Article Text

Abstract
Background As one of the purposes of anterior cruciate ligament reconstruction (ACLR) is to return athletes to their preinjury activity level, it is critical to understand variables influencing return to sport. Associations between return to sport and variables representing knee impairment, function and psychological status have not been well studied in athletes following ACLR.
Purpose The purpose of this review was to summarise the literature reporting on variables proposed to be associated with return to sport following ACLR.
Study design Systematic review.
Methods Medline, EMBASE, CINAHL and Cochrane databases were searched for articles published before November 2012. Articles included in this review met these criteria: (1) included patients with primary ACLR, (2) reported at least one knee impairment, function or psychological measure, (3) reported a return to sport measure and (4) analysed the relationship between the measure and return to sport.
Results Weak evidence existed in 16 articles suggesting variables associated with return to sport included higher quadriceps strength, less effusion, less pain, greater tibial rotation, higher Marx Activity score, higher athletic confidence, higher preoperative knee self-efficacy, lower kinesiophobia and higher preoperative self-motivation.
Conclusions Weak evidence supports an association between knee impairment, functional and psychological variables and return to sport. Current return to sport guidelines should be updated to reflect all variables associated with return to sport. Utilising evidence-based return to sport guidelines following ACLR may ensure that athletes are physically and psychologically capable of sports participation, which may reduce reinjury rates and the need for subsequent surgery.
- Knee ACL
- Sports rehabilitation programs
- Physiotherapy
- Psychology
Statistics from Altmetric.com
Background
Anterior cruciate ligament (ACL) tears are the most commonly reported knee injury in athletes, with nearly 300 000 ACL reconstructions (ACLRs) performed yearly in the USA.1 Previous reports indicate that 98% of orthopaedic surgeons recommend surgery if patients wish to return to sport,2 but not all patients return to sport following ACLR. Clinical guidelines suggest that patients should be expected to return to sport by 9 months postsurgery, but many patients have not achieved this activity level up to 18 months after receiving clearance to return to sport.3 Declines in sports participation compared with preinjury levels are noted as far as 5 and 7 years postsurgery,4–7 though reasons for activity level changes may be unrelated to knee function.
Improved understanding of variables influencing patients’ ability to return to sports is needed. Return to sport recommendations following ACLR are varied and often based on clinical experience or reviews reporting the criteria utilised in randomised controlled trials (RCTs).8–11 Most return to sport criteria following ACLR includes assessments of knee impairment and function, such as knee range of motion (ROM), quadriceps strength and functional test performance. Achieving knee ROM equivalent to the uninvolved limb is frequently emphasised12–17 as ROM asymmetry between limbs has been linked to worse subjective outcomes 10 years postsurgery, though the ability of these patients to return to sport is unknown.18 Quadriceps and hamstring strength are the most commonly utilised objective criteria when determining patient readiness to return to sport,13 ,14 ,16 ,19–26 and published reports note persistent quadriceps weakness years after surgery.27 ,28 Typical criteria include a quadriceps limb symmetry index (LSI) equivalent to >80–90% of the opposite side.13 ,14 ,16 ,19–26 Although quadriceps weakness may alter knee kinematics during running and cutting,29 the actual relationship between quadriceps strength and functional test performance such as hop testing is unclear.30–34 Single-leg hop LSI ≥90% is also often cited,15 ,23 ,25 ,35–38 but the relationship between functional test performance and athletic performance is not well established.39 Despite postsurgical emphasis on strengthening and functional performance, abnormal lower limb kinematics are evident during hopping and jumping 2–4 years following ACLR.40 ,41 The ability of these frequently utilised clinical criteria to predict athletes’ ability to return to sport is unknown.
Some patients without impairments in ROM or strength may choose not to return to their preinjury level of sports participation for reasons unrelated to knee function, such as lifestyle changes. Conversely, some patients reporting substantial knee impairments after ACLR return to competitive sport.42 Psychological variables may partially explain the lack of association between physical function and return to sport.43–45 Fear of movement and reinjury, or kinesiophobia, is one of the most commonly cited reasons for patients not returning to sport following ACLR.46 Although kinesiophobia declines during rehabilitation,47 it is still reported in as high as 20–24% of patients.6 ,48 Higher perceived self-efficacy (one's judgement about whether one can perform a task)49 ,50 and an internal health locus of control51 ,52 have been linked to better quality of life scores, knee function and subjective outcomes post-ACLR. Despite these reports, psychological measures are not typically used in current return to sport criteria following ACLR.
