Article Text

Abstract
Background/aims Adult black athletes (BA) exhibit left ventricular hypertrophy (LVH) on echocardiography and marked ECG repolarisation changes resembling those observed in hypertrophic cardiomyopathy (HCM). Limited data are available for adolescent BA, the group most vulnerable to exercise-related sudden cardiac death.
Methods Between 1996 and 2011, 245 male and 84 female adolescent BA from a wide variety of sporting disciplines underwent cardiac evaluation including ECG and echocardiography. Athletes exhibiting T-wave inversions and/or echocardiographic LVH were investigated further for quiescent cardiomyopathies. Results were compared with 903 adolescent white athletes (WA) and 134 adolescent sedentary black controls (BC).
Results LVH on echocardiography was present in 7% of BA compared to only 0.6% of WA and none of the BC. In the very young (<16 years), 5.5% of BA, but none of the WA, demonstrated LVH. Within the BA group, LVH was more prevalent in men compared to women (9% vs 1.2%, p=0.012). T-wave inversions were present in 22.8% BA, 4.5% WA and 13.4% BC. T-wave inversions in BA occurred with similar frequency in men and women and were predominantly confined to leads V1–V4. T-wave inversions in the lateral leads, commonly associated with cardiomyopathies, were present in 2.4% of BA. On a further evaluation and mean follow-up of 8.3 years, none of the athletes exhibited HCM.
Conclusions Athletic training has a pronounced effect on adolescent BA. Black athletes as young as 14 years of age may exhibit left ventricular wall thicknesses of 15 mm and marked repolarisation changes resembling HCM. Male and female BA demonstrate a high prevalence of T-wave inversions.
- Cardiology prevention
- Exercise physiology
- Evaluation
- Cardiology
Statistics from Altmetric.com
Introduction
Ethnicity is an important determinant of the electrical and structural manifestations of an athlete's heart. Data from adult athletes of African/Afro-Caribbean descent (black athletes (BA)) demonstrate a sixfold increase in the prevalence of marked repolarisation anomalies and an eightfold increase in the prevalence of left ventricular hypertrophy (LVH) on echocardiography compared to Caucasian athletes (white athletes (WA)). Such phenotypes often complicate the differentiation between physiological remodelling and morphologically mild hypertrophic cardiomyopathy (HCM) in this ethnic group.1–5
Adolescent athletes are increasingly subject to preparticipation cardiovascular evaluations including a 12-lead ECG. Initial concerns regarding the presence of the juvenile ECG pattern have been negated, as only a small minority (0.8%) of the adolescent WA exhibit T-wave inversions beyond lead V2, resembling arrhythmogenic right ventricular cardiomyopathy (ARVC).6 ,7
The effect of African/Afro-Caribbean ethnicity on cardiac adaptation to exercise in adolescent athletes has not been elucidated comprehensively. Furthermore, there are no data on adolescent female BA. Data from the USA indicate that adolescent BA are particularly susceptible to sudden cardiac death (SCD),8–10 and therefore, the distinction between athlete's heart and cardiac pathology is of particular relevance in this group. The aim of this study was to identify the spectrum of physiological adaptation in highly trained adolescent BA.
Methods
Athletes
The study was part of a collaborative research programme between the UK and France. Between 1996 and 2011, 329 consecutive normotensive BA, aged 14–18 years and competing at the regional, national or international level, were evaluated. The data were compared with age-matched and sex-matched normotensive WA in similar sporting disciplines. Given the higher proportion of male participation, adolescent WA were matched for sex at a ratio of 1 BA: 2 WA for women and 1 BA: 3 WA for men. The final cohort of WA consisted of 903 individuals. All athletes were assessed with a health questionnaire, cardiovascular examination, 12-lead ECG and two-dimensional echocardiography. Ethnicity was self-assigned.
Adolescent black controls
The charitable organisation Cardiac Risk in the Young (CRY) offers cardiovascular evaluation for conditions predisposing to SCD to all young individuals (14–35 years), irrespective of athletic status. Evaluations are performed throughout the UK and are identical to those in athletes. As part of the recruitment of healthy black controls (BC) for several studies, we offered all African/Afro-Caribbean individuals attending a two-dimensional echocardiogram.
