Article Text

Abstract
Background Chronic groin pain is a common and debilitating condition in highly active athletes. Symptoms are often ascribed to the so-called Sportsman's Hernia, and these patients frequently undergo prolonged and often painful remedial physiotherapy, or, if the condition is refractory, surgery to repair the posterior inguinal wall.
Hypothesis We hypothesised that radiofrequency denervation (RFD) of both the ilioinguinal nerve and inguinal ligament could be used to desensitise the groin region and enable the athlete to become pain-free.
Study design A prospective randomised controlled trial of three groups of patients with chronic groin pain.
Methods Thirty-six patients with chronic groin pain of greater than 6 months duration, with no identifiable structural cause and which was refractory to conservative treatment, were randomised into two groups. Group 1 was treated with RFD (n=18), while group 2 was treated with local anaesthetic (Bupivicaine) and steroid (Trimacinolone) injection (n=18). A further 10 patients with previous failed surgery for the same condition were treated with RFD without randomisation. All patients then underwent a standardised physiotherapy regimen. The Visual Analogue Scale at rest (VASr) and with activity (VASa) was used to assess pain, and London Adductor and Abdominal Groin Score was used to assess function, at baseline and at 1 week, 3 months and 6 months post-treatment.
Results RFD treatment resulted in a significant improvement above baseline in all measures and at each time intervals up to 6 months, in both the randomised Group 1 and in the postsurgery group (p values ranging from <0.001 to 0.001). Injection of local anaesthetic and steroid resulted in a significant improvement above baseline in all measures, but only at 1 week (p values ranging from 0.001 to 0.021), and not at any of the later intervals. Improvements in all measures was significantly greater in Group 1 than in Group 2 at all follow-up intervals (p values ranging from <0.001 to 0.003). No persistent adverse events were recorded.
Conclusions The use of RFD in the treatment of refractory Sportsman's Hernia is safe and efficacious at least in the short term, and is superior to anaesthetic/steroid injection. The results suggest that symptoms are related to tendon inflammation and ilioinguinal nerve compression, and can be abolished with pharmacological or radiofrequency treatment, without the need for surgery.
Clinical relevance This novel technique could help athletes suffering from chronic groin pain return to play more quickly, both facilitating and allowing deferral of remedial physiotherapy treatments, and potentially avoiding the need for surgery.
- Groin injuries
- Intervention effectiveness
Statistics from Altmetric.com
Introduction
Chronic groin pain is a common cause of disability in athletes from a variety of sports.1–4 This chronic pain can result from identifiable pathology of the hip joint and pubis or related tendons. However, many of these cases are given the final diagnosis of ‘Sportsman's Hernia’ (also sometimes referred to as Gilmore's groin, athletic pubalgia, incipient hernia, posterior abdominal wall deficiency, or, simply, groin strain): an ill-defined but debilitating and common condition that represents a large proportion of the cases of chronic groin pain when alternative diagnoses have been excluded.5 This syndrome is likely to have a multifactorial aetiology resulting from overload of the lower anterior abdominal wall and pelvis, with suggestions that symptoms are contributed to by laxity of the posterior inguinal wall, conjoint tendonitis or compression of the ilioinguinal nerve.6 Patients often demonstrate non-specific physical examination findings and normal imaging findings.7 However, symptoms are often severe enough to have ended the careers of a number of professional athletes.8–13 Physical therapy and core stability exercises may be used to control the condition, but efforts are frequently hampered by persistent pain, and are often unsuccessful.14 Refractory cases are often treated with surgery that sets out to strengthen the posterior inguinal wall, but this can be a morbid and expensive procedure, with a long recovery time.6 Given that there is no grossly identifiable structural damage, it may be satisfactory to simply abolish the pain rather than attempt to surgically correct the usually obscure underlying mechanical imbalance.
We postulated that, irrespective of the causative pathology, radiofrequency denervation (RFD) could be used to desensitise the nerves supplying the inguinal ligament enabling the athlete to become pain-free. Athletes could then be allowed to return to play more rapidly, while simultaneously undertaking physiotherapy focusing on strengthening the weak abdominal wall and improving core stability.
Objective
This pilot study seeks to determine the efficacy and safety of using RFD in patients with this condition by randomising patients to receive either RFD or injection of local anaesthetic and steroid.
A third group of patients with failed surgery for the same condition was treated exclusively with RFD, as a pilot study to determine the efficacy of the treatment in that population.
Design
Study design
We conducted a prospective randomised controlled blind trial following institutional review board and local ethics committee approvals. The trial was registered with the National Research Ethics Services (National Patients Safety Agency) with registration number 08/H0724/28.
At enrolment, pain scores (Visual Analogoue Scale at rest (VASr) and during activity (VASa)) and a targeted groin pain and function score (London Adductor and Abdominal Groin (LAAG) score) were determined. Patients were provided with a participation information sheet which included details of the study. Informed consent was obtained from all eligible patients after explaining potential risks such as bleeding, infection and nerve damage. Patients then received their randomised intervention. Follow-up VASr, VASa and LAAG were subsequently recorded at 1-week, and at 3-month and 6-month intervals.
