Article Text

Abstract
Background Heading impairs cognition in the short and medium-terms; however, little is known about the long-term consequences. This study aimed to investigate the hypothesis that chronic low-level head trauma is associated with persistent cognitive decline.
Methods All members of Former Player Associations (FPAs) from four professional football clubs in the UK were contacted to participate in the study. Participants were required to complete a self-assessed test of cognition, the Test Your Memory questionnaire. Further information was collected from respondents in order to analyse the potential effect of a number of variables on cognition.
Results 10 of 92 respondents (10.87%) screened positive for possible mild cognitive impairment (MCI) or dementia. There was no association between low-risk and high-risk playing positions (HR = 0.40, p = 0.456) or length of playing career (HR = 1.051 95% CI 0.879 to 1.257, p = 0.586) and a positive screening result. Age was a risk factor (HR = 1.137 per additional year, 95% CI 1.030 to 1.255, p < 0.05), although this was not significantly different from the population prevalence across age groups.
Conclusions These results suggest that once a player ends their playing career, their risk of harm falls in line with the population, suggesting either that changes are reversible or that heading may not be as harmful as commonly thought. Future longitudinal studies of large numbers of professional football players are needed to support the findings from this study.
- Aging
- Concussion
- Epidemiology
- Neurology
- Soccer
Statistics from Altmetric.com
Background
Animal models have demonstrated that subconcussive trauma leads to increased β-amyloid burden and a dementia-type syndrome,1 but less is known about the long-term effects of subconcussive trauma on humans.2 Association Football provides a human model where participants are exposed to chronic repetitive low impact head trauma through the act of heading—an integral skill and unavoidable component of the game known to result in white matter changes and impaired cognition.3 ,4 The frequency of headers during a season is correlated with poor cognitive performance, placing professional players, who on average head the ball 800 times a season, at particular risk.5 ,6 Previous studies show recently retired players to have significant cerebral atrophy and impairment of attention, memory, concentration and judgement when compared to age-matched controls.7 ,8 These concluded heading to be the likely cause. However, little is known about the long-term consequences of heading on cognition and executive function. This study aimed to gather preliminary data to investigate the hypothesis that chronic low level head trauma is associated with long-term cognitive decline and a potential risk factor for dementia.5
Methods
All members of the Former Player Association (FPAs) from four professional football clubs in the UK (two in Scotland and two in England) were contacted via their respective associations to participate in the study. Participants were required to complete a self-assessed test of cognition, the Test Your Memory (TYM) questionnaire. Postal surveys were used for practicality and to increase the likelihood of participation. The self-administered TYM screening test correlates significantly better than the Mini-Mental State Examination in detecting cognitive impairment (R2=0.78 vs 0.55) when compared with a full cognitive battery.9 It is also validated for use in non-hospital settings.9 ,10 The questionnaire is self-administered in order to remove assessor bias and is therefore useful in postal surveys.11
Participants returned the questionnaires either directly to the research team or via the FPAs. The sole exclusion criterion was age. Respondents under the age of 55 were removed from the final analysis due to the lack of clinical evidence and negligible prevalence rates of cognitive impairment in this age group.12 This age cut-off also ensured that our analysis included only those at risk of displaying long-term impairment, distinguishing it from previous short-term and medium-term studies.
The study was approved by the local ethics committee.
The questionnaires were collated and results obtained in order to establish a final score for each participant. A positive screening result for possible mild cognitive impairment (MCI) is shown by a score of less than 47 of 50 in the below 70 age group, 46 of 50 in those aged 70–79 years and 45 of 50 in those aged over 80 years. A score of less than 43 has a sensitivity of 93% in those with dementia. Particular attention was paid to the final component—short sentence recall. Those with MCI and dementia tend to struggle with this test of anterograde memory.11 Participants who scored below the threshold and had problems with sentence recall were considered positive for possible MCI at this screening stage. There was no additional follow-up.
Further information was collected from respondents in order to analyse the potential effect of a number of different variables on cognition. These included age, length of career and playing position—as some positions involve a greater exposure to heading risk. The contributions of these variables to a positive screening test were assessed using Cox regression analysis. Differences in prevalence between age groups in our sample as compared to the UK male population were assessed using χ2 analysis. Differences between group characteristics within our study were compared using t-tests. All analyses were performed in SPSS (SPSS Inc, V.19).
