Article Text

Abstract
Objective Patellar taping is frequently used to treat patellofemoral pain (PFP). This systematic review and meta-analysis (1) evaluates the efficacy of patellar taping for patients with PFP, (2) compares the efficacy of various taping techniques and (3) identifies potential biomechanical mechanisms of action.
Methods The MEDLINE, CINAHL, SPORTSDiscus, Web of Science and Google Scholar databases were searched in January 2013 for studies evaluating the effects of patellar taping on pain and lower-limb biomechanics in individuals with PFP. Three independent reviewers assessed each paper for inclusion and two assessed for quality. Means and SDs were extracted from each included study to allow effect size calculations.
Results Twenty studies were identified. There is moderate evidence that (1) tailored (customised to the patient to control lateral tilt, glide and spin) and untailored patellar taping provides immediate pain reduction of large and small effect, respectively and (2) tailored patellar taping promotes earlier onset of vastus medialis oblique (VMO) contraction (relative to vastus lateralis contraction). There is limited evidence that (1) tailored patellar taping combined with exercise provides superior pain reduction compared to exercise alone at 4 weeks, (2) untailored patellar taping added to exercise at 3–12 months has no benefit and (3) tailored patellar taping promotes increased internal knee extension moments.
Conclusions Tailoring patellar taping application (ie, to control lateral tilt, glide and spin) to optimise pain reduction is important for efficacy. Evaluation of tailored patellar taping beyond the immediate term is limited and should be a research priority. Possible mechanisms behind patellar taping efficacy include earlier VMO onset and improved knee function capacity (ie, ability to tolerate greater internal knee extension moments).
- Evidence based reviews
- Intervention efficacy
- Knee
- Knee injuries
- Physiotherapy
Statistics from Altmetric.com
Introduction
Patellofemoral pain (PFP) is one of the most common musculoskeletal presentations to orthopaedic,1 ,2 general practice3 and sports medicine clinics. Simple activities of daily living such as squatting and walking down stairs commonly exacerbate PFP, thereby reducing occupational and physical capacity.4 Furthermore, chronic knee pain, which is frequently associated with PFP,5–7 has been linked to osteoarthritis in later life.8
There is a lack of consensus on the source of pain in relation to PFP.9 However, patellar maltracking including increased lateral patellar translation,10–12 tilt10 and spin,11 as well as increased lateral patellofemoral joint (PFJ) stress,13 ,14 may associate with PFP. Owing to its ability to control lateral patellar tracking, vastus medialis oblique (VMO) delay or weakness is considered a key biomechanical risk factor for patellar maltracking.15 Supporting this, delayed VMO onset proved to be a risk factor for PFP development during basic military training.16 Additionally, a systematic review reported that VMO onset occurred after vastus lateralis (VL) in some individuals with PFP compared to controls during a range of functional tasks.17
In addition to impaired VMO muscle function, a number of other proximal, distal and local biomechanical factors may contribute to the aetiology of PFP.9 As a result, numerous conservative interventions such as orthoses, taping and exercise are commonly used in rehabilitation. A recent systematic review identified multimodal physiotherapy as the gold standard approach, and foot orthoses and acupuncture should also be considered.18 Multimodal physiotherapy combines a number of interventions including stretching, deep friction tissue massage, strengthening exercises, education and patellar taping. To tailor and improve the efficiency of this proven multimodal approach, the value, mechanisms behind efficacy and the most effective method of application for each multimodal component need to be understood.