Patient enrolment
Patients with chronic groin pain of no readily identifiable structural cause and of greater than 6 months duration were recruited from a public sector outpatients department, referred from consultant orthopaedic surgeons and sports physicians. All had received extensive clinical assessment and MRI scans to exclude alternate diagnoses (such as inguinal hernia, hip joint disorders, iliopsoas bursitis, symphyseal degeneration, adductor tears and stress fracture). All patients had failed conservative treatment, including physiotherapy. Patients with previously unsuccessful surgery for a diagnosis of ‘Sportsman's Hernia’ were also eligible for enrolment in the study, as a separate subgroup, but were not randomised.
Recruitment started in February 2008 and concluded in July 2009.
All 46 patients screened were eligible for enrolment. Of these 46 enrolled patients, all completed the prescribed treatments and follow-up evaluations.
Randomisation
Randomisation was generated by dedicated software (StatsDirect Ltd, Cheshire, UK). This was operated by an independent individual, who did not participate in the treatment. Results of randomisation were presented to the proceduralist (DC) immediately prior to the procedure.
Ten patients previously had surgery in an attempt to resolve their symptoms, which had been unsuccessful; these patients were not randomised, but instead progressed directly to RFD. The remaining 36 patients were randomised into two groups; group 1 received RFD of the ilioinguinal nerve and inguinal ligament (n=18) and group 2 received local anaesthetic (Bupivicaine 5 ml 0.5%) and steroid (Trimacinolone 40 mg) injection (n=18) around the same structures.
Outcome measures
Subjective pain assessment was made using VAS on a scale from 0 (no pain) to 10 (worst pain ever). Functional assessment was achieved using LAAG score on a scale from 0 to 100. The questionnaire is a non-validated index of Sportsman's Hernia which includes questions regarding patients’ symptoms, functional tests and ability to play sport (see appendix). LAAG and VAS scores were self-reported; the VASa scores were reported from patient memory of recent activity. Six questions in the LAAG questionnaire were scored using a VSA from 0 to 10.
RFD procedure (group 1 and postsurgical patients(group 3))
A single operator performed all the procedures (DC). An ultrasound of the symptomatic groin was performed in order to identify the ilioinguinal nerve and the inguinal ligament. Abnormalities of the inguinal ligament were sometimes demonstrated in these patients (figure 1A,B). About 5 ml of local anaesthetic (Bupivacaine 0.5%, AstraZeneca, London, UK) was infiltrated around the nerve and ligament under direct ultrasound guidance. Using a 22G 10 cm straight cannula with a 10 mm active tip (S-1010, Neurotherm, Wilmington, Massachusetts, USA) and matching 10 cm length thermocouple electrode (NRFE-10, Neurotherm), RFD was initially applied for 3 min to the nerve (adjacent to the iliac crest; figure 2) and then along the length of the distal half of the ligament (figure 3).