The evidence supporting current clinical criteria used to allow patients to return to sport following ACLR has not been thoroughly examined. The primary purpose of this systematic review was to summarise the published literature reporting on knee impairment, functional and psychological variables proposed to be associated with return to sport following ACLR. Knowledge of variables associated with athletes’ return to play following surgery may aid clinicians in counselling patients and focusing rehabilitation programmes. The secondary purpose of this review was to provide recommendations for future research to develop evidence-based return to sport criteria.
Methods
Search strategy
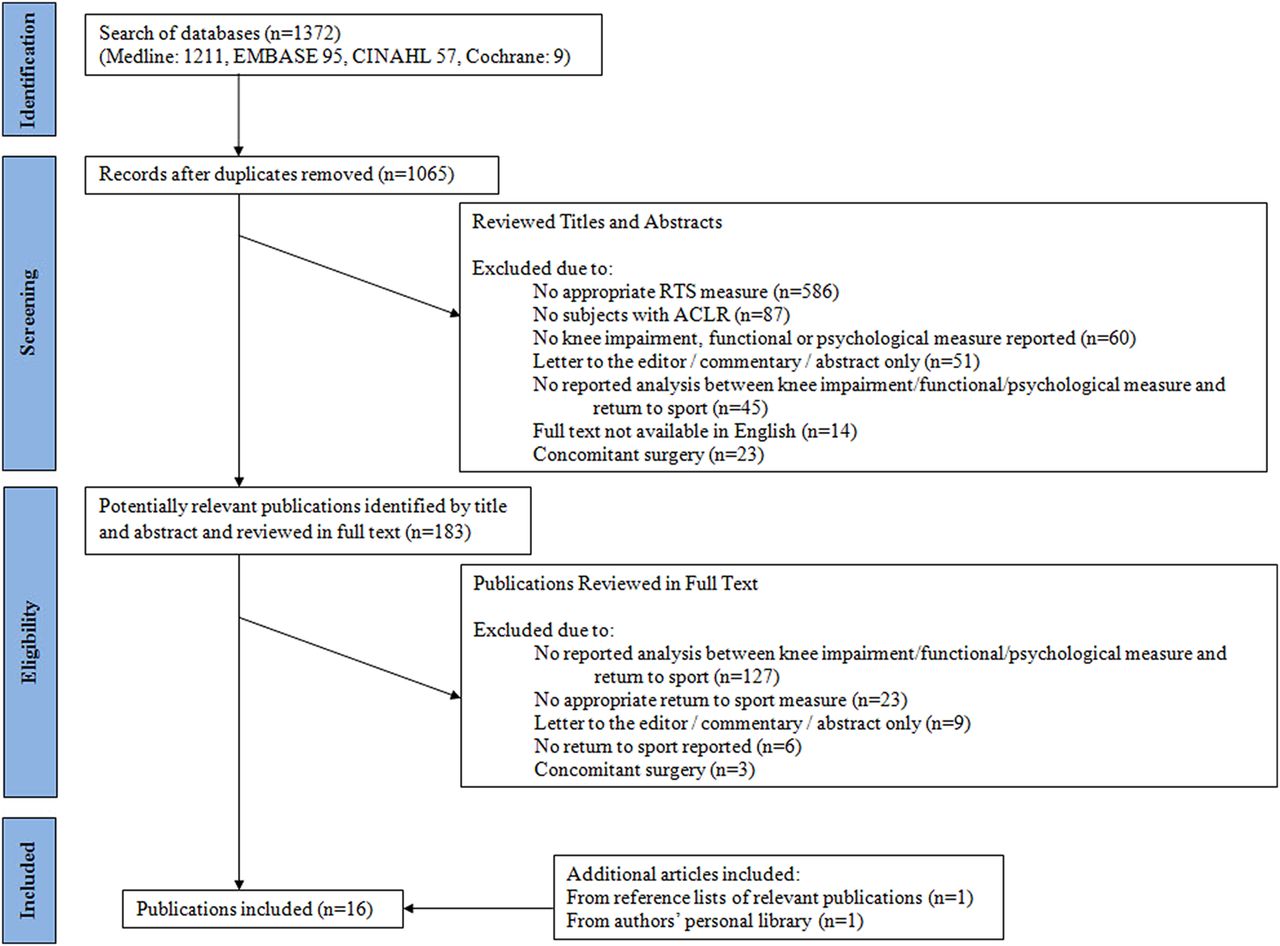
Medline, CINAHL, EMBASE and the Cochrane Database were searched for articles published in print or electronically prior to November 2012. Subject mapping and key words were used for each search engine, including ACL surgery and/or injury, preoperative care, postoperative care, ROM, muscle strength, proprioception, kinesiophobia, psychological, recovery of function and return to sports/return to play/sports re-entry. A reference librarian assisted with the database searches. A sample search is shown in online supplementary appendix 1. Two board-certified orthopaedic physical therapists independently applied the inclusion/exclusion criteria to these articles. The preferred reporting items for systematic reviews and meta-analyses flow diagram of the search results is shown in figure 1.53

{kind=link}
Preferred reporting items for systematic reviews and meta-analyses flow diagram of search results.