Patellar taping forms a core component of evidence-based multimodal programmes.19 ,20 Many taping protocols exist, with the most widely used ones being the tailored McConnell taping technique.21 Adhesive, rigid taping is applied to the knee to reduce lateral glide, tilt and rotation of the patella according to assessment findings (see figure 1), with the primary goal being to reduce pain by at least 50% during relevant functional activity.21 Additional taping methods used clinically and evaluated in the literature include untailored medially directed taping,22 inferiorly directed taping23 and Kinesio Taping aimed at enhancing vastii muscle activation and synergy.24
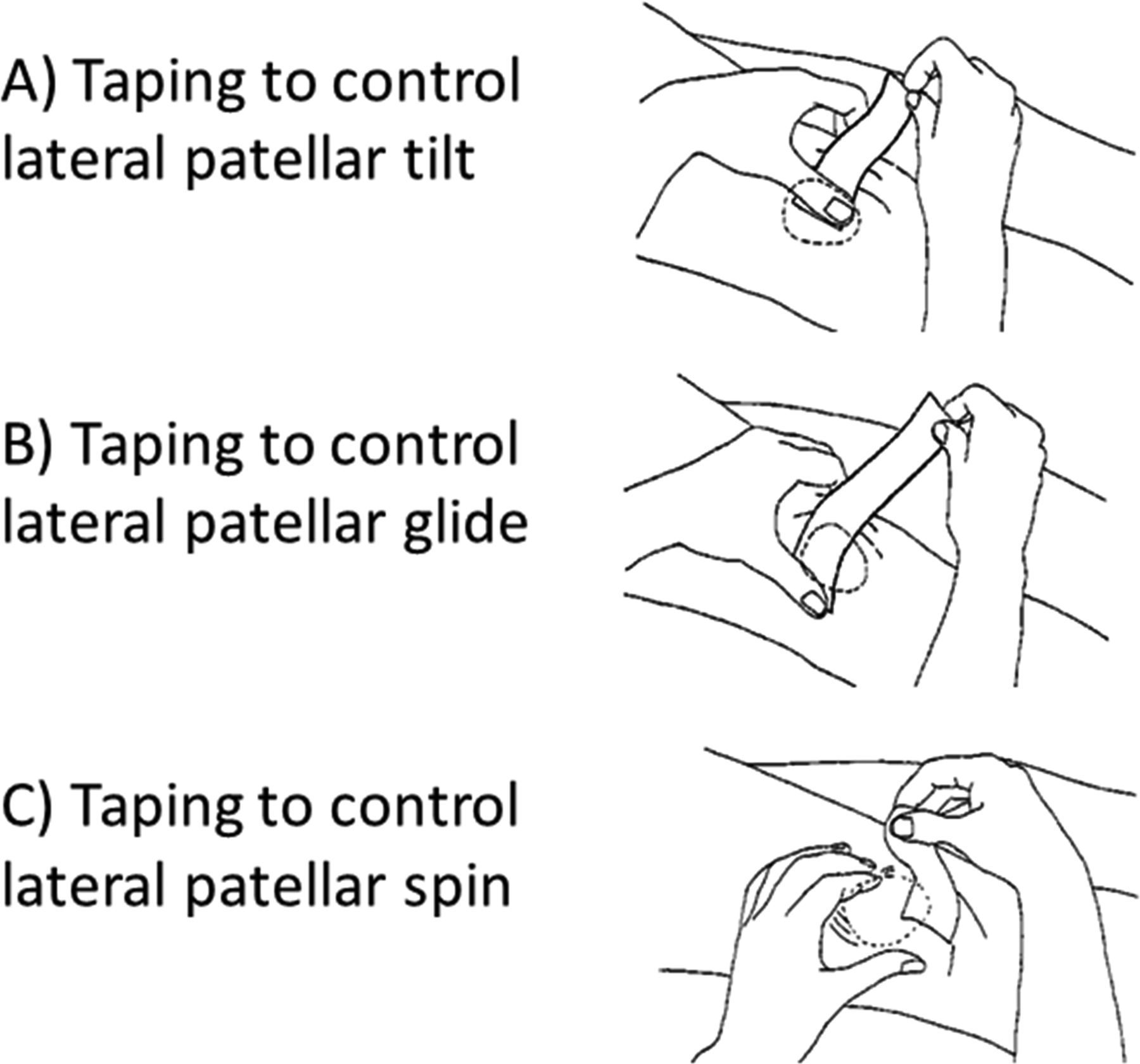
Components of McConnell's tailored patellar taping.
Previous systematic reviews evaluating patellar taping in PFP18 ,25–28 have reported mixed results; in 2014, those reviews will have at least four limitations. First, three of those reviews are now dated25 ,27 ,28 and therefore do not benefit from important recent trials concerning clinical outcomes and biomechanical mechanisms. Second, two of the reviews did not specifically evaluate patellar taping effects in PFP (ie, they considered a broad range of treatments together) or did not focus on PFP.18 ,25 Third, none of the previous reviews18 ,25–28 evaluated the biomechanical effects of patellar taping to better understand potential mechanisms for effectiveness. Finally, the Cochrane review26 of patellar taping trials up to mid-2011 used very stringent inclusion criteria in relation to methodological quality and thus included just five randomised controlled trials. Although stringency is laudable, the review concluded that there was ‘insufficient evidence’ regarding efficacy and the underlying mechanisms were ‘unclear.’ Importantly, trials of patellar taping cannot score the maximum Cochrane ‘quality’ scores because it is difficult to blind patients, and it is not possible to blind the treating practitioner. Our systematic review and meta-analysis was designed to ‘loosen’ the Cochrane inclusion criteria slightly while still using clear a priori principles taking into account risk of bias in lower quality studies when determining levels of evidence. The aims included (1) evaluation of the efficacy of patellar taping for patients with PFP, (2) comparison of the efficacy of various taping techniques and (3) identification of the potential biomechanical mechanisms of action.
Methods
The PRISMA statement was consulted prior to the start of this review and the checklist completed.29
Search strategy
The MEDLINE, CINAHL, SPORTSDiscus and Web of Science databases were searched in January 2013. Reference lists of included studies were screened, and citation tracking (ie, identifying studies which have cited included references) in Google Scholar was completed to identify any additional studies. Key words searched and search results are shown in online supplementary appendix table 1. MeSH headings were not used to narrow or broaden the search.
Inclusion and exclusion criteria
Studies evaluating the effects of patellar taping on pain and lower-limb biomechanics in adults with PFP were included. The inclusion criteria required participants to be described as experiencing retropatellar, peripatellar or PFP. Other terms or synonyms associated with PFP (anterior knee pain, chondromalacia patellae) were also included. Patellar taping included tailored, medially directed or any other suitably described protocol. If other interventions were combined with taping, the study was only included if the effects of taping could be clearly extracted (eg, taping and exercise compared to exercise alone).
Studies or data evaluating the effects of patellar taping on pain beyond the immediate term, which did not contain a control or comparison group, were excluded. Unpublished studies, case-series studies, non-peer reviewed publications, studies not involving humans, reviews, letters, opinion articles, non-English articles and abstracts were excluded. Studies including participants with other knee conditions such as patellar tendinopathy, osteoarthritis, internal derangement, knee ligament insufficiency or previous knee surgery were excluded. Outcome measures of interest included (1) symptom reduction (pain) and (2) lower-limb biomechanics (muscle activity, kinematics and kinetics).
Review process
All retrieved studies were downloaded to Endnote Web, V.X4 (Thomson Reuters Philadelphia, Pennsylvania). Results were cross-referenced and duplicate studies were deleted. Relevant titles were highlighted, with abstracts and full texts reviewed independently for inclusion by three authors (CB, VB and SL).