Ultrasound (A) and Power Colour Doppler (B) appearances of the inguinal ligament tear demonstrated as disruption of the normal linear fibrillar structure (white arrow) at the pubic bone attachment of the inguinal ligament. This figure is only reproduced in colour in the online version.

Photograph of patient as in figure 1 treated with radiofrequency denervation (RFD) under ultrasound guidance using 10 cm straight cannula with both a 10 mm active tip and matching 10 cm length thermocouple electrode, RFD was applied for 3 min along the length of the distal half of the ligament close to the attachment on to the pubis. This figure is only reproduced in colour in the online version.
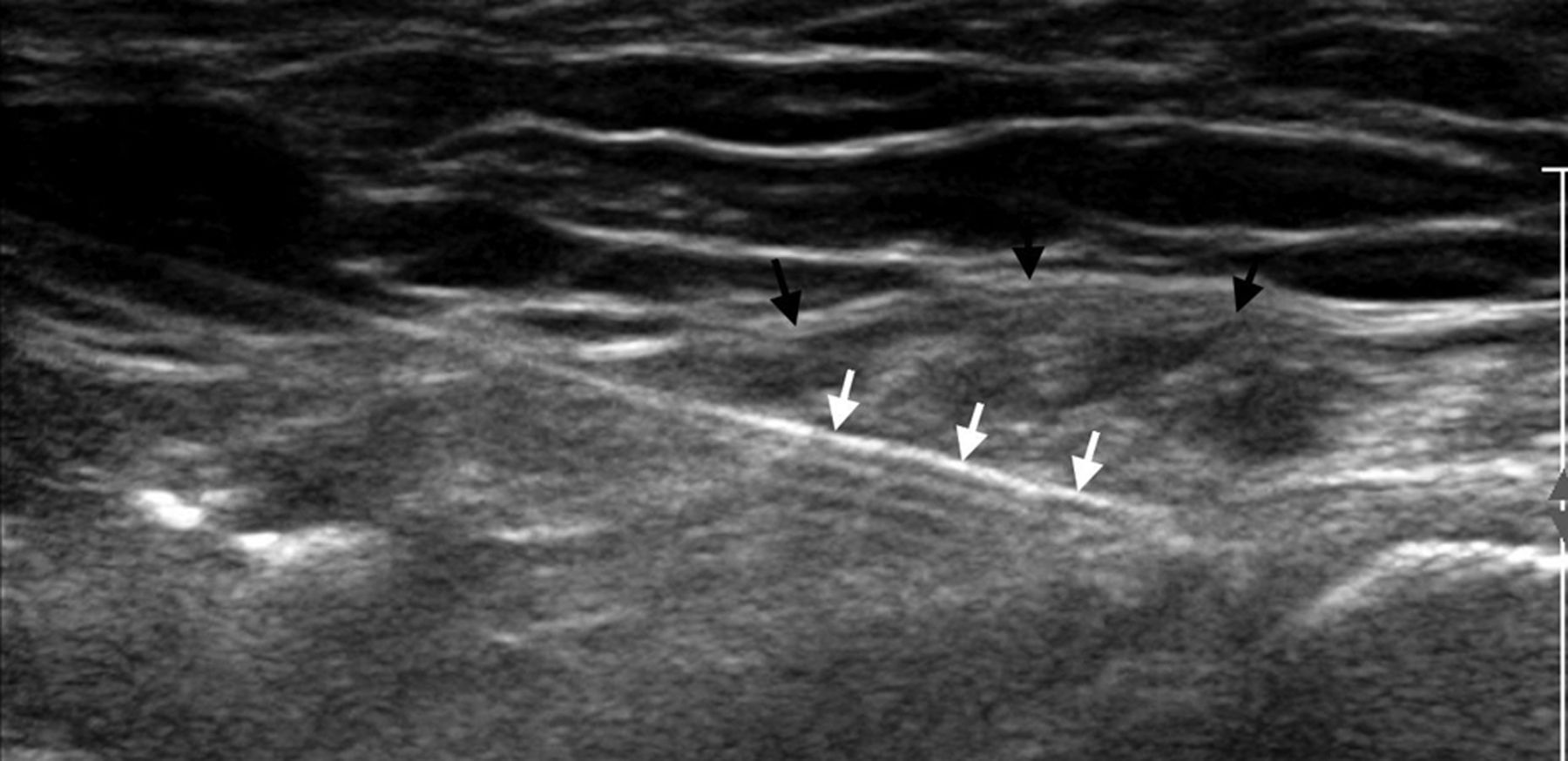
Ultrasound image of the cannula and matching length thermocouple electrode (white arrow) positioned proximally within the inguinal ligament (black arrow).
The first application was close to the attachment on to the pubis, and then retracted 10 mm proximally for the second sequence. A total of four applications were performed and this covered a 4 cm length of the distal inguinal ligament. The RF settings were 2 Hz, 20 ms widths, at 45 V for 2:00×3 (NT 1100 RF Generator, Neurotherm, Wilmington, Massachusetts, USA) under the supervision of a consultant anaesthetist. Temperature was limited not to exceed 80°C. Patients were discharged home after 1 h of observation. Exercise and heavy lifting were forbidden for the following 48 h. The patients were reviewed by the physiotherapist on the day of treatment and provided with an instruction leaflet to begin a standardised physiotherapy protocol specific to Sportsman's Hernia after the 48 h period, if there were no complications. This included exercises for the adductors, abdominals and gluteals, which were initially isometric and then eccentric. The physiotherapist monitored and supervised the programme through email and telephone correspondence. Patients were reviewed in the groin clinic after 6 weeks and 3 months to reassess their VAS and LAAG questionnaires.
Steroid injection procedure (group 2)
The same single operator performed all the procedures (DC).
In place of RFD, the patients had the distal 4 cm of the inguinal ligament bathed in 40 mg triamcinolone and 4 ml of bupivacaine (0.25%) under sonographic guidance. Preprocedural and postprocedural management was otherwise identical.
Statistical analysis
The statistical analysis was performed by an independent statistician using SPSS V.18.0 (Chicago, Illinois, USA).
The primary outcome measure was LAAG, and the secondary outcome measures were VASr and VASa, and the primary time point was 6 months. Both LAAG and VAS scores were checked for normal distribution which was not fulfilled across all repeated measurements. Therefore, non-parametric significance testing using Mann-Whitney U test for between-group and Wilcoxon test for within-group testing was applied.
Groups 1 and 2 were compared in a confirmative way. To correct for multiple comparisons the Bonferroni procedure was applied. p Values<0.005 (0.05/10) were considered to indicate statistically significant differences. Data were given as mean±SD, 25th, 50th and 75th percentiles and minimum and maximum values.
