Article Text

Abstract
Objective The purpose of this review is to examine the evidence for determining the lowest threshold for diagnosing a sport-related concussion.
Data Sources MEDLINE, CINAHL, EMBASE, Mosby's Index, PsycEXTRA, PsycINFO and Scopus. Key words included sports concussion, concussion assessment, diagnosis, concussion symptoms, onfield assessment and sports-related traumatic brain injury.
Results The majority of concussions in sport occur without loss of consciousness or frank neurological signs. Some of the hallmark signs of acute concussion include mental confusion, memory and balance disturbance. Over the course of the first 24 h, the most common symptoms include headache, nausea, dizziness and balance problems, blurred vision or other visual disturbance, confusion, memory loss and ‘fatigue’. Symptoms such as tiredness, irritability, nervousness or anxiety, sleep disturbance and sensitivity to light or noise may be noticed in the days after injury. The pathophysiology of sports concussion remains poorly understood. There appears to be a period of vulnerability following concussion in which an overlapping injury might cause magnified pathophysiology.
Conclusions Sport-related concussions can be difficult to diagnose. Concussion produces an evolving constellation of somatic, cognitive and neurobehavioral symptoms that are typically most severe during the earliest acute postinjury period (ie, within the first 24–48 h) and diminish over a matter of several days to weeks in the majority of athletes. Athletes suspected of concussion should be removed from play and evaluated thoroughly.
- Concussion
Statistics from Altmetric.com
Introduction
Concussion is considered to be among the most complex injuries in sports medicine to diagnose, assess and manage. The majority of concussions in sport occur without the loss of consciousness (LOC) or frank neurological signs.1–4 In addition, most concussions cannot be visualised, identified or diagnosed using structural neuroimaging. At present, there is no perfect diagnostic test or marker that clinicians can rely upon for an immediate diagnosis of concussion in the sporting environment. To make matters more complicated, clinicians often face significant pressures to make a rapid assessment of an athlete on the sporting field to determine his or her fitness to return to play as soon as possible.
Concussion produces an evolving constellation of somatic, cognitive and neurobehavioral symptoms that are typically most severe during the earliest acute postinjury period (ie, within the first 24–48 h) and diminish over a matter of several days to weeks in the majority of athletes. When obvious signs exist (eg, LOC or concussive convulsions) the diagnosis of concussion is relatively straightforward; however, the sports medicine team can have difficulty when symptoms and/or cognitive disturbance may be delayed or when concussive symptoms may be present but not specific for the injury. Similarly, symptoms may be inaccurately reported by athletes who either do not recognise the significance of the symptoms or are reluctant to report them because of fear of being removed from competition or indeed may not endorse symptoms because they are concussed.5–7 Although the complexity of this injury underscores the importance of a thorough multimodal examination as well as the potential usefulness of having a baseline cognitive and symptom scores for each athlete, it also highlights the very real difficulty for team physicians in determining the ‘minimum’ concussion diagnosis. The purpose of this review is to consider the published evidence regarding the minimal diagnosis of concussion and to provide recommendations from an expert consensus group as this may be practically utilised.
Methods
Articles were retrieved via on-line database searching, hand-searching reference lists and cited reference searches. The online databases of MEDLINE, CINAHL, EMBASE, Mosby's Index, PsycEXTRA, PsycINFO and Scopus were searched. Key words, MeSH terms and combinations of these were used to systematically search the databases. Key words included sports concussion, concussion assessment, diagnosis, concussion symptoms, onfield assessment and sports-related traumatic brain injury.
Results
Definition of concussion
Head injuries and their effects have long been recognised in the medical literature. A detailed description of the history of concussion has been reviewed elsewhere.8 ,9 This historical view of concussion being a low-velocity injury leading to transient disturbance of function rather than structural damage has been maintained as a key element of current definitions. It is worth noting that in many European countries the term brain commotion or commotio cerebri is still used today to mean concussion.