Quality assessment of studies
The appropriateness of each study's PFP diagnostic criteria was evaluated by two independent reviewers (CB and VB) using a previously established inclusion/exclusion criteria checklist.30 Additionally, the internal validity of each study was evaluated by two independent reviewers (CB and VB) using the PEDro scale.31 Any discrepancies between the two reviewers on either the inclusion/exclusion criteria checklist or the PEDro scale were resolved through a consensus meeting, with a third reviewer (DM) available if necessary. Following the application of the PEDro scale, studies with a score of ≥6/10 were considered to be of high quality (HQ), and those <6/10 as low quality (LQ). To evaluate the impact of the less stringent inclusion criteria used in this review, a sensitivity analysis was completed, where studies of quality assessment scores on the PEDro scale of less than 7 (ie, all non-randomised trials) were excluded.
Data extraction
To assist with interpretation of findings, information including study design, population (number of PFP participants, mean age), intervention, control intervention/comparisons, taping protocol and results was extracted from each included study. Means and standard deviations (SDs) for all baseline and follow-up data were extracted to calculate effect sizes (ESs; Cohen's d) using Cochrane Review Manager (V.5). Interpretation of ES magnitude was based on those used by Hume et al32 where ESs were considered small (<0.6), medium (0.6–1.19) and large (>1.2). Where means and SDs were not available in the publication, we emailed corresponding authors to seek additional data. For ease of visual interpretation, ES calculations including 95% CI were presented in forest plots produced by the same Cochrane Review Manager software. Where homogeneity between studies was adequate (ie, similar taping methods and outcome measures), we pooled those data. The level of statistical heterogeneity for pooled data was established using the χ2 and I2 statistics (heterogeneity defined as p<0.05).
The strength of evidence supporting each outcome for the various taping methods was determined by the number and quality of studies supporting that finding using predetermined criteria similar to that proposed by van Tulder et al33:
-
Strong evidence was based on results derived from multiple studies, including a minimum of two HQ studies which are statistically homogeneous (p>0.05).
-
Moderate evidence was based on results derived from multiple studies, including at least two HQ studies which are statistically heterogeneous (p<0.05), or from multiple LQ studies which are statistically homogeneous (p>0.05).
-
Limited evidence included results from multiple LQ studies which are statistically heterogeneous (p<0.05) or from one HQ study.
-
Very limited evidence was based on results from one LQ study.
-
Conflicting evidence included insignificant pooled results derived from multiple studies, of which some show statistical significance individually, regardless of quality which is statistically heterogeneous (p<0.05).
Data were extracted relating to the following questions:
-
Was patellar taping or the addition of patellar taping effective at reducing pain in the longer term (ie, beyond immediate effects)?
-
Could patellar taping provide immediate pain reduction?
-
How did patellar taping alter lower-limb biomechanics?
Results
Search results
The initial search produced 228 citations. Following the application of the selection criteria to titles and abstracts, this was reduced to 28, and after viewing full texts the final number was 20 (see figure 2). The primary reasons for exclusion included lack of a control group for long-term follow-up, evaluation of asymptomatic participants and evaluation of non-functional activities (eg, static quadriceps contraction in non-weight-bearing). Results of the diagnostic checklist and the PEDro scale are shown in online supplementary appendix tables 2 and 3, respectively. Supplementary online appendix table 4 summarises the main methodological details and results for the included studies. Ten studies21 ,34–42 specified using a tailored taping protocol (ie, taping tailored based on lateral tilt, glide and spin evaluation), with others describing an untailored medially directed,22 ,43–45 Kinesio Tape24 ,46 or infrapatellar23 taping protocol. Additional data were obtained from Cowan et al,34 Gilleard et al35 and Keet et al.22

Flow diagram of search results.
Effects of patellar taping on pain in PFP
The effects of patellar taping on pain are summarised in figure 3. Owing to the heterogeneity of interventions compared, data pooling was inappropriate for taping effects beyond the immediate term.