Differential diagnosis of groin pain
-
Soft tissue:
-
Adductor tendonitis
-
Rectus abdominis tears/strain
-
Iliopsoas tendinits/bursitis
-
Gracilis syndrome
-
Hernias:
-
Femoral
-
Inguinal
-
Obturator
-
Bones and joints:
-
Osteoarthritis of the hip joint
-
Avascular necrosis of the femoral head
-
Labral tear
-
Transient osteoporosis of the femoral neck
-
Osteitis pubis
-
Stress fractures of the femur and pelvic bones
-
Avulsion fractures
-
Sacroiliitis
-
Neuropathic:
-
Obturator nerve
-
Lumbar radiculopathy
-
Ilioinguinal neuropathy
-
Referred pain:
-
Epididymitis
-
Ureteric colic
-
Prostatitis
Results
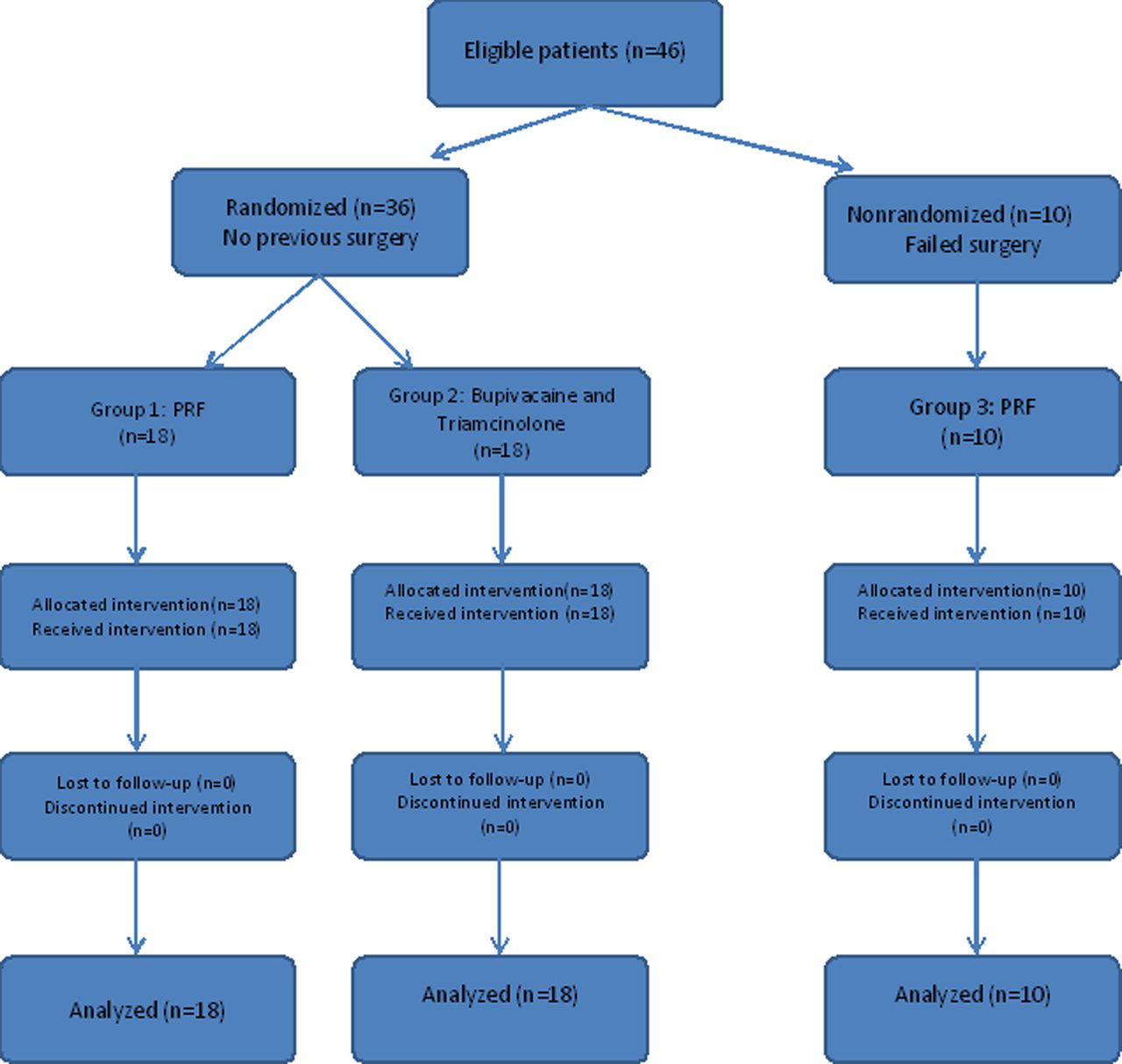
Forty-six patients who satisfied the study criteria were recruited. All patients were males. Twenty had right-sided symptoms, and 26 had left-sided symptoms. The mean duration of symptoms was 9.1 months (range 6–17.3 months). Mean patient age was 43.2 years (range 18–67). Twenty were professional full-time athletes. The most commonly main sports played were football (18 patients) and cricket (9 patients). Patient flow is illustrated in figure 4.