Results
Three hundred questionnaires were sent to four players associations. A total of 138 former professional football players completed and returned the TYM assessment, giving a response rate of 46%. Of these, 92 met the inclusion criteria. The mean age of those included in the study was 67.45 years (±6.96, 95% CI); the mean length of the professional playing career was 13.84 years (±4.67, 95% CI) years. 8.7% of respondents were goalkeepers; 30.4% played the majority of their career in defence, 27.2% in midfield positions and 33.7% in forward or striking positions (figure 1).

Questionnaire distribution, returned screening tests, results and playing positions of respondents (95% CIs).
In total, 10 of the 92 respondents (10.87%) scored less than the cut-off for their age and therefore screened positive for possible MCI. Of these, two respondents scored well beneath the cut-off—25/50—for possible dementia (6/50 and 7/50, respectively). All eight respondents with possible MCI had difficulty with the sentence recall task, adding further validity to their low score.
There were no statistically significant differences between goalkeepers and other playing positions (table 1). Length of playing career among those who screened positive for MCI was no different than for the negative group (t test, p=0.26), and the increase in risk of a positive screening result for each year of the professional career was not significant (table 1). As expected, there was a positive correlation between age and positive screening tests (table 1) and a significant difference between the mean age of those in the MCI screen positive group and the negative group (t test, p<0.05).
Sport-specific and demographic risk factors for a positive cognitive impairment screening test in former professional football players
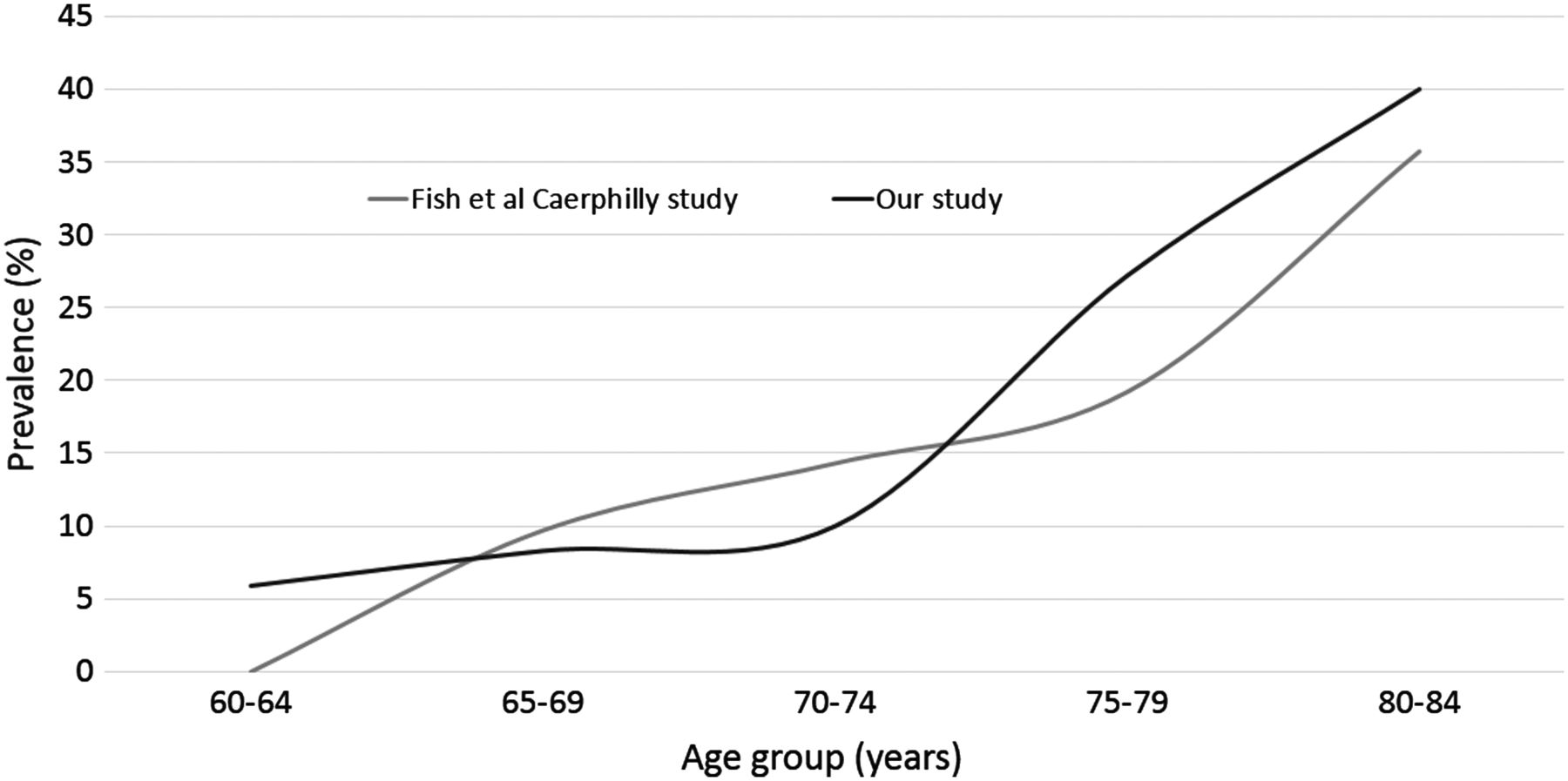
Comparison with the only large UK-based MCI prevalence study of men demonstrated no statistical significance between cognitive impairment among our sample of ex-professional footballers and a large sample of men in Wales.13 This was true across all age groups over 65 divided into 5-year groups: 65–69 (χ2 (1), p=0.92), 70–74 (χ2 (1), p=0.68), 75–79 (χ2 (1), p=0.65), 80–84 (χ2 (1), p=0.94). The pattern of similarities can be seen in figure 2.
{kind=link}
{kind=link}
The prevalence of positive screening tests for dementia/mild cognitive impairment in British men by age group. A comparison between the normal population and retired professional footballers.
Conclusions
Our findings counter a number of previous studies which have suggested that chronic subconcussive head injury in football may be a risk factor for accelerated cognitive decline.5 ,14–,16 These surprising results are supported by the lack of any statistical difference in cognitive performance on the TYM test between players in positions with very minimal exposure to heading—goalkeepers—and those for whom heading the football is a frequent and unavoidable occupational hazard. This suggests that the short-term and medium-term cognitive decline caused by heading may only be transient.17 ,18 The discovery that an extended length of playing career did not significantly add to the risk of a positive screening may be seen as further evidence of this and supports previous studies which failed to find any significant neurological consequences of heading.3 ,18 ,19 Our findings are supported by a similar prevalence of MCI in British men identified by the Caerphilly Study.13