Between 1996 and 2011, 8926 individuals were assessed. Selection criteria for controls were black ethnicity, age 14–18 years, sedentary lifestyle (≤2 h of organised physical activity/week), absence of symptoms, drug history, family history of cardiomyopathy or premature (≤40 years) SCD, normal blood pressure and a structurally normal heart. The final cohort comprised 134 BC.
Electrocardiography
Standard 12-lead ECGs were performed as described elsewhere.1 Relating to repolarisation abnormalities, ST-segment shift was considered significant if ≥0.1 mV in ≥2 contiguous leads. Early repolarisation pattern was defined as J-point elevation ≥0.1 mV in ≥2 contiguous non-anterior leads. T-wave inversion was considered significant if ≥−0.1 mV in ≥2 leads (excluding aVR, V1 and III in isolation). Biphasic T-wave inversion was considered abnormal if the negative deflection of the T-wave exceeded ≥−0.1 mV. The distribution of T-wave inversions was categorised into anterior (V1–V4), inferior (II, III, aVF) and lateral (I, aVL, V5, V6). Deep T-wave inversions were defined as a T-wave deflection ≥−0.2 mV.6 All ECGs were read independently by two authors (SS and FC) in the UK and France.
Echocardiography
Two-dimensional echocardiography was performed using either a GE Vivid I (Tirat, Israel), Philips Sonos 7500, iE33 or CPX50 (Bothel, Washington, USA). Standard views were obtained and cavity and wall thickness measurements performed using established guidelines.11 Left atrial (LA) diameter and left ventricular (LV) internal diameter were measured from the parasternal long-axis view. Left ventricular wall thickness was measured in the parasternal short-axis view, at the levels of the mitral valve and papillary muscles; the greatest measurement was defined as the maximum left ventricular wall thickness (mLVWT). LVH was defined as an mLVWT >12 mm. Left ventricular mass was calculated with the formula of Devereux.12 Relative LV wall thickness (RLVWT) was calculated by dividing the sum of the LV septal and posterior wall thicknesses in diastole by the end diastolic LV internal diameter. Two-dimensional continuous-Doppler and pulsed-Doppler imaging were performed using standard parasternal and apical views.13 A cardiologist blinded to the athlete's identity reviewed all scans.
Further evaluation and follow-up
Athletes with T-wave inversions or an mLVWT >12 mm were investigated with an exercise stress test14 ,15 and Holter monitor to check for the broader phenotype of HCM. A significant proportion agreed to cardiac MRI (cMRI) with gadolinium injection.16 Several athletes underwent repeat cardiac evaluations in accordance with the policies of their sporting organisations, regardless of the baseline results.
Ethical approval/consent
Ethical approval was granted by the National Research Ethics Service, Essex 2 Research Ethics Committee in the UK and approved by the French Ministry of Health and Youth in France. Written consent was obtained from individuals ≥16 years and from a parent/guardian for those <16 years.
Statistical analysis
Statistical analyses were performed using SPSS software, V.17 (Chicago, Illinois, USA). Variables were tested for normality using the Kolmogorov-Smirnov test. Group differences were tested using Student's t-test or one-way ANOVA (analysis of variance) (Sidak test for post hoc analysis) and Mann-Whitney U test or Kruskal Wallis (Dunn's test for posthoc analyses) test for normally and non-normally distributed variables, respectively. The χ2 test or Fisher's exact tests were used as appropriate to test group differences of proportions.
Univariable analyses were performed to determine which variables (ethnicity, age, gender, body surface area, hours of exercise/week, LV cavity diameter in end-diastole (LVED) and LA size) were significantly associated with the presence of LVH on the echocardiogram of athletes. Univariable analyses were also performed to determine whether the same variables and mLVWT were associated with the presence of T-wave inversions and ST-segment elevation on the athletes’ ECG. Binary logistic regression analyses were used to determine the independence of the above associations. The goodness of fit was evaluated using the Hosmer-Lemeshow test. Significance was defined as p<0.05 (two-tailed) throughout.
Results
Demographics
Demographics of the study cohorts are outlined in table 1. Athletes competed in a wide range (n=29) of sporting disciplines, as illustrated in figure 1. Almost a third (28%) of the athletes were <16 years old. Black athletes exercised more hours per week compared to WA (13.2±5.4 vs 11.6±4.1 h; p<0.001).