Selection criteria
Inclusion criteria for the articles selected were: (1) patients had undergone primary ACLR, (2) English language, (3) at least one knee impairment, functional or psychological measure was reported, (4) return to sport (defined as any sport, the same sport and the same level of preinjury sport at any postsurgical timeframe) was reported via subjective report or any measure directly identifying the patients’ level of active sports participation, such as the Tegner activity score or study-defined criteria and (5) studies contained statistical analyses examining the association between variables of interest and return to sport. Exclusion criteria were concomitant surgery of other ligaments or microfracture surgery. Concomitant meniscectomy or meniscal repair, or history of contralateral ACLR was permitted. Studies simply identifying whether patients could perform sport-related tasks but not reporting actual return to sport were excluded. Thus, measures such as the International Knee Documentation Committee (IKDC) objective form score, Cincinnati Knee Rating Scale score and the Lysholm Knee Score did not meet the definition of a return to sport measure for this review. Two reviewers independently reviewed titles and abstracts, then full text of potentially relevant articles, and attained consensus on articles to be included in the review.
Data extraction and analysis
Once articles meeting the inclusion criteria were identified, the lead author independently extracted information from each article. Information identified for descriptive analysis included study population, follow-up timeframe, preinjury athletic participation, return to sport rate, knee impairment and functional outcomes, psychological outcomes and statistical analyses relating variables of interest to return to sport. If data such as return to sport rate were not directly reported within a study, it was calculated with available data. A second reviewer confirmed all information. As a framework for data analysis, strength of evidence was classified according to Logerstedt et al54 Evidence is considered strong when supported by numerous high-quality RCTs, moderate when supported by either a single high-quality RCT or numerous low-quality RCTs or cohort studies, and weak when supported by retrospective or case controlled studies.
Assessment for risk of bias
Using the 11-item checklist recommended by the Cochrane Collaboration Back Review Group,55 two reviewers independently assessed each study for methodological risk of bias and discrepancies were resolved by consensus (see online supplementary appendix 2). These criteria assess study characteristics related to selection bias, performance bias, attrition bias and detection bias. Van Tulder et al56 reported that RCTs meeting fewer than six criteria reported approximately 50% greater effect sizes than those meeting ≥6 criteria, indicating that studies with lower methodological quality may have exaggerated results. Therefore, in this review, articles were classified as having a ‘high risk’ (<6 ‘yes’ responses) or ‘low risk’ of bias (≥6 ‘yes’ responses).
Two reviewers independently rated the level of evidence of the final selected articles according to the Oxford Centre for Evidence Based Medicine.57 This system is a systematic approach to rank strength of evidence according to the type of clinical question involved. Levels of evidence range from 1 to 5 where level 1 studies are regarded to contain the highest quality of evidence. Consensus was obtained between both reviewers for each article's risk of bias and level of evidence rating.
Results
Initial database searches identified 1372 potential articles with 183 articles selected for detailed review (figure 1). Sixteen articles were included in the final review (table 1).