Consensus definition—circa 1966
In an attempt to standardise the definition of concussion, a working party was formed by the Congress of Neurological Surgeons in 1964. After a debate, a consensus definition was finally deduced and published in 1966.10 Concussion was defined as, “a clinical syndrome characterised by immediate and transient impairment of neural function, such as alteration of consciousness, disturbance of vision, equilibrium, etc., due to mechanical forces.”10 Until 2002, this definition has been the most commonly accepted definition in both research and clinical practice.
Consensus definition—circa 2002
Recently, the issue of a standardised injury definition was revisited at the first International Conference on Concussion in Sport.11 The Concussion in Sport Group felt that while the Congress of Neurological Surgeons’ definition was useful, it had a number of critical limitations. In particular, it was too simplistic and failed to account for some of the common clinical presentations of sports concussion.11
The Concussion in Sport Group defined concussion as, ‘a complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces’ that ‘may be caused by a direct blow to the head, face, neck or elsewhere in the body with an impulsive force transmitted to the head’.11 The definition went further to include the points listed below.
-
“Typically results in the rapid onset of short-lived impairment of neurological function that resolves spontaneously”;
-
“May result in neuropathological changes, but the acute clinical symptoms largely reflect a functional disturbance rather than a structural injury”;
-
“Results in a graded set of neurological syndromes that may or may not involve an LOC. Resolution of the clinical and cognitive features typically follows a sequential course”;
-
“Is typically associated with grossly normal structural neuro-imaging studies”.11
In the outcome papers of the second and third International Conferences on Concussion in Sport, this definition remained largely unchanged12 beyond noting that in some cases postconcussive symptoms may be prolonged or persistent.
Concussion or mild TBI?