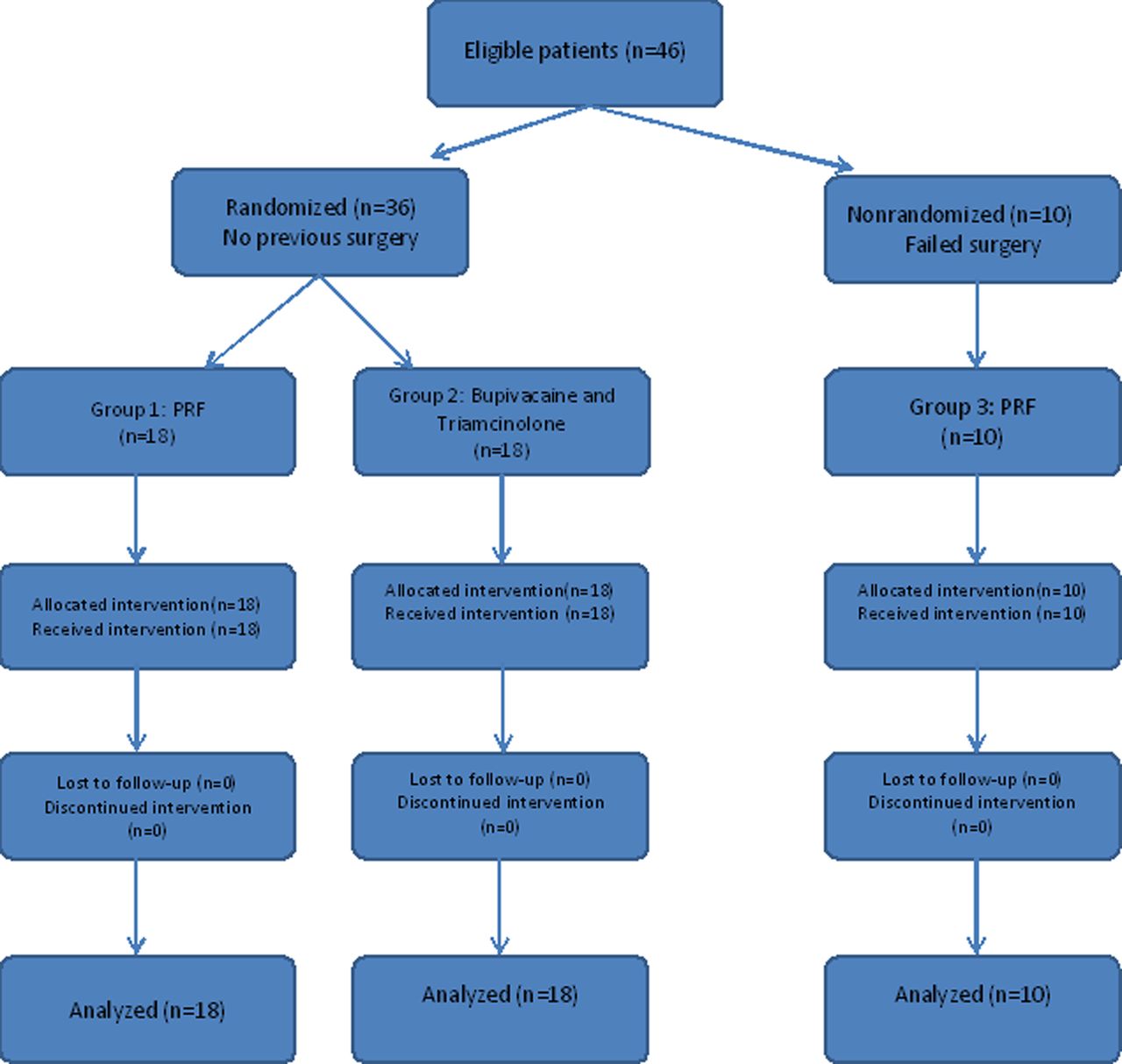
Flow diagram using Consort template to demonstrate the various stages of patients’ recruitment, follow-up and analysis. This figure is only reproduced in colour in the online version.