Patient characteristics
Study design
Of the 16 articles,6 ,48 ,49 ,58–70 4 were RCTs.62 ,63 ,67 ,70 The remaining 12 studies were prospective cohort design49 ,58–60 ,64 ,68 or cross-sectional studies.6 ,48 ,61 ,65 ,66 ,69 Four included multivariate analyses to control for variables (such as age, gender, education, height, weight, body mass index and time since surgery) that may have affected their results.49 ,64–66 Six studies were rated as level 249 ,58 ,63–67 ,69 and 10 were rated level 4.6 ,48 ,58–62 ,68 ,70 All studies6 ,48 ,49 ,58–70 were rated as having a high risk of bias (see online supplementary appendix 2).
Patient characteristics
All 16 studies6 ,48 ,49 ,58–70 included both men and women. Women comprised between 3% and 45% of patients within studies. Mean age ranged from 22 to 30 years. Patellar tendon graft was used exclusively for reconstruction in four studies,59 ,60 ,65 ,70 hamstring graft exclusively in four studies6 ,58 ,63 ,67 and both graft types were utilised in six studies.48 ,49 ,62 ,64 ,68 ,69 Two studies did not report graft type.61 ,66
One study excluded patients with any previous history of knee surgery.69 Two studies excluded patients who specifically had a previous history of ACLR6 ,48 and three excluded patients with a history of meniscectomy.62 ,63 ,67 Three studies included patients with ipsilateral partial meniscectomy62 or contralateral ACL reconstruction.66 ,68 Nine studies49 ,58–61 ,64 ,65 ,68 ,70 did not provide information regarding patients’ previous surgical history. Surgical details beyond graft type and fixation, including information regarding meniscectomy or meniscal repair, was stated in one study.6 Concurrent meniscal repair during surgery was permitted in two studies6 ,67 but not in two others.64 ,68
Each study defined athletic status based on patients’ preinjury competition level or Tegner activity level. Competitive athletes were generally defined as anyone participating in non-professional sports leagues locally, regionally or nationally. Recreational athletes were defined as anyone participating in sports who did not meet the definition of a competitive athlete. Ten studies included patients participating in at least recreational sports.6 ,49 ,60–63 ,65 ,66 ,69 ,70 Two studies included only patients participating in competitive sports.58 ,68 Four studies did not report preinjury athletic status.59 ,64 ,66 ,67
Patient follow-up
Patients were tracked for return to sport between 6 months and 7.9 years after ACLR. The most common re-evaluation timeframe was at 1-year postsurgery.49 ,58 ,63–66 ,68 ,69 Other timeframes used were 6 months,68 1–2,61 2–3,62 ,63 ,67 ,70 3–4,48 ,60 56 and 8 years.59
Return to sport outcomes
Return to sport information was obtained using two methods: through patient self-report48 ,58 ,65 ,66 ,68–70 including the Tegner Activity Scale,6 ,49 ,61–64 ,67 and study-defined criteria.59 ,60 In studies where patient self-report was used but not with the Tegner Activity Scale, patients compared their current sports participation frequency65 ,70 and/or competition level48 ,58 ,65 ,66 ,68 ,70 with their preinjury participation level. For study-defined criteria, Arvidsson et al59 grouped patients from I–IV, where group I included patients with ‘no complaints, sports possible as normal’ to group IV which included those with ‘pronounced instability and pain made sports impossible.’ Barrett and Mackenney60 graded activity from I–IV, where grade I included national or county level sports and grade IV included those not participating in any sport. Though patients may not have returned to the same preinjury sports, they classified these patients as having returned to their preinjury level of sports if they rated their current and preinjury activity levels the same at follow-up. At follow-up, an average of 50.7% of patients returned to preinjury level of sports activity.6 ,48 ,58–60 ,62 ,63 ,68–70 Modified sports participation, defined as patients achieving a lesser activity level compared with their preinjury level, was reported in 32.9% of patients and 17.2% of patients did not return to sports at all.6 ,58–60 ,62 ,63 ,66 ,70 Patient reported reasons for not returning to preinjury sports participation included fear of reinjury,6 ,48 ,60 ,62 ,69 ,70 impaired knee function,48 ,70 social/family reasons,6 ,70 instability,6 ,69 pain,62 ,69 no motivation,48 effusion,69 muscle weakness69 and knee extension deficit.62
Variables associated with return to sport
Variables representing knee impairment and function
The evidence reporting the association between knee impairment and function and return to sport is limited. Based on four level 4 studies and one level 2 study, weak evidence54 supports associations between return to sport and higher postoperative quadriceps torque,59 ,69 ,70 less knee effusion60 ,69 and a higher Marx Activity Score.62 Based on two level 2 studies and one level 4 study, weak evidence54 supports associations between return to sport and greater postoperative tibial rotation,67 less pain60 ,69 and fewer episodes of instability.69 Based on one level 2 study and four level 4 studies, weak evidence54 indicates no association between return to sport and preoperative quadriceps torque,64 preoperative anterior knee joint laxity,64 postoperative anterior knee joint laxity,60 ,68 ,69 preoperative knee extension ROM,64 postoperative knee extension or flexion ROM69 or preinjury activity level.64 There is conflicting evidence for associations between return to sport and the IKDC subjective form score,6 ,62 ,69 IKDC Grade,6 ,58 ,62 postoperative hamstring torque,59 ,61 Lysholm Knee Score6 ,61 ,62 and postoperative LSI for single hop or crossover hop for distance.58 ,61 ,68 Available raw data and between-group statistics for each study is presented in table 2.