Although the terms mild traumatic brain injury (mTBI) and concussion are often used interchangeably in the sporting context and particularly in the US literature, others use the term to refer to different injury constructs. Concussion is the historical term representing low-velocity injuries that cause brain ‘shaking’ resulting in clinical symptoms and which are not necessarily related to a pathological injury.9 In Europe, the term commotio cerebri is often used in place of concussion to represent this injury.
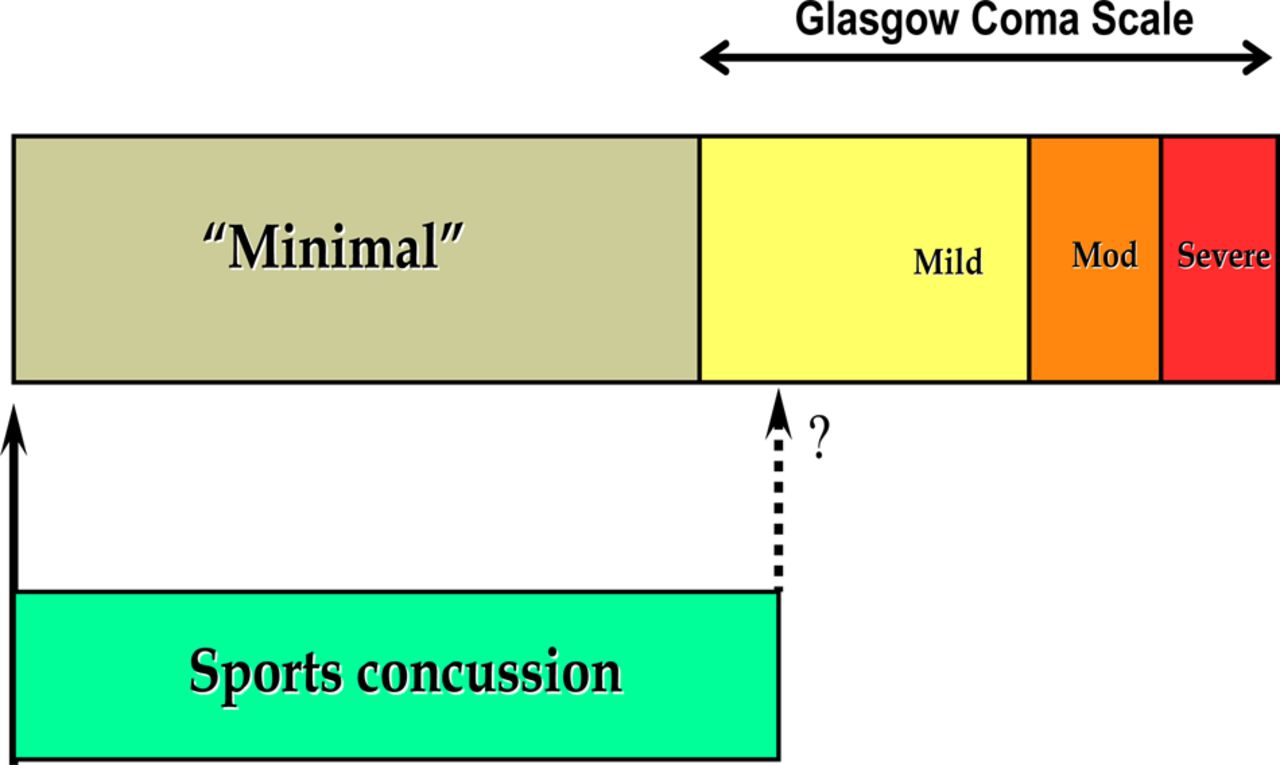
In contrast, mTBI is part of a spectrum of injury severity that reflects a pathological injury. This is most simply differentiated by the Glasgow Coma Scale, which is a prospectively validated prognostic scale for the assessment of traumatic brain injury that is widely used in emergency departments worldwide.13 The different forms of TBI (mild, moderate and severe) are distinguished on the basis of a standardised score that is assessed 6 h postinjury. The time frame was used to exclude relatively minor injuries that have no neurosurgical significance, from the analysis. To fit these injuries into a full spectrum of traumatic brain injury using this conceptual model, one must also include a ‘minimal’ injury subset that falls below the threshold of mTBI (ie, Glasgow Coma Scale (GCS) score 15) at the 6 h time point. In this sense, the majority of concussive injuries seen in sports, fall into this category (figure 1). According to this model, concussion is a subset of GCS mild brain injury, however, the converse is not true and the terms cannot be used interchangeably.

{kind=link}
Conceptual understanding of sports concussion. This figure is only reproduced in colour in the online version.
Pathophysiology of concussion
The pathophysiology of sports concussion remains poorly understood.14–18 Owing to difficulties in studying the phenomenon in humans, much of our current understanding has been derived from experimental animal models of impact or acceleration. However, these models have significant limitations in their application to sports concussion. Although detailed reviews of the pathophysiology of acceleration concussion already exist in the current literature,19 ,20 and such reviews are beyond the scope of this literature, a general overview is important for an understanding of the topic.
Linear acceleration or rotational shearing forces transmitted to the brain are proposed to result in a series of short-lived neurochemical, metabolic and gene expression changes.15 ,19 ,20 Some of the common changes observed experimentally are listed below.