Comparison of demographic and echocardiographic parameters between adolescent black athletes, white athletes and black controls

Sporting disciplines expressed as percentage (%) of the total black-and-white athlete cohort. Others: black athletes: gymnastics, n=5; baseball, n=3; cricket, n=3; water polo, n=3; table tennis, n=2; tennis, n=2; fencing, n=1; hockey, n=1; ice skating, n=1; netball, n=1; weight lifting, n=1. White Athletes: canoeing n=22; diving n=7; fencing n=6; hockey n=6; speed skating n=6; water polo n=6; badminton n=4; ballet n=3; hurling n=3; netball n=3; volleyball n=3.
Only one 15-year-old male black soccer player reported cardiac symptoms of exertional chest tightness, prompting further evaluation despite a normal ECG. No athlete reported a family history of cardiomyopathy, premature SCD or use of regular medications.
Ethnic differences in LV wall thickness
Black athletes exhibited a greater mLVWT compared to both WA and BC; the difference in mLVWT between BA and WA persisted even after indexing for body surface area (table 1). The greater mLVWT in BA was not associated with an increased LV cavity size compared to WA. Relative LV wall thickness was greater in BA compared to WA (table 1). In absolute terms, LVH was present in 7% of BA (n=23) compared with 0.6% of WA (n=5) and none of the BC (figure 2). The mLVWT did not exceed 15 mm in BA and 13 mm in WA. The pattern of LVH in all athletes was concentric, and athletes with LVH exhibited normal or increased LV cavity size (mean 52.1±5.2 mm; range 42–60 mm) with normal diastolic function.

Histogram demonstrating the distribution of maximal left ventricular wall thickness as a percentage (%) of the total black athlete (black bars), black control (grey bars) and white athlete (white bars) cohorts. Seven per cent of black and 0.6% of white athletes exhibited left ventricular hypertrophy.
Ethnic differences in mLVWT persisted in athletes aged <16 years old, with BA exhibiting a mean mLVWT of 9.8±1.5 mm vs 9.1±1.1 mm in WA, p<0.001. Of interest, 5.5% of BA in this particular age group exhibited LVH compared to none of the WA.
Ethnic differences in ECG repolarisation changes
Black athletes demonstrated a higher prevalence of ST-segment elevation, T-wave inversions and deep T-wave inversions compared to WA (table 2). T-wave inversions in BA were predominantly observed in the anterior leads V1–V4 (14.3%), although a significant proportion of BA also exhibited T-wave inversions in the inferior (6.1%) and lateral (2.4%) leads (figure 3).
ECG characteristics of adolescent black athletes, white athletes and black controls

Histogram depicting the prevalence, distribution and nature of T-wave inversions (TWI) as a percentage (%) of the total black athlete (black bars), black control (grey bars) and white athlete (white bars) cohorts.
Black athletes also revealed a higher prevalence of early repolarisation pattern compared to WA (34.7% vs 21.1%, p<0.001). The commonest ST-segment morphology in the inferior leads was a rapidly ascending ST-segment in both groups, with only 7.7% of the total BA and 1.6% of the total WA cohort (p<0.001) exhibiting early repolarisation in the inferior leads with associated horizontal or descending ST-segment.