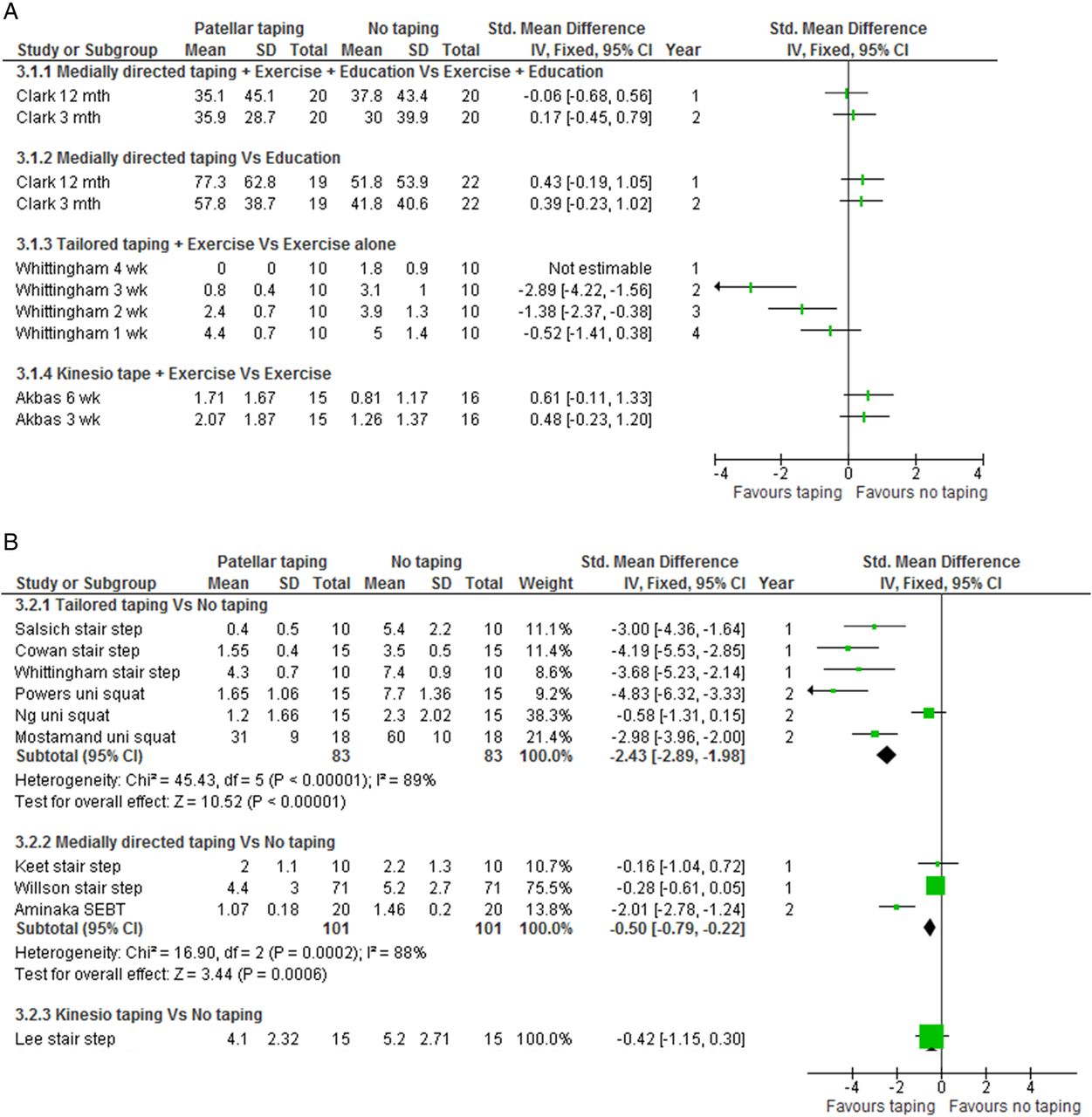
Effects of patellar taping on pain, (A) beyond the immediate term, (B) in the immediate term.
Effects of patellar taping on pain in PFP beyond the immediate term
Limited evidence (1 HQ study) indicates that adding medially directed taping to exercise and education compared to exercise and education alone, and that adding medially directed taping to education compared to education alone do not improve pain at 3 or 12 months (figure 3A).37 Limited evidence (1 HQ study) indicates greater pain reduction following the addition of tailored patellar taping to exercise at 4 (ES not estimable), 3 (ES, 95% CI −2.89, −4.22 to −1.56) and 2 weeks (ES, 95% CI −1.38, −2.37 to −0.38), but not 1 week.42 Very limited evidence (1 LQ study) indicates that adding Kinesio Taping to exercise does not improve pain at 3 or 6 weeks.46
Immediate effects of patellar taping on pain in PFP
Six studies evaluated the immediate effects of tailored patellar taping; three studies evaluated the immediate effects of untailored medially directed taping and one study evaluated the immediate effects of Kinesio Tape (see figure 3B). Moderate evidence (6 HQ studies21 ,39 ,41 ,42 ,44 ,47) indicates that tailored patellar taping provides immediate pain relief of large effect during a range of functional tasks (I2=89%, p<0.00001; ES, 95% CI −2.43, −2.89 to −1.98). Additionally, moderate evidence (3 HQ studies22 ,38 ,48) indicates that untailored medially directed taping produces immediate pain relief of small effect during functional tasks (I2=88%, p=0.0002; ES, 95% CI −0.50, −0.79 to −0.22). Very limited evidence (1 LQ study) indicates that Kinesio Taping has no immediate effect on pain.24
Effects of patellar taping on muscle activity in PFP
Moderate evidence (3 HQ studies21 ,36 ,47 and 1 LQ study35) indicates earlier VMO onset timing of large effect following tailored patellar taping during a range of functional tasks (see figure 4A; I2=77%, p=0.0005; ES, 95% CI −1.31, −1.67 to −0.95). Moderate evidence (3 HQ studies36 ,44 ,47) indicates no change in the VMO:VL ratio following tailored patellar taping during functional tasks (I2=0%, p=0.54; ES, 95% CI −0.15, −0.63 to 0.33).19 ,35 Limited evidence (1 HQ study22) indicates that the VMO:VL ratio is significantly lower following untailored medially directed taping with medium effect during stair-stepping tasks (see figure 4B; ES, 95% CI −0.98, −1.92 to −0.04). Limited evidence (1 HQ study36) indicates no difference in VMO amplitude following tailored patellar taping during a knee perturbation test (see figure 4C). Limited evidence (1 HQ study22) indicates no change in VMO amplitude following untailored medially directed taping during stair negotiation. Very limited evidence (1 LQ study24) indicates reduced VMO amplitude following Kinesio Taping during stair negotiation (see figure 4C; ES, 95%CI −1.24, −1.81 to −0.67).