Physiological evidence of metabolic vulnerability following injury
A number of animal and human studies on mild TBI and concussion have focused attention on concussion-induced changes in brain metabolism, including those related to cerebral energy state.14 ,27 Hovda et al20 first suggested the concept of metabolic vulnerability occurring in brain tissue after any concussive episode. During this transient period of altered brain metabolism and function, a second concussive episode of even modest entity may cause significant additional and/or dramatic brain damage.28
This concept has been supported in recent studies using magnetic resonance spectroscopy (MRS) in animal and human models of concussive injury.29–31 These observations suggest that N-acetylaspartate (NAA) measurement may be a valid indirect biomarker of the brain energy state.30 ,31 Coupled with its non-invasive in vivo detectability by proton MRS (1H-MRS),32 NAA appears to be a useful index in monitoring metabolic brain changes following concussion in humans. Subclinical alterations of central energy metabolism might well represent a reasonable explanation of the striking and unpredictable discordance often observed between the minimal findings on conventional imaging and the extent of neurocognitive deficits exhibited by patients with mild TBI.33 The results of this pilot study indicated that NAA cerebral levels are decreased for weeks after concussion, even after the resolution of all concussion-associated clinical symptoms, with normalisation to control values occurring only 30 days postinjury.34 Another study by Chamard et al raised the issue that even non-concussed athletes may have MRS abnormalities and these authors suggested that subconcussive impacts may also induce similar changes. These findings need to be independently verified.35
It is likely that besides indicating a general alteration in cellular homeostasis, these findings might reflect a condition of energetic imbalance. As long as this energy deficit persists, NAA resynthesis is significantly impaired.36 ,30 Researchers have reported a profound period of subclinical bioenergetic depression in the concussed brain, corresponding to the well-known state of metabolic ‘brain vulnerability’, that follows a concussive event.30 ,31 ,36
Animal work shows cognitive impairments correlating with the time period of glucose metabolic dysfunction (as distinct from the mitochondrial impairment of Vagnozzi et al36), lasting about 7–10 days in adult rats.23 The time window animal studies of Vagnozzi et al36 suggest that mitochondrial dysfunction is maximally exacerbated when injuries occur at 3 days gap.
Keeping concussed athletes from participating in physical (or mental) activity to prevent brain activation, while it is intuitive to some, has mixed evidence. Animal evidence suggests that exercise in concussed rodents worsens outcome when the exercise occurs acutely after an injury, however, if instituted more than 1 week after the injury the exercise then confers benefits in terms of recovery.37 ,38 Human evidence is limited to class III studies that, while intriguing, require replication prospectively and with more objective measurement of activity levels. One human study suggests moderate levels of activity were associated with best outcome.39
Some metabolic studies carried out in juvenile animals after concussive injury show they actually recover faster, while studies of plasticity and cognition in juvenile animals suggest that concussive injury has more lasting effects, which suggests abnormalities extend beyond simply physiological change.40
The data suggest there is a period of postconcussive metabolic dysfunction; the early phase of which may be associated with vulnerability to second injury and to excessive neural stimulation. Currently, it remains uncertain as to whether similar biomechanical, metabolic and gene expression changes occur in all cases of human sports concussion and, more importantly, whether the clinical symptoms reflect this process.12
Do athletes report the injury correctly?
As mentioned previously, the subjective reporting of symptoms is problematic when athletes are less than honest when reporting their symptoms. Athletes often minimise and/or do not report their symptoms because they want to play and believe that their symptoms are mild enough to safely play through them. It is common for athletes, at all levels, to assume that ‘having their bell rung’ is part of the game, and they do not realise the significant possible consequences of playing with concussion.
In a study of high-school football players, only 47.3% of players with a concussion reported their injury. Of those who did not report, 66.4% did not think their injuries were serious enough to report, 41% did not want to be held out of play and 36.1% did not realise their symptoms were consistent with concussion. In this study, when injuries were reported, they were most often reported to an athletic trainer. It is important that the culture of sports change such that athletes, parents, coaches and healthcare providers understand the significance of unreported, repetitive concussive injury. This is most important at the youth level where sports-trained medical providers, such as athletic trainers and team physicians, are often not available.
Recognition of concussive impacts
The first step in evaluating and managing concussion is recognition of injury. Although a big hit gathers the attention of medical staff and others present, it is important to realise that the mechanism of injury may be subtler and not as obvious. The mechanism of injury may not even be a single impact, but rather the combined effects of multiple hits over a short period of time (minutes). In a study evaluating the relationship between the force of impact in college football and clinical outcome, magnitude of impact did not correlate with clinical injury.41 This study used accelerometers embedded into the football helmet and evaluated athletes with a clinical programme involving preinjury baseline testing (symptoms, neuropsychological testing, postural balance testing) and repeat postinjury testing. The postinjury measures were compared with the baseline measures. The impact magnitude of the hits in concussed athletes ranged from 60.51 to 168.71 g, yet no significant relationships between these impacts (linear or rotational, location) and the change scores for symptom severity, postural stability or neurocognitive function were found.