Black athletes versus black controls
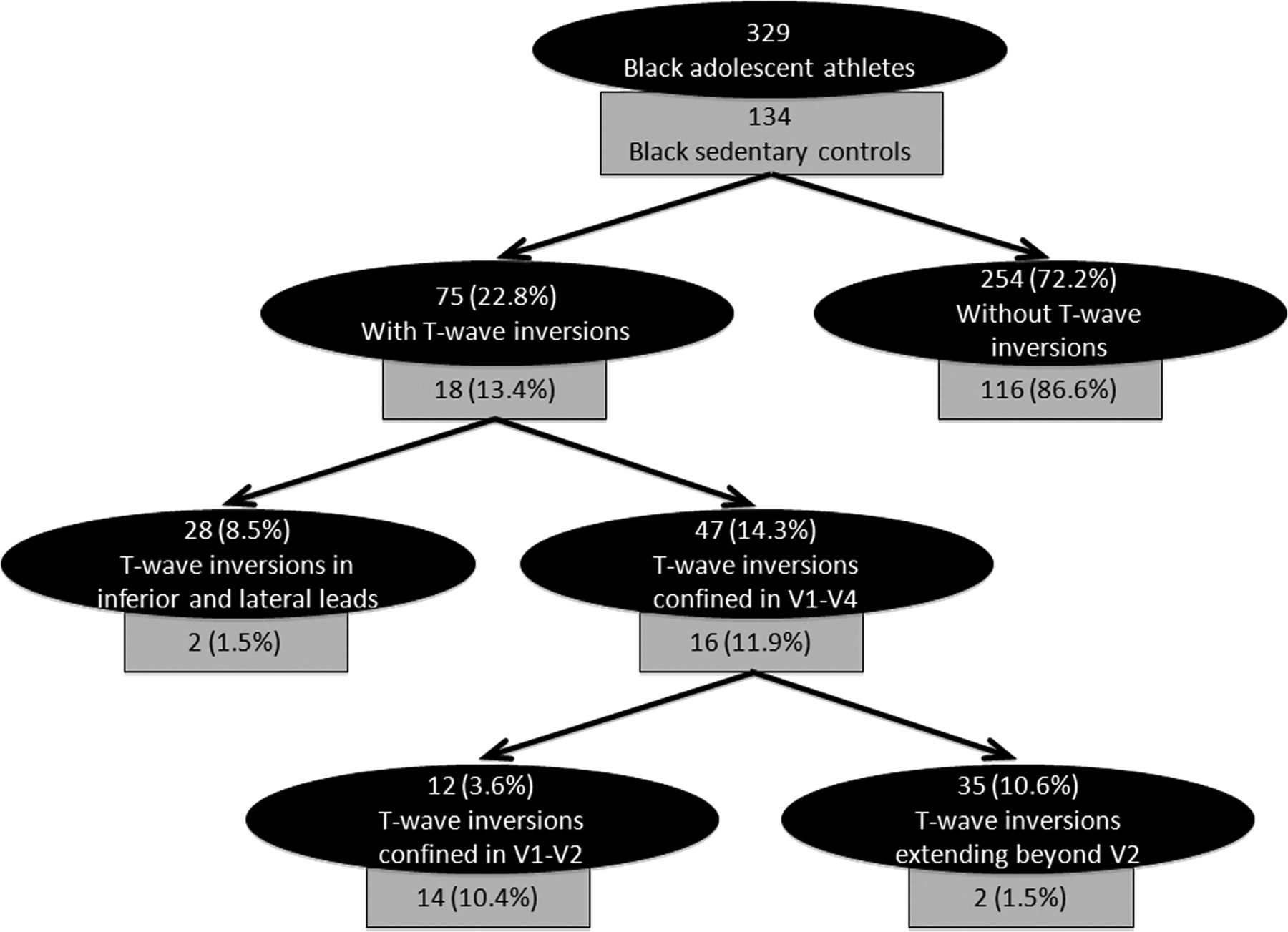
ST-segment elevation was present in almost 50% of both BA and BC. ST-segment depression was rare, regardless of athletic training, race or gender. T-wave inversions were more common in BA compared to BC (table 2). As with BA, the majority (89%) of T-wave inversions observed in BC were confined to the anterior leads (figure 4). In BA with anterior T-wave inversions, the majority (74%) extended beyond V2 and their prevalence did not vary with age (13.3% for <16 years vs 15.1% for ≥16 years, p=0.310). In contrast, only 12% of controls with anterior T-wave inversions showed T-wave inversions beyond V2 (figure 4). Most T-wave inversions in controls were observed in those <16 years old (16.7% <16 years vs 4% ≥16 years, p<0.030), suggesting that the majority represented the juvenile pattern.

Diagrammatic representation of the prevalence and distribution of T-wave inversions in black athletes (black boxes) and black controls (grey boxes). Numbers in brackets express percentages (%) of each cohort.
Sex differences in athletes
Female athletes demonstrated a smaller mLVWT compared to men in both ethnic groups (9.2±1.1 mm vs 10.3±1.5 mm, p<0.001 for BA; 8.7±1.1 vs 9.5±1.2 mm, p<0.001 for WA). Female BA exhibited a larger mLVWT compared to female WA (9.2±1.1 mm vs 8.7±1.1 mm, p<0.001). None of the female WA revealed an mLVWT >11 mm. In contrast, two female BA revealed an mLVWT >11 mm and up to 13 mm (figure 5).