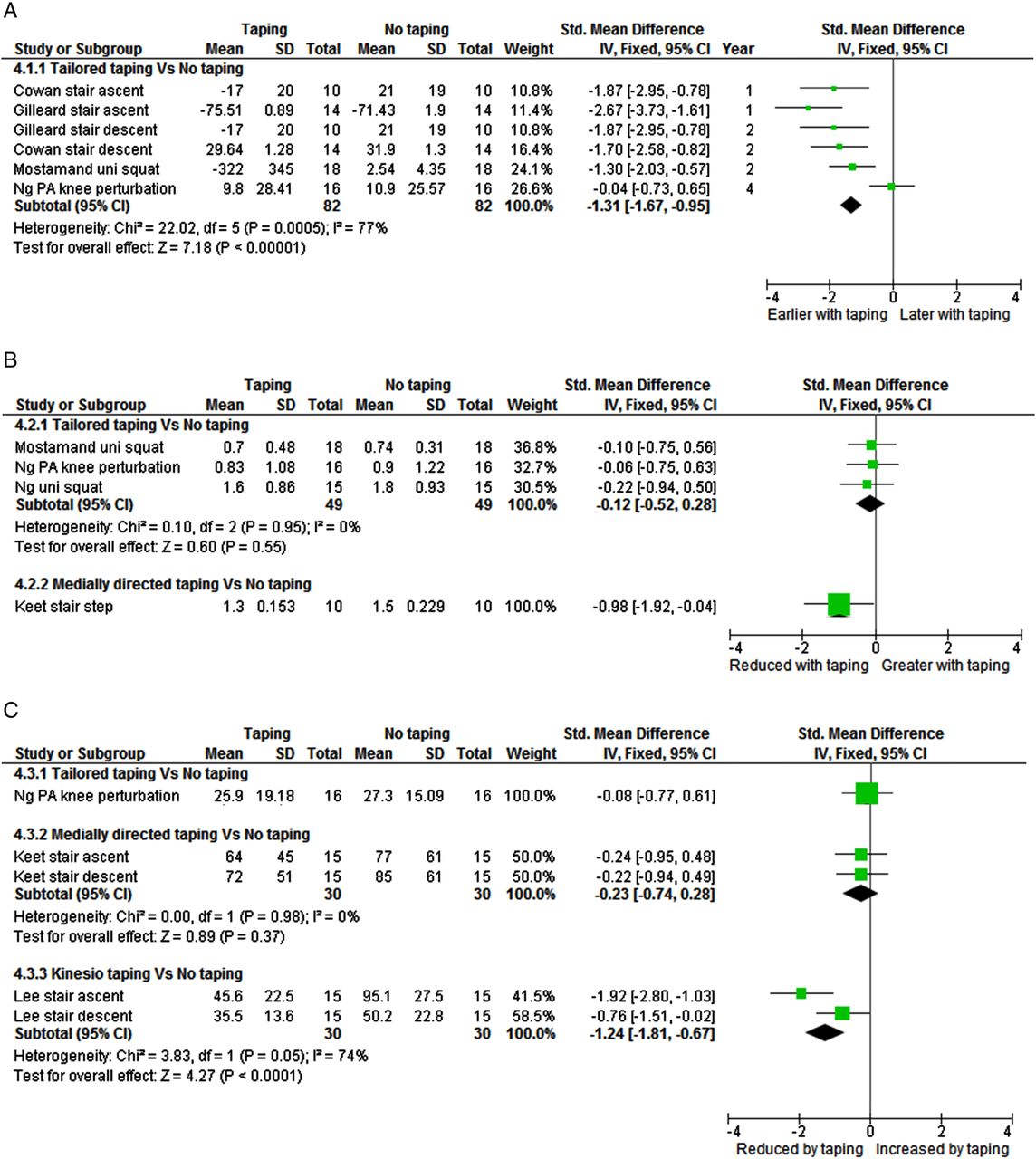
Effects of patellar taping on quadriceps muscle activity, (A) vastus medialis oblique onset, (B) vastus medialis oblique—vastus lateralis ratio, (C) vastus medialis oblique amplitude.