Variables associated with return to sport
Psychological variables
Studies utilised several standardised measures to assess psychological variables, including the Tampa Scale of Kinesiophobia (fear of movement or reinjury),48 ,65 ,69 Anterior Cruciate Ligament-Return to Sport after Injury Scale (athletic confidence, emotions and risk appraisal),66 ,68 Psychovitality questionnaire (self-motivation to return to sport),62 ,63 Knee Self-Efficacy Scale (evaluates beliefs about the ability to perform tasks),49 Shortened Profile of Mood States (negative affect),65 Pain Catastrophising Scale (evaluates people's thoughts and feelings about pain)65 and Emotional Responses of Athletes to Injury Questionnaire.68
Based on three level 2 and two level 4 studies, weak evidence54 supports associations between return to sport and kinesiophobia48 ,65 ,69 and athletic confidence.66 ,68 Based on one level 2 and one level 4 study, weak evidence54 supports associations between return to sport and preoperative knee self-efficacy49 and preoperative self-motivation.62 ,63 Weak evidence54 exists indicating that emotional response to injury/surgery,68 negative affect and pain catastrophising65 are not associated with return to sport. Available raw data and between-group statistics are presented in table 2.
Discussion
Surgery is commonly recommended for athletes with ACL tears wishing to return to their previous level of sports activity.2 However, many of these athletes never return to their preinjury level of play.3 ,5 This review summarises the literature on knee impairment, function and psychological variables associated with return to sport following ACLR. In this review, we broadly defined return to sport to include all possible definitions (any sport, the same sport and the same level in preinjury sport) and at any postsurgical timeframe. A limited number of articles met our inclusion criteria. Many potentially relevant articles only included self-report of function as the primary outcome and were excluded. Although functional improvement is important, return to sport is often the main reason for patients to elect surgery.2 Based on our review, weak evidence54 exists suggesting that higher postoperative quadriceps strength,59 ,69 ,70 less knee effusion,60 ,69 lower pain,60 ,69 fewer episodes of instability,69 greater tibial rotation ROM,67 lower kinesiophobia,48 ,65 ,69 higher athletic confidence,66 ,68 higher preoperative knee self-efficacy49 and higher preoperative self-motivation62 ,63 are associated with return to sport. Although postsurgical anterior knee joint laxity has been linked with patient satisfaction71 and general knee function72 following ACLR, there was insufficient evidence that anterior knee laxity influences return to sport.60 ,68 ,69
Return to sport criteria following ACLR includes various assessments of knee impairment and function. Recently, Barber-Westin and Noyes10 reported the most commonly cited postsurgical return to play criteria included achieving specific LSI for quadriceps strength and hop testing, full knee ROM and no knee effusion. They also advocated for the inclusion of a drop-jump test, single-leg squat test to 90°, assessment of knee laxity and examination of sports-specific drill performance. Thomee et al9 recommended strength and hop test performance criteria utilising absolute values and between-limb comparisons prior to return to sport, and proposed criteria can be adjusted according to type of sport patients are returning to (eg, cutting/pivoting, recreational/competitive and/or contact/non-contact). Our review supports including assessment of LSI for quadriceps strength and measurement of knee effusion. However, we found conflicting evidence to support the use of hop testing, and insufficient evidence to support using anterior knee joint laxity assessment or knee flexion and extension ROM in return to sports criteria following ACLR. Although functional testing, which traditionally evaluates differences between the surgical and non-surgical limb, is considered important to assess athletes’ neuromuscular control and has been linked to better self-reported knee function,73 only three studies examined the association between hop testing and return to sport.58 ,61 ,68 Although two studies found no association between LSI on the single hop for distance61 ,68 or crossover hop for distance61 ,68 and return to sport, Ardern et al58 noted that an LSI ≥85% on both hop tests significantly increased the likelihood of return to preinjury level of sports participation. Baltaci61 also studied the triple hop for distance and found no association with return to sport. Additional studies investigating the relationship between hop testing and return to sport are needed for more definitive conclusions.