Physical signs of acute sports concussion
The symptoms of concussion are one component of diagnosis with the other components including a neurological examination, cognitive assessment and balance evaluation. The physical examination is important to exclude other critical diagnoses, as well as to determine whether additional emergent evaluation is necessary.
The hallmark signs of acute sports concussion include LOC, problems with attentional mechanisms (often manifest as slowness to answer questions and follow directions, being easily distracted, poor concentration, vacant stare/glassy eyed or inappropriate playing behaviour), memory disturbance and balance disturbance.1 ,2 ,42 ,43
Other signs of acute sports concussion that have been variably reported in the literature include concussive convulsion or impact seizures, and emotional lability or displaying inappropriate emotions (eg, laughing or crying).12 ,44–46 At best, such symptoms correlate only moderately with neurocognitive and balance measures.47 ,48 The range of clinical symptoms scale and their reliability have been reviewed elsewhere.49
Guskiewicz et al have demonstrated increased postural sway in concussed athletes using both sophisticated force plate technology50 and simple clinical tests of balance.51 The studies have shown that postural deficits are most pronounced within 24 h of injury and return to baseline levels by 36–48 h postinjury. Overall, assessment of balance may provide useful additional information in concussed athletes as part of their overall management.51
Acute symptoms reported following sports concussion
Sports concussion typically results in a range of acute and delayed symptoms in the injured athlete. Historically, the reporting of these symptoms has been largely anecdotal.52 Moreover, in the few prospective studies that exist in the literature, findings are often variable. Common symptoms in the initial minutes following injury include headache, dizziness and some form of mental status disturbance, such as mental clouding, confusion or feeling slowed down. Over the course of the first 24 h, the most common acute symptoms reported in the literature include headache, nausea, dizziness and balance problems, blurred vision or other visual disturbance, confusion, memory loss and ‘fatigue’.1 ,2 ,43 ,53–57 Symptoms such as tiredness, irritability, nervousness or anxiety, sleep disturbance and sensitivity to light or noise may be noticed in the days after injury.54 ,58 ,59 It is important to note that not all of these symptoms are seen in every case of sports concussion. Furthermore, there is often variable presentation of symptoms even in the same athlete who is concussed on multiple occasions.
Baseline, preinjury symptom reporting can be influenced by a number of situational factors (eg, school-related stress, peer relationship difficulties, fatigue, over-training and illness). Symptom reporting often reflects a ‘state’, not a ‘trait’. However, some athletes do have trait-like baseline experiences with these symptoms. There is a large literature in civilian mTBI illustrating that these symptoms, especially postacutely, are not specific to concussion—they are commonly reported by people with depression, anxiety and chronic pain.60
Neuropsychological deficits in acute concussion
Acute neuropsychological deficits have been described following sports concussion. Some domains of functioning that can be adversely affected are listed below.
-
Reduced planning and ability to switch mental set61–64;
-
Reduced attention and ability to process information8 ,68–72;
-
Slowed reaction times and increased variability of responses.73–76
Neuropsychological deficits can be pronounced in the initial minutes and hours following an injury. Over the initial days following an injury, neuropsychological deficits associated with sports concussion are usually subtle and may exist in a number of cognitive domains. To be most useful, neuropsychological testing must be sensitive enough to detect mild changes and specific for the cognitive domains in which deficits are commonly observed. This area has been reviewed in detail in one of the accompanying papers in this supplement.
Do we have sufficient evidence or knowledge to diagnose something other than a concussion in mild or transient cases?