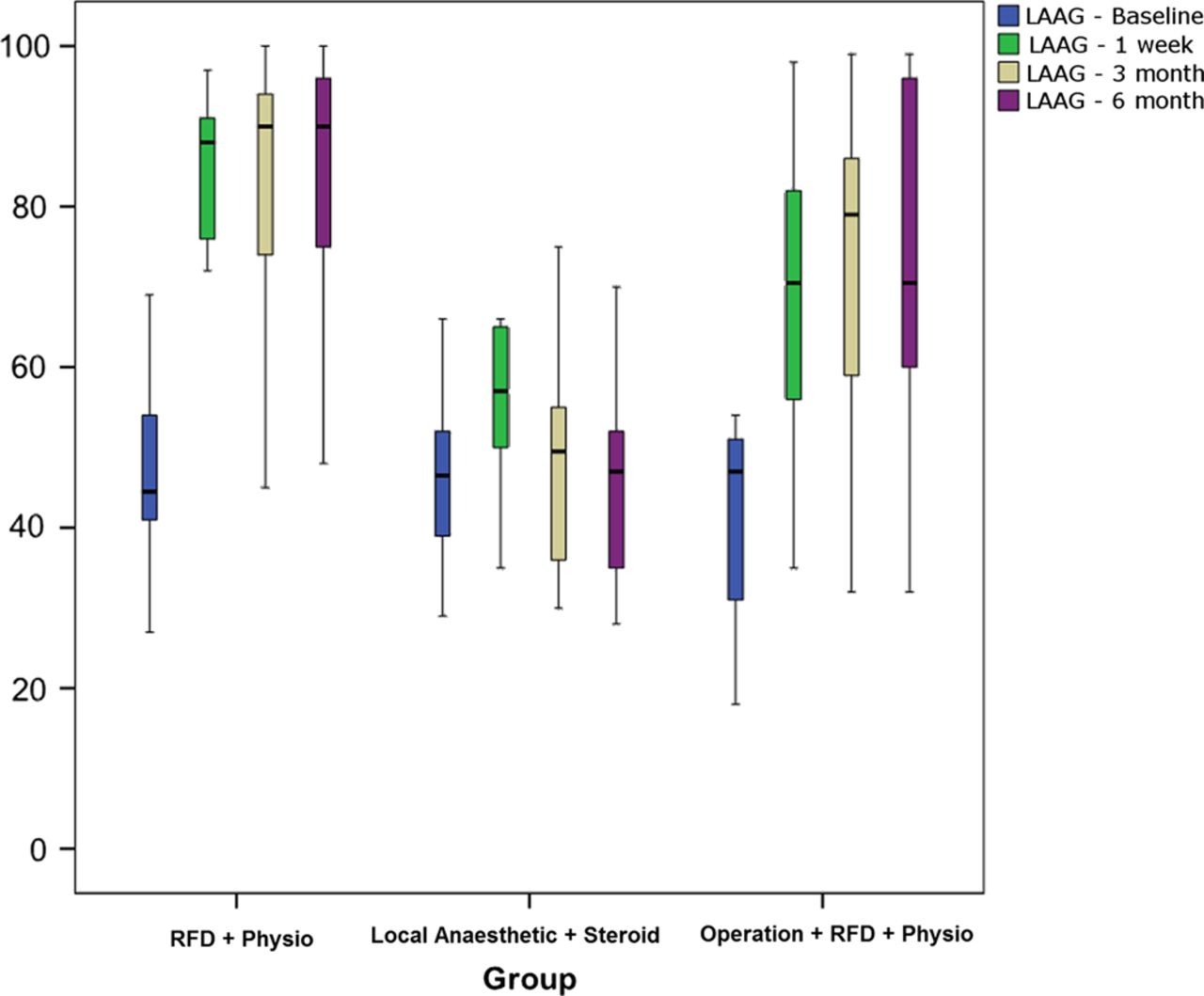
There were no procedural complications. Four patients in group 1 and 12 patients in group 2 ended up having surgery. The distribution of LAAG and VASa/r scores preintervention and 1 week, 3 and 6 months postintervention for all the groups is illustrated in (figures 5⇓–7). Mean scores within a box represent the upper and lower quartiles and the whiskers signify the range.

Boxplots demonstrating the between-group and within-group London Adductor and Abdominal Groin scores for the three groups. Significant improvement is noted in group 1 (radiofrequency denervation+physiotherapy) after 1 week, 3 and 6 months when compared with baseline. This figure is only reproduced in colour in the online version.
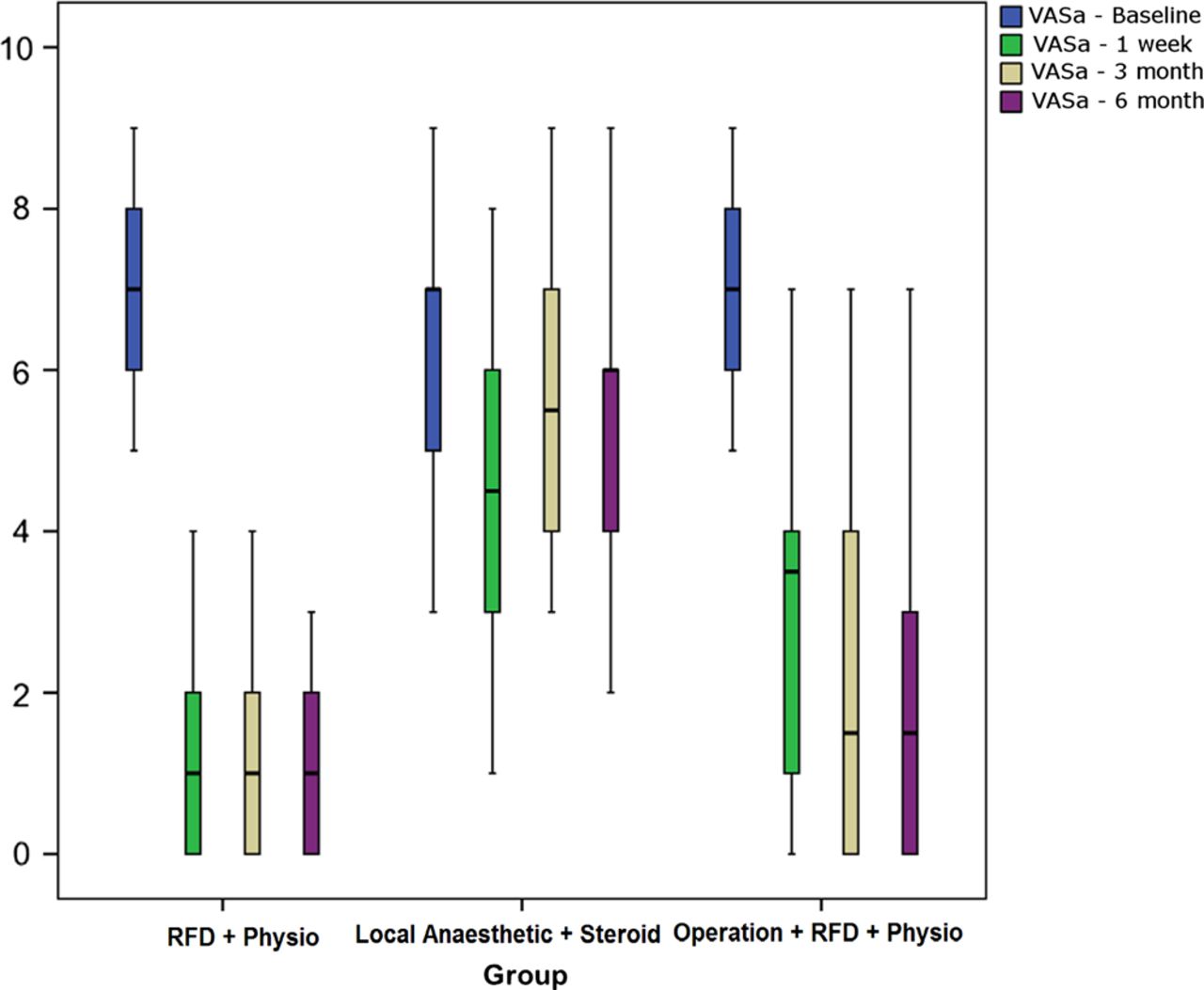
Boxplots demonstrating the between-group and within-group Visual Analogue Scale (VAS) scores (at activity) in the three groups. There is significant improvement in the VAS score in group 1 after 1 week, 3 and 6 months when compared with the baseline and the groups 2 and 3. This figure is only reproduced in colour in the online version.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Boxplots demonstrating the between-group and within-group Visual Analogue Scale (VAS) scores (at rest) in the three groups. There is significant improvement in VAS score in group 1 after 1 week, 3 and 6 months when compared with the baseline and groups 2 and 3. This figure is only reproduced in colour in the online version.
Within-group comparisons