Effects of patellar taping on kinetics and kinematics
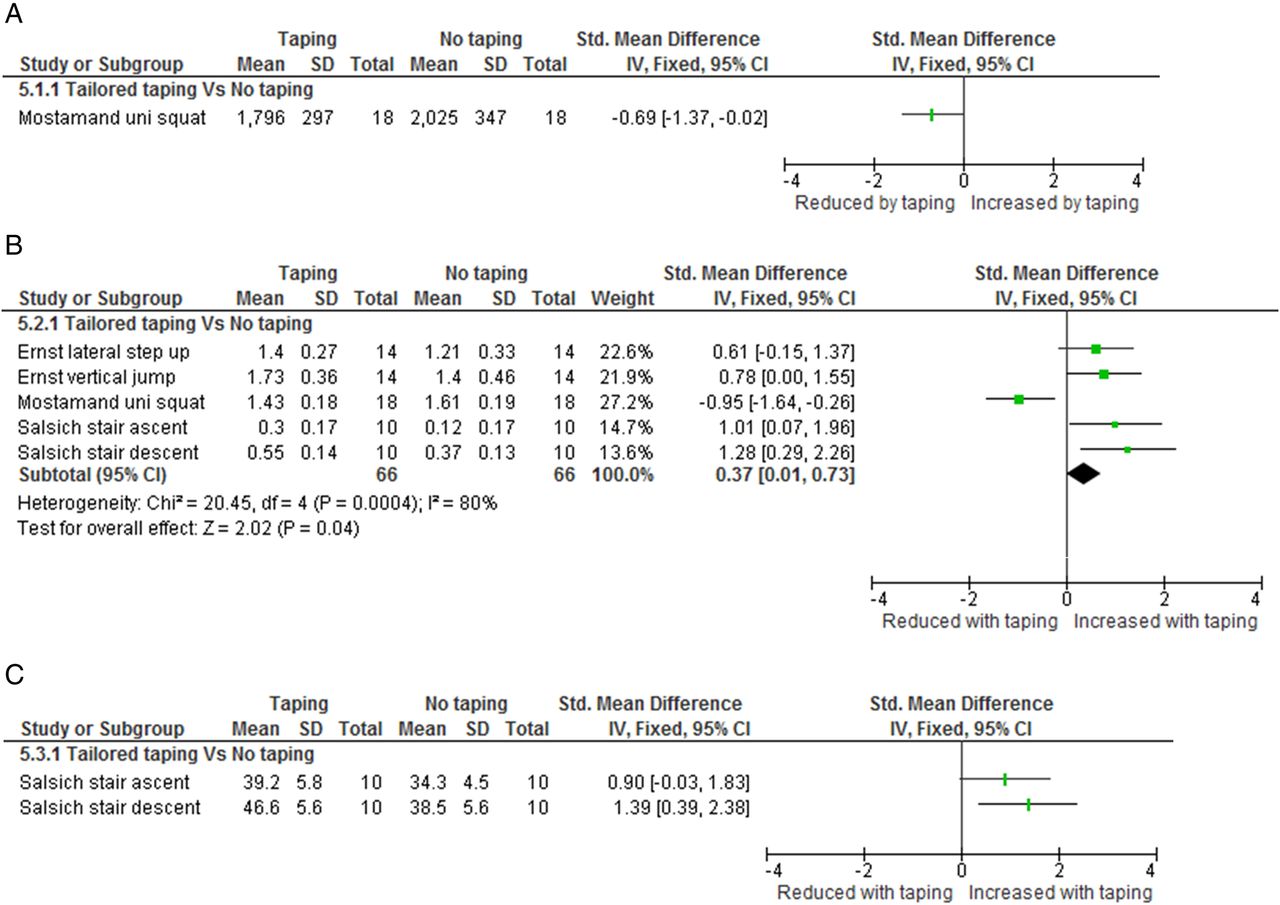
Limited evidence (1 HQ study49) indicates a significant reduction in PFJ reaction force following tailored patellar taping during a unilateral squat task (see figure 5A; ES, 95% CI −0.69, −1.37 to −0.02). Moderate evidence from three HQ studies39 ,40 ,49 indicates increased knee extension moments of small effect following patellar taping during functional activities (see figure 5B; I2=80%, p=0.0004; ES, 95% CI 0.37, 0.01 to 0.73). Limited evidence (1 HQ study39) indicates greater knee flexion following tailored patellar taping during stair ascent and descent (see figure 5C; ES, 95% CI 1.13, 0.45 to 1.81).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of patellar taping on kinetics and kinematics, (A) patellofemoral joint reaction force, (B) internal knee extension moment, (C) peak knee flexion.
Sensitivity analysis
Results of the sensitivity analysis (ie, excluding studies with quality scores of less than 7) indicated similar findings in relation to pain for tailored and untailored medially directed patellar taping (see in web appendix table 5). However, all findings related to the effect of Kinesio Taping on pain were omitted. Additionally, a number of findings related to the biomechanical effects of patellar taping were also omitted, including the effects of tailored patellar taping on PFJ reaction force and peak knee flexion, and the effects of Kinesio Tape on VMO amplitude.
Discussion
This systematic review and meta-analysis provides a clinically relevant summary of the effects of patellar taping on pain and its potential biomechanical mechanisms for efficacy in individuals with PFP. Our systematic review extends the 2012 Cochrane review26 by including data from several studies excluded by the Cochrane randomisation to treatment criterion, adding novel insights into the immediate effects of patellar taping on pain and the biomechanical effects of patellar taping. The sensitivity analysis shows that our conclusions related to changes in pain following tailored and untailored medially directed patellar taping are robust despite using less stringent criteria (ie, inclusion of non-randomised trials). Specifically, similar findings are indicated when more stringent inclusion criteria similar to the previous Cochrane review26 are applied. Additionally, the less stringent criteria allowed the inclusion of greater information related to the effects of Kinesio Taping on pain and patellar taping on potential biomechanical mechanisms.
Twenty studies of varying quality met the inclusion criteria and provided clear guidance for clinicians. Moderate evidence indicates that tailored patellar taping provides immediate pain reduction of large effect during a range of functional activities. Importantly, the individual tailoring of the patellar taping (ie, attempting to control lateral tilt, glide and spin—see figure 1; and ensuring optimal pain reduction) appears to provide more pain relief than simple untailored medially directed taping. Furthermore, there is moderate evidence that VMO onset is earlier and internal knee extensor moments are greater following patellar taping during a range of functional tasks. This provides a plausible biomechanical mechanism for taping efficacy. Importantly, the review highlights a paucity of research investigating longer term effects of tailored patellar taping on pain and function in individuals with PFP. However, clinicians can confidently include taping in management of patients with PFP to obtain/provide short-term pain relief and improved function.