This study has a number of limitations including a relatively small sample size and the potential for selection bias. Being a member of a former player association may preselect individuals who are cognitively able to maintain this link and who were able to understand the nature and instructions of the TWM test. However, a number of the surveys returned showed evidence of cognitive decline, and in two cases this was severe. No premorbid information on intellectual level was available, but reassuringly, difficulties with anterograde memory recall were seen in all failed screening tests, suggesting that low scores were genuine and not solely due to low IQ. In the absence of detailed information regarding non-responders, an impressive response rate was reassuring, although we did not have detailed information on known risk factors such as previous concussions and drug and alcohol intake.2 Finally, the use of self-administered questionnaires may be less accurate than alternative data collection methods, but an encouraging range of final test scores from participants suggested that respondents were completing the assessments appropriately and as instructed.20
Despite these limitations, it is useful to note that players experiencing prolonged exposure to multiple head trauma continued to remain cognitively intact well into later life. Indeed, the two eldest respondents—81 and 86 years old, respectively spent 13 years heading a leather ball without any significant decline in their scores on the TYM test (scoring 50/50 and 47/50 on their respective tests). These results provide some evidence against the present thinking that head injury or concussion is chronically damaging to neurological health.
Future longitudinal studies of large numbers of professional football players are needed to support the findings from this study.
Acknowledgments
This research was supported by the National Institute for Health Research (NIHR) Academic Foundation Programme and Newcastle upon Tyne Hospitals (NUTH) NHS Foundation Trust and Newcastle University. The views expressed are those of the authors and not necessarily those of the NHS, NUTH, the NIHR or the Department of Health
References
Footnotes
-
Contributors SAVJ was involved in study design, data collection and collation, literature review and initial and early drafting of manuscript. RWB was involved in the statistical analysis, literature review, manuscript editing, and final preparation of manuscript. PJE was involved in document editing, figure and table formatting, and final editing.
-
Competing interests None.
-
Ethics approval Newcastle University.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com