General return to sport criteria does not include assessments of psychological variables, yet evidence exists for their inclusion. Fear of reinjury is a frequently cited reason that patients do not return to preinjury level of sport46 and may relate to some athletes’ confidence in their ability to safely return to sport following surgery. In this review, lower athletic confidence was associated with decreased likelihood of return to sport.66 ,68 Psychological variables such as fear of reinjury48 ,65 ,69 and reduced athletic confidence66 ,68 may explain why some athletes without physical or functional impairments choose not to return to sport.45 Physical and psychological readiness to return to sport following injury do not always coincide,43 so techniques addressing fear and athletic confidence may need to be incorporated during rehabilitation. Patients receiving presurgical education by patients who have completed their post-ACLR rehabilitation, known as ‘modeling,’ demonstrate higher rehabilitation self-efficacy and earlier functional achievements 6 weeks post-ACLR.74 In the postlumbar fusion population, combined psychomotor training to improve movement patterns and address maladaptive psychological behaviours decreases kinesiophobia, improves self-efficacy and decreases functional disability up to 3 years postsurgery.75 The short-term and long-term effectiveness of modeling and psychomotor training on return to sport in the post-ACLR population warrants further attention.
For this review, we broadly defined return to preinjury sport to include the same level of sport, whether or not participation in the actual preinjury sport was achieved, at any timeframe postsurgery. Overall, 50.7% of patients returned to their preinjury level of sports,6 ,48 ,58–60 ,62 ,63 ,68–70 which is lower than previously published reviews.3 ,46 At 2 years postsurgery, two separate reviews reported 63–79% return to preinjury sports participation.3 ,46 In contrast to these reviews, postsurgical follow-up in this review ranged from 1 to 8 years postsurgery, which may have influenced reported rates. Additionally, 10 studies in this review included recreational athletes,6 ,49 ,60–63 ,65 ,66 ,69 ,70 but the athletic participation levels in previous reviews3 ,46 was not described. Athletes participating at higher competitive sports levels have shorter physical recoveries postsurgery76 and professional athletes’ motivation to return to preinjury level of sport is likely higher than non-professional athletes. However, compared with recreational athletes, professional athletes’ drive to return to play may yield greater negative psychological responses following injury and/or surgery, which may also affect return to sport. Future research addressing the influence of the level of athletic participation on return to sports rates is needed.
There are some limitations to this review. First, relevant articles may have been missed. In an attempt to capture all relevant articles, multiple databases were searched with the aid of a reference librarian and no limitation on publication year was applied. Only one exclusion criterion of no concomitant ligamentous surgery or microfracture surgery was used. This did not affect the number of studies examined, as studies including concomitant ligamentous surgery or microfracture surgery had already been eliminated for not meeting the inclusion criteria, including analysis between variables of interest and return to sport or utilising a specific return to sport measure. Second, we restricted our search to articles published in English, which may have limited our results. Resources to translate foreign publications were not available. Additionally, we included articles using the Tegner Activity Scale, which categorises individuals who are playing sport as well as those who are not. By not differentiating between sports and work activities, articles utilising this measure may not accurately report actual return to sport. We chose to include these articles because they made attempts to quantify regular physical activity levels, as opposed to articles which were excluded because they used scales that only identified potential activity levels. Finally, four studies59 ,64 ,66 ,67 did not indicate patients’ preinjury sports participation. It is possible that these patients were not participating in sports before surgery so returning to sport was not a relevant outcome. This may have affected the accuracy of our return to sport analysis.