Histogram illustrating the distribution of maximal left ventricular wall thickness as a percentage (%) of the total female white athlete (light red bars), female black athlete (dark red bars) and male black athlete (blue bars) cohorts. Nine per cent of male black athletes and 1.2% of female black athletes exhibited left ventricular hypertrophy.
Among BA, there was a lower prevalence of ST-segment elevation in female athletes compared to male athletes (table 3). T-wave inversions were more prevalent in men, but this did not achieve statistical significance. The distribution of T-wave inversions was similar in both sexes. Importantly, while deep T-wave inversions were identified in a significant proportion of male BA (9%), they were absent in female BA.
ECG repolarisation characteristics of adolescent black male and female athletes
Reliability of LVWT measurements in athletes
The averaged coefficients of variation between intraobserver and interobserver reliability for mLVWT measurements were 3.2% and 5.4%, respectively.
Determinants of LV remodelling and repolarisation changes in athletes
Determinants of LVH
Multivariable analyses revealed that male sex (OR 2.4; 95% CI 1.33 to 4.17, p=0.003), black ethnicity (OR 2.3; 95% CI 1.66 to 3.20, p<0.001) and ST-elevation (OR 2.18; 95% CI 1.49 to 3.18, p<0.001) were the strongest independent predictors of LVH. Other predictors included age (OR 1.22; 95% CI 1.05 to 1.43, p=0,011) and LA size (OR 1.06; 95% CI 1.01 to 1.11, p=0.018).
Determinants of ST-segment elevation and T-wave inversions
Multivariable analyses revealed that male sex (OR 2.22; 95% CI 1.37 to 3.70, p=0.001), black ethnicity (OR 1.57; 95% CI 1.12 to 2.22, p=0.010) and an increasing mLVWT (OR 1.16; 95% CI 1.01 to 1.32, p=0.033) were all independent predictors for ST-segment elevation.
Multivariable analyses revealed that black ethnicity (OR 3.22; 95% CI 2.09 to 4.94, p<0.001) and mLVWT (OR 1.21; 95% CI 1.03 to 1.42, p=0.017) were the only independent predictors for T-wave inversions.
Further evaluation
All 133 individuals with T-wave inversions and/or LVH on echocardiography were investigated with exercise testing and a Holter monitor. A considerable proportion (n=55; 41%) underwent cMRI including 89% of athletes with inferior and lateral T-wave inversion. None of these individuals exhibited any phenotypic features consistent with HCM during initial evaluation or subsequent clinical surveillance.
Long-term follow-up
Of all 1232 athletes, follow-up data were available in 503 (40.8%) over a mean period of 99.1±47.6 months. During this period, one fatality was reported in a 15-year-old male BA who had described exertional chest tightness. The 12-lead ECG, transthoracic echocardiogram, exercise stress test and 24 hour ambulatory ECG showed no significant abnormalities, although satisfactory images of the origin of the right coronary artery could not be obtained. Postmortem examination revealed an anomalous origin to the right coronary artery from the left aortic sinus, coursing between the aorta and the pulmonary trunk.17
We observed resolution of T-wave inversions in some athletes who were persuaded to detrain (figures 6A,B). Athletes with T-wave inversions who refused to detrain and exercised continuously over the follow-up period showed a deepening of T-wave inversions (figure 6C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
ECG examples of repolarisation abnormalities in black athletes. (A1) 16-year-old football player of Nigerian ethnicity exhibiting T-wave inversions in the anterior precordial leads. (A2) ECG from the same athlete after a period of detraining, illustrating a resolution of the T-wave inversions. (B1) 17-year-old football player of Ghanaian ethnicity exhibiting T-wave inversions in the anterior precordial, inferior and lateral leads. (B2). ECG from the same athlete after a period of detraining, illustrating a resolution of all T-wave inversions. (C1) ECG from a 16-year-old professional football player exhibiting ST-segment elevation and deep T-wave inversions in leads V1–V3. (C2) ECG from the same athlete 12 years later at the age of 28; note the progression of the deep T-wave inversions, despite the individual remaining asymptomatic and event-free.
