of creating a Med-E was not being utilised. For a host city of the Olympic Games, it is very important for the dentists to administer different treatments to a certain number of patients in the polyclinic before the OLV officially opens. Dental treatment rooms in the polyclinic are a totally new environment for the dentists and nurses. They need practice to acquaint themselves with the new treatment room before they meet real athletes. There were 105 people filling the important role of a volunteer in the Beijing Olympic Games. These volunteers could not be recorded by medical encounter, but the treatment could be recorded by hand in the RCd and PF. These treatments must be taken into account as part of the Olympic dental service. That was the main reason that the number of RCds and PFs was higher than the medical encounter.
During the opening of the OLV, the registration card and computer system had occasional problems. In figure 2, the cases, which could not be registered in the system, show more than 10 cases per day in the first 4 days (blue line). The dentists could not keep the athletes waiting while the computer recovered. Handwriting in the RCd and the PF was utilised during the treatment. There were 74 cases in this situation. This is the second reason for the difference in numbers.
The number of RCds has 33 more cases than the PFs numbers (table 1). The reasons of this difference might be after registration, some athletes left without seeing the dentist because they went to have dinner, went to see other doctors in the polyclinic or went to training. In this case, they had only the RCd number, and no PF.
After analysis of these reasons, it was realised that the number of PFs was closer to the real number of dental services delivered at the Olympic Games. The finding of this study may explain the reason for differences in separate papers about the 2004 Olympic dental care.4 10
Before an Olympic organising committee makes a decision on the suitable size of a medical team or a dental team, the most important point is to understand the previous data, especially the data from the last Olympic Games. This understanding is necessary to organise and train a dental team for the host city. This should be done as early as possible.7 Unfortunately, the data were published more than 2 years after the Olympic Games. This means that a host city will only have data available for 1 year or less, before they host a new Olympic Games. If the data are not accurate, this could be unfortunate for the host city. The data from this paper were reported to the IOC in 2009.
Peak times of dental care
The first wave of dental care visits was created by assistant members of different national delegations (from the 4 days before the opening ceremony until the third day after the opening ceremony (brown line in figure 1)). As a routine practice, the team doctors always visit the polyclinic first. In this way, they can get to know the procedures for medical care at first hand. In 2008, the chief dentist tried to meet every team doctor who visited the dental care department in the polyclinic, showed them around every room of the dental department and explained to them what kind of dental problems must be treated at once and what kind of problems could better be treated after competition. With the understanding and cooperation of the team doctors, the dental care in the 2008 Olympic Games was busy but not rushed. After the OLV officially opened, the need for dental care kept rising from 20 cases per day to over 60 cases per day before the games started (period B–C in figure 1). After the opening ceremony on 8 August 2008 (day 1), the Games began. During the Games' period (C–D in figure 1), dental care came into peak hours with visiting participants of over 70–80 cases per day. On day 11, 88 cases were treated. Visits by the athletes (red line in figure 2) were significantly higher after the third day of the opening ceremony until the closing ceremony (day 17). The case numbers of athletes were suddenly lower on days 7 and day 10 (red line in figure 2). In the mean time, it was shown that the numbers of others, for example coaches or other team staff, in sport teams (brown line in figure 2) increased. According to the response from team doctors, the reason for this was that some athletes had finished their competitions, and the coaches or other assistants had time to receive dental care for themselves. After the closing ceremony, there were still some cases needing dental care in the polyclinic, but the number became less and less (period D–E in figure 1). Compared with more than 40 000 volunteers in the OLV, dental care was rarely needed by this population.
Type of dental treatments
Extraction of teeth used to be highest (370 cases) in dental services in 1968 with few endodontic interventions; however, by 2004, endodontics became higher with a significant fall in extractions. There were only six cases seeking urgent treatment of abscess in 2008. It is known that tooth extraction, abscess and endodontic are the treatments undertaken for teeth with a poor prognosis, but permanent fillings and oral hygiene are generally undertaken for teeth problems in the early stage. This may indicate that the level of dental care for athletes has been steadily progressing in 40 years. The oral health of the athletes seems to be improving. Education of the patients played an important role in improving athlete dental health in the 2008 Olympic Games (table 2).