All scores were statistically improved versus baseline at each time interval in group 1 (all p<0.001), and to a slightly lesser extent in group 3 (p=0.005–0.007; table 1). In group 2, only LAAG and VASa were improved versus baseline, and only at week 1 (p<0.001–0.001). There was a non-significant improvement in VASr at 1 week versus baseline in this group (p=0.021), which became weaker at later follow-up intervals.
Within-group comparison Wilcoxon tests versus baseline
The mean VASa score had significantly improved in group 1 from 6.89 (baseline) to 1.61 (6 months post-treatment) and in group 3 from 7 (baseline) to 2.20 (6 months post-treatment, while in group 2 there was only non-significant improvement from 6.22 (baseline) to 5.72 (6 months post-treatment).
The mean VASr had also improved in group 1 from 4.28 (baseline) to 1.44 (6 months post-treatment) and in group 3 from 4 to 1.40, but was almost unchanged in group 2 (from 2.89 to 2.94).
The mean LAAG scores improved from 47.22 (baseline) to 83 (6 months post-treatment) in group 1, and from 42.2 to 73.2 in group 3, but again nearly unchanged in group 2 (from 45.67 to 46.06).
Between-group comparisons (groups 1 and 2)
Applying the Bonferroni-corrected significance level of 0.005, there was no significant difference of LAAG or VASa scores between groups 1 and 2 at baseline (p=0.913 and 0.323, respectively); VASr was significantly higher in group 1 (p=0.003; table 2).
Between-group comparison Mann-Whitney U tests between groups 1 and 2
LAAG and VASa scores became significantly lower in group 1 at 1 week, 3 and 6 months (p<0.001 for all). The VASr reversed its previous relationship, with a significantly lower scores in group 1 at 1 week (p=0.013), 3 months (p<0.001) and 6 months (p=0.003).