In essence, concussion becomes the default diagnosis and must be excluded or ruled out. Conceptually, it is important to appreciate that sideline tests, neuropsychological scores or symptom scales do not diagnose whether a concussion has occurred. Rather, tests measure the physiological, cognitive, psychological and behavioural changes associated with the injury. The diagnosis of concussion is based on a comprehensive assessment of the injury event and the athlete's acute signs and symptoms at the time of assessment. However, because the injury may be evolving pathophysiologically it may not be possible to be certain of the diagnosis in the acute stage of the injury.
Without the presence of a biomarker or confirmatory test, it may be helpful to define concussion as the clinical manifestation of an underlying brain injury. In this way, concussion becomes a possible clinical outcome from a subset of TBI—specifically the subset that causes the metabolic cascade to the degree needed to cause a clinical effect for the injured brain. If there are temporary symptoms such as those that are not caused by the cascade or by any measurable cellular pathology, but by piezoelectric depolarisation caused by the biomechanical force, then should they also be labelled as concussion. Given the evolving nature of the injury and the fact that the duration, severity and trajectory of this injury cannot be adequately estimated in the very acute stages, then concussion becomes the default diagnosis. Some concussions also have very brief symptom presentation but may not produce a measurable clinical or cognitive injury and have no detectable sequelae given the current technology.
Discussion
Overall, the diagnosis of concussion in athletes can be problematic especially if the injury is ‘mild’, the symptoms subtle, the physiology evolving and the functional effect minimal. Compounding the ability of the sports medical staff to assess the injury is often the unwillingness of the athletes to declare or even recognise his or her symptoms as being concussive in nature.
The previous Concussion in Sport Group meetings have highlighted the need for a 360° or multifaceted assessment of the injury, which in part relates to the variability in the sensitivity or specificity of the various components of this assessment, if done in isolation.
Given the metabolic and possibly neuropathological vulnerability in the period immediately following a concussion, significant risk may exist for all athletes who sustain a concussion. At this point in time, the scientific evidence does not allow us to distinguish different outcomes in different athletes with the same injury. We know from biomechanical studies that there is an intrinsic variation in tolerance to head impacts, which could be speculated to have a genetic basis; however, our understanding of these injuries remains elusive. This means that we need to have a high degree of clinical suspicion and all head injuries need to be treated as a concussion until proven otherwise; a determination that is impossible to make in the first few hours after injury.
Proposed diagnostic criteria for concussion
An athlete who has any one or more of the following, needs to be removed from play with a suspected concussion and then assessed in a thorough fashion.
-
Initial obvious physical signs consistent with concussion (eg, LOC, convulsion or gait unsteadiness).
-
Teammates, trainer or coaching staff observe cognitive or behavioural changes in functioning [eg, mental confusion (often manifest as slowness to answer questions and follow directions, being easily distracted, has poor concentration, vacant stare/glassy eyed or inappropriate playing behaviour) or emotional lability].
-
The athlete reports any concussive symptoms.
-
Abnormal neurocognitive and/or balance examination (eg amnesia, confusion or other neurological abnormalities).
While there is no hard scientific evidence for or against this approach at this stage, it does reconcile some of the clinical observations seen in athletes. It is important to consider that all such injuries need to be treated as a clinical concussion (ie, removal from play and medical assessment) given that even these ‘non-clinical concussions’ may have the potential for adverse outcomes. Embedded in that approach is the concept that diagnosing concussion is often not a ‘point in time’ event but rather one that requires observation over time and exclusion of other conditions that may mimic a concussion. Management is then based not on whether or not the clinician has diagnosed concussion, but rather whether or not he or she has diagnosed something else. In the interim, between injury suspicion and concussion diagnosis, the patient is treated as if they are concussed.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Competing interests See the supplementary online data for competing interests (http://dx.doi.org/10.1136/bjsports-2013-092247).
-
Provenance and peer review Commissioned; internally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmjgroup.com