Many studies provided only level 4 evidence and all studies were rated as having a high risk of bias. Although RCTs are ideal, prospective cohort designs including assessment of the multiple variables thought to be associated with return to sport, such as age, gender and time since surgery, would be appropriate. Fourteen studies had 100 patients or less6 ,48 ,49 ,59–65 ,67–70 and of these, 6 had less than 50 patients.49 ,60 ,61 ,65 ,67 ,70 With relatively small sample sizes, it is possible that the magnitude of the results was overstated. Studies with larger cohorts are needed to clarify these relationships. The type of postoperative rehabilitation, such as accelerated versus conservative, may influence patients’ ability to return to sport. Patients’ postoperative rehabilitation course was reported in varying detail in only 10 studies,6 ,58 ,60 ,63 ,64 ,66–70 making it difficult to critically examine all variables that may be related to patient outcomes. Only four prospective cohort studies accounted for potential confounders to surgical outcomes, such as age, gender, time since surgery and body mass index.49 ,64–66 These studies did not find significantly different results compared with those not statistically adjusting for these confounders, but the strength of associations reported in this review may have been altered if all studies performed these analyses. Although several studies included documentation of anterior knee laxity62 ,63 ,67 ,70 and ROM,60 ,61 ,63 ,68 their association with return to sport was not examined. Four articles examining these relationships found no association between return to sport and laxity60 ,64 ,68 ,69 or ROM64 ,69 but these conclusions may have been altered if the associations were consistently analysed across all studies. Finally, gender-related differences in return to sport may exist but were not explored in any study in this review. Ardern et al58 reported that men were more likely than women to attempt full competition in their preinjury sport 1-year postsurgery and Noojin et al77 reported that men scored higher on the Tegner Activity Scale than women 3 years postsurgery. However, Ferrari et al78 found no gender difference in Tegner scores 4.5 years post-ACLR. These limitations highlight the need for further studies in this area.
The influence of multiple variables representing knee impairment, function and psychological status on return to sport following ACLR has been investigated. Commonly utilised postsurgical return to play criteria include evaluation of knee impairments such as quadriceps strength and effusion that, in this review, were weakly54 associated with return to sport. Evidence was lacking to definitively support associations between return to sport and other variables representing knee impairments and function, such as knee joint laxity and hop testing. The ability of athletes to return to their preinjury level of sport following surgery is likely multifactorial, but currently there is not enough evidence to make strong recommendations about current return to play criteria. Greater attention should be placed on the effectiveness of these objective criteria in accurately identifying when patients can safely return to preinjury activity levels. Additionally, including psychological criteria in return to sports guidelines is likely warranted. Future research should include larger randomised studies that investigate multiple variables representing knee impairment, function and psychological status, their interactions and return to play.
What are the new findings
-
Variables that may be associated with good functional outcome and patient satisfaction following anterior cruciate ligament reconstruction have been examined, but few studies have examined whether these variables are also associated with return to sport.
-
There is weak evidence for some of the existing return to sport criteria following anterior cruciate ligament reconstruction.
-
Weak evidence exists supporting an association between psychological variables and return to sport, suggesting that psychological variables should be considered for inclusion in return to sport criteria.
Acknowledgments
The authors would like to acknowledge Kim Lipsey, MLS, member of the Health Information Resources division at Washington University's Bernard Becker Medical Library, for her assistance with the literature search.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors In detail, SC participated in conception, performed part of the literature search, determination of final articles, analysis and interpretation of data, drafting of the manuscript, and final approval given; BAR and SEK participated in critical revision of the manuscript and given final approval; MH-H participated in determination of final articles, analysis and interpretation of data, critical revision of the manuscript, and given final approval. SC is the guarantor.
-
Funding This work was supported by the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH) and NIH Roadmap for Medical Research Grant Number UL1 RR024992.
-
Competing interests BAR received research funding from the National Institute of Health by K24 NS060825 and UL1 TR000448 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH). MH-H was supported by the National Center for Medical Rehabilitation Research, National Institute of Child Health and Human Development Grant K23 HD067343. All authors had financial support through the NCRR for the statistical analyses only for this manuscript.
-
Provenance and peer review Not commissioned; externally peer reviewed.