Discussion
There is limited information on the effect of black ethnicity on cardiovascular adaptation in adolescent athletes, although both black ethnicity and adolescence appear to confer a significant risk of SCD from HCM.8 ,10 A recent study reported a high prevalence of repolarisation changes in adolescent black soccer players.18 Although useful, the conclusions drawn from that study are limited, given the single sporting discipline assessed, absence of female athletes and absence of a control group. This study attempted to elucidate the prevalence and significance of LVH on echocardiography and repolarisation changes in black male and female adolescent athletes competing in a wide variety of sporting disciplines.
Ethnic differences in left ventricular remodelling in adolescent athletes
Consistent with studies in adult athletes, adolescent BA demonstrated greater mLVWT compared to WA. Contrary to the concept that children exhibit limited structural adaptation to exercise, our study demonstrated that 7% of adolescent BA revealed an mLVWT >12 mm, and up to 15 mm. Importantly, almost 25% (n=5) of BA with LVH were <16 years old. In contrast, only 0.6% (n=5) of adolescent WA exhibited LVH but never >13 mm; all were >16 years old. The quantitative differences between the two ethnicities were most profound in men; however, even among female athletes, there were appreciable ethnic differences. While none of the female WA revealed an mLVWT >11 mm, we identified an mLVWT >11 mm in two female BA.
During subsequent investigations of athletes with LVH, none exhibited features suggestive of HCM. Based on these results, it is reasonable to infer that outside the context of symptoms or a family history of HCM, an absolute mLVWT of 15 and 13 mm probably represents the physiological upper limit of LVH in male and female adolescent BA, respectively.
Ethnic differences in repolarisation changes in adolescent athletes
The prevalence of both T-wave inversions and ST-segment elevation in adolescent BA was comparable to that reported in adult BA.1 A remarkable number of female BA (16.7%) showed T-wave inversions of distribution similar to male BA (table 3). Consistent with recent studies in adult athletes, the prevalence of early repolarisation in the inferior and lateral leads was common in our cohort and more prevalent in BA compared to WA. ST-segment depression was rare in all groups, indicating the need for further investigations and clinical surveillance when this abnormality is observed.
T-wave inversions
T-wave inversions were most commonly identified in the anterior leads in all individuals of black ethnicity, irrespective of athletic activity (figure 3). Almost 75% of athletes with anterior T-wave inversions demonstrated T-wave inversions beyond V2. In contrast, almost 90% of anterior T-wave inversions in the sedentary group were confined to leads V1 and V2 (figure 4) and usually in individuals aged <16 years old. Our results indicate that while T-wave inversions in leads V1 and V2 may reflect a juvenile ECG pattern, extension beyond V2 and up to V4 would favour an athlete's heart. This notion is supported by previous observations in adult athletes, which revealed a similar percentage of BA with anterior T-wave inversions.1
T-wave inversions in the inferior and lateral leads were more prevalent in BA compared to the control group with figures similar to those observed in adult athletes.1 Although the precise significance of these repolarisation patterns have not been fully elucidated, the authors noted a resolution of T-wave inversions following detraining, regardless of their distribution (figure 6A,B).
While we believe that T-wave inversions in V1–V4 in BA are probably benign, we have previously recommended that T-wave inversions in the lateral leads should be viewed with caution based on our experience of 2 aborted SCDs in BA with this repolarisation pattern.1 However, the presence of lateral T-wave inversions with the same frequency between adult1 and adolescent BA, their resolution with detraining, and the absence of an association with any cardiomyopathy phenotype on echocardiography or cMRI infer that such repolarisation changes may represent an ethnic variant in the majority. All athletes with T-wave inversions in the lateral leads remained free of adverse cardiac events during an average follow-up period of over 8 years. When one takes into consideration that almost 2.5% of adolescent BA exhibit T-wave inversions in the lateral leads, it is statistically improbable that all such athletes harbour a sinister cardiomyopathy or ion channelopathy. Deep T-wave inversions were only identified in male BA, and therefore, it may be reasonable to recommend further evaluation in female BA harbouring such repolarisation anomalies.
It is prudent to emphasise that our observations are based solely on comparisons between healthy athletes and controls. We were unable to make direct comparisons with ECGs in adolescent patients with HCM; therefore, until such data are available, it would be our policy to continue comprehensive evaluation and diligent surveillance in adolescent BA with lateral T-wave inversion. Our data provide some reassurance that isolated T-wave inversions in BA, irrespective of the territory, should not preclude competitive sport if subsequent investigations are normal.