Internal and external validity
Five studies (21%)21 ,22 ,24 ,34 ,38 scored full points for the diagnostic checklist (web appendix table 2). The majority of studies were consistent in their inclusion criteria for PFP participants; however, a number of studies did not state that they excluded possible internal derangement,23 ,35 ,36 ,40 ,43 ,44 ligamentous instability23 ,35 ,36 ,43 ,44 or other sources of anterior knee pain.35 ,36 ,40 ,42–44 These omissions reflect an assumption that PFP is easy to diagnose, which may be defensible, but ensuring that diagnosis is as accurate as possible would be advisable in future studies to avoid confounding pathology. Scores from the PEDro scale were variable and ranged between two and eight. The majority of studies provided adequate eligibility criteria, matching of participant groups, measures of key outcome variables and outcome statistics. However, only four studies blinded participants,23 ,36 ,40 ,48 and only four studies blinded assessors.23 ,34 ,37 ,42 Therapist blinding did not occur in any of the studies; however, this is difficult to achieve in taping studies as effective patellar taping requires therapist skill, knowledge and instruction. Considering that therapeutic effects have been reported to be overestimated by up to 17% with the absence of participant and therapist blinding,50 we recommend that researchers consider and address these potential sources of bias where possible. Additionally, the effect estimates of patellar taping related to pain where participants were not blinded and/or where conditions were not randomised in the current meta-analysis may be overstated. However, these issues may be less important for biomechanical variables such as VMO onset than, for example, pain reports.
Effect of patellar taping on pain in PFP
Patellar taping is commonly used as part of the evidence-based multimodal physiotherapy programmes for the management of PFP.19 ,20 However, only three included studies37 ,42 ,46 evaluated the effects of patellar taping on pain beyond the immediate term (see figure 3). One of these studies evaluated Kinesio Tape designed to facilitate vasti muscle activity,46 and this method of taping provided no additional benefits to exercise prescription over a 6-week period. Findings from the two studies evaluating more traditional patellar taping methods37 ,42 show that it may be an effective adjunct to exercise over a 4-week period42 but not at 3 or 12 months37 (see figure 3A). Although this indicates that the positive effects of patellar taping may dissipate over time, methodological elements must be considered. Importantly, taping approaches between the two studies vary. Specifically, Whittingham et al,42 whose findings show beneficial effects of combining taping with exercise over 4 weeks, tailored patellar taping based on medial/lateral glide, medial/lateral tilt and rotation of the patellar (see figure 1) to achieve a significant (≥50%) reduction in perceived pain following taping. However, Clark et al's37 taping method only included a medial patellar glide in an attempt to reduce pain, without assessment of patellar position, or minimum goal for pain reduction. These differing results highlight the potential importance of tailoring the taping application for each patient.
Further support for individual assessment is provided by considering the immediate effects of taping. Tailored patellar taping reduces pain substantially, while untailored medially directed taping has only small effects on pain (see figure 3B). Immediate and substantial pain reduction may help reduce muscle inhibition associated with PFP51 ,52 and thus improve the patient’s ‘envelope of function’,53 ability to participate in rehabilitation exercise and ultimately hasten and optimise recovery. It is possible that adhering to the tailored patellar taping protocol21 may reduce pain substantially in the longer term (ie, beyond the 4 weeks evaluated by Whittingham et al42). HQ randomised controlled trials are needed to explore this specific question.
Effect of patellar taping on patellar biomechanics
Patellar taping is proposed to reduce pain in individuals with PFP by altering faulty PFJ kinematics during functional activities, and thus reduce PFJ stress. As we did not identify any studies evaluating the effects of taping on PFJ kinematics during weight-bearing functional tasks, this hypothesis cannot be confirmed or refuted. However, one HQ study provided limited evidence that patellar taping reduced PFJ reaction force during a unilateral squat, standardised to 30° knee flexion. The authors hypothesised that reduced PFJ reaction force may be due to an inferior displacement of the patellar and thus greater engagement within the trochlear.49 These mechanical changes may increase the contact area and reduce stress in the PFJ, factors which have been linked to PFP.13 ,14 Supporting this hypothesis, a recent non-weight-bearing MRI study reported inferior patellar translation following patellar taping.54 Further studies evaluating the effects of patellar taping on PFJ kinematics during weight-bearing tasks are needed to clarify the clear mechanisms of clinical effect and potentially improve taping protocols.
The VMO muscle is the primary medial stabiliser of the patella, with its optimal function thought to prevent lateral patellar tracking and subsequent increases to PFJ stress.15 Supporting this, delayed VMO activity was recently reported as a risk factor for the development of PFP,16 and reversal of VMO onset delays during functional movement has been reported to be associated with a successful 6-week course of physiotherapy.55 Our review indicates that one of the mechanisms behind the efficacy of patellar taping for PFP may be earlier VMO onset. In three studies21 ,35 ,47 investigating individuals with PFP and delayed VMO onset relative to pain-free controls, taping led to earlier VMO onset and pain reduction. Taken together, these findings highlight the potential significance of altered VMO timing as a mechanism of patellar taping efficacy. How earlier VMO onset affects PFJ kinematics and stress is unclear and requires further investigation.
Limited evidence22 indicated that the VMO:VL ratio was significantly less (ie, reduced VMO activity relative to VL) following medially directed patellar taping in PFP participants performing stair-stepping tasks. However, the significance of this finding is unclear as pain was not reduced.22 Similarly, Kinesio Taping reduced VMO amplitude during stair negotiation,24 but ES calculations indicated no concurrent reduction in pain (see figure 3B). Additionally, there is limited evidence that the VMO:VL ratio and VMO amplitude are unchanged following the taping method most effective at reducing pain—tailored patellar taping.22 ,36 ,44 These findings may demonstrate that the activation pattern of the vasti is more important than the level of activity when attempting to identify the mechanism of action behind patellar taping efficacy.