The Mouthguard Service was extremely popular in the 2008 Olympic Games, and 122 athletes received their new custom-made mouthguards in Beijing. That might be the highest number of mouthguards made in the Olympic Games since 1932.4 Mouthguard played an important role since 1913.11,–,13 Many studies of mouthguards have been carried out in the past 50 years.14,–,18 However, many sport dentists have pointed out that a large number of uncomfortable mouthguards were still used by athletes until now.19,–,21 Knowledge of making and using the mouthguards needs to be improved.22,–,24 Greater effort must be made to improve the comfort of mouthguards if their use is to be increased.25 An investigation concerning uncomfortable symptoms after using unsuitable mouthguards by athletes was carried out in 2008.
Trauma of soft tissue and teeth is always the focus of an oral surgeon on the team of dental care. From the beginning, at least one surgeon has been scheduled for on-call everyday in the polyclinic. However, there were only six cases of either soft-tissue trauma or tooth trauma sent to the polyclinic during the 2008 Summer Games. According to the BOCOG, more trauma cases may have been treated in the venue or sent to nearby local hospitals. One oral surgeon was scheduled as an on-call doctor every day in the later stage of the 2008 Olympic Games.
Some oral problems associated with TMDs, implants and orthodontics had been found at the Beijing Olympic Games. These situations were treated by specialists. An on-call service by these specialists is necessary. Not all, but many, countries have realised that arranging for a team dentist seems necessary.26 Caring for the oral health of the athletes was their duty not only during the Olympic Games but also after the games when they returned to their home town.27,–,29
What is already known on this topic
▶ The Olympic games is a worldwide sports event which hosts more than 10 000 athletes from over 200 countries who come together in one host country to take part in the games over a period of 2 weeks. Injuries and cases of heat-related illness, even sudden death, among participants in the Olympic Games are the main focus of medical research concerning Olympic Games. However, it was found that more and more participants seek dental care during the Olympic Games since 1932. Besides physiotherapy, dental care becomes the second busiest service provided in the polyclinic of the Olympic Village. How to organise an appropriate team to provide quality dental care during the Olympic Games has become an important consideration for each successive host country.
▶ Many reports have come to the realisation that, so as not to overextend a dentist's time and stamina, it was very important to organise a suitably sized dental team for the Olympic Games. The first issue was how to determine the exact number of dental services provided in the last Olympic Games as early as possible. However, it seems difficult to obtain an exact number, and there have been no detailed reports discussing this reason until now.
▶ It was also very important to estimate which days were the peak time of dental care during the period, and what kind of dental treatments might be required. With this information, the IOC and organising committee could estimate how many dentists may be needed and what kinds of specialists would be required. Many reports on dental service in Olympic Games have been published since 1969, but only a few reports discuss the peak times of dental service during the Olympic Games. This might affect the arrangement of dentists' schedules during the service. The aim of this study is to document dental services provided at the Olympic Games in 2008 in Beijing and to provide data for planning future events.
What this study adds
▶ In this study, the reasons for difficulties in obtaining exact data for dental services in Olympic Games were analysed. Suitable ways of data control during the games were suggested.
▶ The set-up of the dental care department in the 2008 Olympic Games was also reported. The number of dentists, necessary equipment for the dental department in the Olympic Village and dental working schedules were discussed.
▶ The peak times of dental care in 2008 Olympic Games were reported in this study. This information was important for the host city to arrange the dental work, but also might be useful for the doctors in the sport teams to arrange their athletes to visit the dental department at a suitable time during the games.
▶ In the 2008 Olympic Games, there were 1607 cases involving 1126 patients requiring dental care: 795 cases from 516 athletes, 483 cases from 370 coaches and other staff, and 99 cases from volunteers. The types of dental treatments in 2008 Olympic Games were discussed in this study, and it was found that endodontic treatments, permanent fillings, oral hygiene, mouthguards and treatment for pericoronitis were the most frequent procedures in dental care. The Mouthguard Service was also very important.
Conclusions
Duties of dental care during the Olympic Games might be very heavy. More general-practice dentists were needed in the team. Different kinds of specialist were suggested to work in the team—for example, oral and maxillofacial surgeons, and sport dentists for mouthguards.
Acknowledgments
The authors are grateful to D Yu, Associate Director, Global Oral Care R&D, Johnson & Johnson, and C Mandell, Director and Chairman of the Implantology Division Dade County Dental, for their valuable guidance, support and cooperation. Both are training lecturers who acted as senior consultants for the dental service of the 2008 Olympic Games.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.