Clinical implications
Preparticipation screening with 12-lead ECG is an increasingly global phenomenon.19 ,20 Although updated guidelines on the interpretation of an athlete's ECG make some allowance for African ethnicity,21 the criteria for further cardiac evaluation still rely on data from Caucasian athletes.22 If consideration is given to T-wave inversions alone, almost 23% of the adolescent BA would fail the initial preparticipation screening and warrant further investigations. The issue is complicated further because 7% of adolescent BA in our study exhibited LVH, which in the context of coexistent repolarisation anomalies poses significant challenges in differentiating physiological LVH from HCM.
Data from WA suggest that women exhibit lesser quantitative ECG changes compared with men,6 ,7 particularly with respect to T-wave inversions, and therefore, it is usually the male athletes that are affected by false-positive results. Our study, however, revealed that up to 17% of black women could potentially be affected by a false-positive test if current ECG interpretation guidelines are applied, further emphasising the need for age-specific, sex-specific and ethnicity-specific guidelines.
Limitations
Despite extensive investigations, this study failed to identify any individual with HCM or ARVC. This may be attributable to a relatively low number of athletes studied when one considers the prevalence of either disorder. Moreover, the prevalence of both disorders, based on phenotypic expression, is probably lower in the paediatric population since it is recognised that gene carriers may not exhibit the phenotype until early adulthood. In this regard, the investigators recognise that they may have failed to identify an athlete harbouring HCM or ARVC who is yet develop the disease phenotype. In order to fully elucidate the significance of the ECG and echocardiographic features observed, the authors endeavour to continue clinical surveillance of evaluated athletes in the context of an international collaboration, with a view to reporting longer term outcomes in a large cohort of adolescent BA.
Conclusion
Adolescent BA exhibit a significantly higher prevalence of repolarisation changes and LVH than adolescent WA. Our results underscore the need for ethnicity-specific criteria for differentiating normal cardiac adaptation to exercise from cardiomyopathy.
What are the new findings?
-
Even adolescent black athletes may develop significant left ventricular hypertrophy, in response to exercise, of up to 15 mm.
-
The prevalence of T-wave inversions in adolescent black athletes is comparable to the prevalence reported in adult athletes (23%).
-
Female black adolescent athletes exhibit a similar prevalence of T-wave inversions but a lower prevalence of ST-elevation compared to men. However, deep T-wave inversions are rare in adolescent female athletes.
-
In black controls, there appears to be a high prevalence of the juvenile ECG pattern.
How might it impact on clinical practice in the near future?
-
Both male and female black adolescent athletes develop significant repolarisation changes, in response to athletic training, which must be taken into account during the preparticipation screening process.
-
Black male adolescent athletes may develop significant left ventricular hypertrophy, which must be taken into account during the preparticipation screening process.
-
Our data emphasise the need for age-specific, sex-specific and ethnicity-specific guidelines for the purpose of preparticipation cardiovascular evaluation.
Acknowledgments
The authors would like to thank CRY for providing portable echocardiography equipment and ECG machines used for the study in the UK. The authors acknowledge Dr Siransky (Abidjan, Ivory Coast), Bako Tchiouake (Niamey, Niger) and Dr Uzan from INSEP (Paris, France) who assisted in the collection and collation of data.
References
Footnotes
-
Contributors NS, GK, SGh, AZ, SGa, JR and MW carried out the study design, data collection and preparation of the manuscript. MP and FC were involved in the interpretation of the data and revision of the manuscript for intellectual content. VF carried out the study design, data collection, statistical analysis and preparation of the manuscript. SS was the lead for the study and was involved in the study design, data collection, quality control of data and preparation of the manuscript.
-
Funding NS, MP, JR, SGa, AZ and SGh were funded by research grants from CRY. SS has been a coapplicant on previous grants from CRY to study African∕Afro-Caribbean athletes. Studies on French athletes were supported by grants from the Club des Cardiologues du Sport and the French Ministry of Health and Sport.
-
Competing interests None.
-
Ethics approval National Research Ethics Service, Essex 2 Research Ethics Committee in the UK and the French Ministry of Health and Youth in France.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com