The internal knee extensor moment39 ,40 (see figure 5B) and knee flexion angle during stair negotiation39 were found to increase following patellar taping (see figure 5C). These biomechanical changes are most likely related to the increased cadence also observed.39 Interestingly, Mostamand et al49 actually showed reduced internal knee extensor moments during a unilateral squat following taping. Importantly here, however, unlike in other studies evaluating knee extensor moments,39 ,40 Mostamand et al49 controlled the knee function, limiting the squatting depth to 30°. Put together, these findings indicate that patellar taping may effectively reduce knee loading during controlled tasks and increase knee function during uncontrolled tasks. This improved functional capacity is likely to hasten exercise progression and recovery, thereby improving the physiotherapy outcomes and the patient’s occupational capacity. Further research is needed to explore this possibility.
Although we reviewed the potential biomechanical mechanisms for the efficacy of patellar taping in PFP, proprioceptive and other neural mechanisms may also contribute to reductions in pain following taping. For example, asymptomatic individuals demonstrated altered cortical activity on functional MRI following tape application without a directional bias.56 However, tailored taping and exercise produced significantly better outcomes compared to neutral (placebo) taping and exercise.42 Additionally, results from studies evaluating the immediate effects of sham (neutral) taping reviewed in this paper indicate minimal or non-significant changes in pain,22 ,34 muscle activity21 ,34 ,36 and kinematics.40 Therefore, it would seem unlikely that low-level sensory input would be sufficient to generate functional change without a substantial simultaneous mechanical effect. Given that recurrent and/or persistent pain is a potent modulator of cortical activity in many situations, further research combining cortical activity measures and taping in pain populations is warranted to explore the possible proprioceptive taping effects. Finally, taping may have an effect on spinal level excitation via afferent mediation of anterior horn cells supplying the quadriceps, either by a mechanical effect on muscle spindles and golgi tendon organs, or via cutaneous input.57
Limitations and caveats when interpreting this review
Studies in this review used varying methods, specifically with regard to inclusion/exclusion criteria, taping and functional activities evaluated. Therefore, caution must be exercised when considering results from the data pooling completed. Nevertheless, pooling in this meta-analysis improves the power of smaller studies and further synthesises available evidence. Additionally, when identifying ‘levels of evidence’ for each comparison, statistical heterogeneity has been considered, with lower levels of evidence allocated where heterogeneity exists. Owing to a lack of funding and service to facilitate translation, non-English studies were not included in this review.
Although the meta-analysis indicates that tailored patellar taping may have a greater effect on pain than medially directed patellar taping, no study has yet directly compared the two taping approaches. Addressing this should be a priority in future research. Only one study has evaluated the longer term effects of patellar taping in individuals with PFP,37 with many opting for a same-day crossover design. Considering that PFP is often characterised by chronic and recurring knee pain,5–7 long-term studies evaluating the efficacy of patellar taping as an adjunct or alternative to other pain relieving interventions such as foot orthoses and acupuncture18 should be a research priority. The other important consideration related to longer term follow-up in patellar taping studies is the frequency with which patellar taping is applied. Clark et al37 only applied taping during the six treatment sessions over 3 months, yet followed participants for 12 months. This approach may not reflect clinical practice, where tape may be applied more frequently during the initial stages of a rehabilitation programme to enhance function, and is also used in the longer term intermittently to treat flare-ups or during periods of increased activity (sports matches or events). These factors should be considered in the design of any future trials.
Currently, limited evidence indicates that PFJ reaction force is reduced by patellar taping.49 Considering that PFJ reaction force may be linked to the efficacy of patellar taping, further HQ studies are required to confirm these findings in the immediate and longer term. Additionally, the effects of patellar taping on PFJ kinematics, contact area and stress during weight-bearing activities need to be evaluated. This will allow a greater understanding of its potential mechanisms of action, which in turn may improve application methods. Considering that PFP is a multifactorial condition, with variability in the response to interventions such as patellar taping, identification of subgroups of people with PFP who respond to patellar taping may also further optimise patient care.
In summary, our analysis provides moderate evidence for clinicians to include tailored patellar taping in management of PFP, knowing that in the immediate term it will most likely have a large effect on reducing pain and improving functional capacity during accompanying rehabilitation exercises. Tailoring should correct for lateral tilt, translation and spin, as well as modification to ensure optimal pain reduction. Additionally, patellar taping appears to be an effective adjunct to exercise over a 4-week period, although further HQ research is needed to confirm this. Long-term follow-up studies of the efficacy of tailored patellar taping are lacking, and this should be a research priority given the economic and societal burden of patellofemoral pain.
What are the new findings?
-
Tailored patellar taping immediately reduces pain with a large effect, while other techniques have only small (untailored medial patellar taping) or negligible (Kinesio Tape) effects on pain in the immediate term.
-
Tailored patellar taping should be applied to control lateral patellar tilt, translation and spin, with the goal of providing at least 50% pain reduction.
-
Tailored patellar taping is an effective adjunct to exercise over 4 weeks.
-
The mechanism of patellar taping effectiveness appears to be facilitation of earlier vastus medialis oblique onset and enhanced knee function capacity during functional tasks.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix-table 1
- Data supplement 2 - Online appendix-table 2
- Data supplement 3 - Online appendix-table 3
- Data supplement 4 - Online appendix-table 4
- Data supplement 5 - Online appendix-table 5
Footnotes
-
Contributors Each author contributed to developing the research question. CB, VB and SL led on the data collection and analysis, while all authors contributed to the interpretation of data, manuscript preparation and approval for publication. All authors approved the final version for publication.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com