Conclusion
Chronic groin pain with no identifiable structural abnormality on imaging or clinical assessment is a complex condition that orthopaedic surgeons and sports physicians encounter on a regular basis. The onset can vary from insidious, longstanding and debilitating pain that does not respond to conservative treatment, to a sudden acute event.1 ,8 ,9 ,12 ,15–21 The syndrome has been described using various terminologies and the precise pathophysiology remains uncertain. Some have defined it as an ‘incipient’ posterior inguinal wall hernia17 ,22 attributable to deficiency of the transversalis fascia or dilatation of the internal inguinal ring, while others have correlated the condition with tears of the external oblique aponeurosis23 or the rectus abdominis insertion,24 or entrapment of the ilioinguinal nerve and its branches.25
Given the confusion regarding the origin of symptoms, it is unsurprising that debate on the best treatment method for this condition is ongoing.5 ,12 ,13 ,26 Further confounding our understanding, there is no robust system yet established to assess post-treatment outcomes, although successful postoperative response has sometimes been assessed by the degree of pain relief and the time needed to return to play.12 ,13 ,26 ,27
Non-operative methods such as rest, anti-inflammatory drugs and physiotherapy for muscle strengthening and core stability have been used, but often with limited success.14 ,27 Even when ultimately successful, these methods are often slow to take effect.28 ,29
Only a few trials of minimally invasive percutaneous treatment techniques have been reported previously. These have targeted the rectus abdominis or adductor longus insertions with steroid and local anaesthetic,30 ,31 or prolotherapy with 12.5% dextrose,32 ,33 with reasonable results at up to 1-year follow-up. Satisfactory relief of chronic groin pain for 2 months of follow-up was reported in a single patient using ultrasound-guided cryoablation of the genitofemoral nerve.34
Many have felt that the condition rarely fully improves without surgery,5 ,9 and often resort to surgical intervention after a brief trial of conservative measures. Regardless of specific technique, most of the surgical literature describes procedures aiming to reinforce the abdominal wall near the inguinal ligament, much like traditional hernia repair. Success rates ranging from 63% to 95%8 ,9 ,35 have been described. Other surgical techniques used for treatment include neurotomy of the ilioinguinal nerve36 and reattaching the inferolateral edge of the rectus abdominis muscle to the pubic bone and tenotomy of the adductor longus tendon.26 Given the broad range of operative approaches and success rates, and given the still obscure aetiology of the condition, it is possible that some or all of these techniques may have brought about symptom relief by some inadvertent denervation of the area, rather than by their theoretical design.
We postulated that pain could be successfully abolished without attempting to address the mechanical dysfunction or imbalance, by percutaneously denervating the region with radiofrequency energy. Currently, radiofrequency desensitisation of nerves is an emerging technique in the anaesthetic and pain management fields that is becoming increasingly popular, although its mechanism of action is not well elucidated.36
The preliminary results of this prospective randomised trial have demonstrated an improvement in pain and function scores both with RFD treatment and, in the very short term, with steroid and local anaesthetic injection. The results also show that RFD treatment is effective also in patients with previous failed surgery.
This suggests that pain is related to either nerve compression or tendon inflammation, or a combination of both, and is not necessarily directly related to posterior abdominal wall laxity (which was not addressed by the treatments administered to either group 1 2, and had already proven unsuccessful in group 3). Either treatment may therefore prove to be more efficacious as well as safer than traditional surgical methods, which involve repairing perceived posterior abdominal wall defects. This is particularly likely given the success seen with RFD treatment in the small group of patients who had remained symptomatic despite previous surgical repair.
The greater magnitude and duration of improvement seen with RFD treatment compared with anaesthetic and steroid injection demonstrates the efficacy of RFD in this application, and is concordant with results demonstrated for RFD in other applications.37
This study does have certain limitations. First, the sample size was small, as this was only a pilot study. Second, there were no physiotherapy-only or surgery-only groups for comparison, in order to further elucidate the pathophysiology of the condition. Third, although we believe that the LAAG questionnaire is useful for assessing patients’ functional status, it has not yet been validated and may be more valuable for assessing adductor dysfunction; at the time, we were not aware of any validated assessment of groin function to use in its place. Subsequently, a new questionnaire was designed and validated for the assessment of groin function.38
Finally, the follow-up period was relatively limited; we do not know for how long the patients will remain symptom-free, or if the underlying structural abnormality, now denervated, will continue to deteriorate, leading to more severe disability down the track. This is likely to be highly dependent on the still-obscure aetiology of the pain (ie, nerve dysfunction or tendonitis or abdominal wall weakness), the long-term efficacy of RFD in general and the success of concomitant physiotherapy and strengthening routines.
Our study has shown that using RFD in the treatment of cryptogenic chronic groin pain is safe and efficacious, at least in the short term; it is superior to anaesthetic and steroid injection. This novel technique could help athletes return to play quite quickly and defer any surgical intervention, if symptoms recur, to take place ‘out of season’.
Furthermore, the success of denervation suggests that the concept of posterior abdominal wall weakness as a cause of this condition may be incorrect, or at least immaterial. The fact that the abolition of inflammation and/or nerve conduction (whether by anaesthetic/steroid or by RFD) abolishes the pain in patients who may have been diagnosed with a ‘Sportsman's Hernia’ raises the possibility that the condition is primarily a tendonitis with a resultant neuropathy. This also brings into question the need for surgical intervention to repair perceived abdominal weakness.
Further larger studies with comparison to groups receiving surgery or physiotherapy alone, and with a longer duration of follow-up, are needed to complement this groundwork.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online Appendix1
Footnotes
-
Contributors HO, JC and GL worked on the manuscript. DC performed the procedures. JM and MW developed the LAAG scoring system, identified suitable patients.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval National Research Ethics Services (National Patients Safety Agency).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmjgroup.com