Article Text

Abstract
Aims To prospectively follow a cohort of elite young male professional soccer players with sequential symptom questionnaires and imaging of the anterior pelvis to determine the prevalence and severity of imaging findings.
Methods 34 male athletes (mean age 16.5 years) underwent clinical examination, history/symptom questionnaire, ultrasound and 1.5 T MRI of the anterior pelvis. Athletes then underwent annual questionnaire and ultrasound with MRI also performed every 18 months. Two experienced radiologists scored ultrasound (consensus) and MRI (independently) for abnormality including pubic bone, capsule and tendon oedema and scores correlated with symptoms and presence or absence of previous injuries.
Results Over 4 years the participants fell from 34 to 22 in number with no withdrawals due to groin injury. On study entry no athletes had undergone previous hip or pelvic surgery. On MRI pubic bone oedema, secondary cleft, capsule/tendon oedema and enhancement did not differ substantively between players with and without history of previous injury. κ Analysis for MRI scoring showed excellent agreement (0.84–0.96) for pubic bone marrow oedema, secondary cleft, capsule/tendon oedema and enhancement. On ultrasound inguinal wall motion and adductor tendinopathy did not differ substantively between players with and without history of previous injury. Stability of imaging assessments over time showed no consistent difference.
Conclusions Pubic bone marrow and parasymphyseal findings (cleft, capsule/tendon oedema) on MRI or inguinal canal ballooning on ultrasound were frequently found in asymptomatic athletes and did not predict injury or symptom development.
- Groin Injuries
- MRI
- Soccer
- Ultrasound
- Athletics
Statistics from Altmetric.com
Introduction
Athletic groin pain is a clinical and diagnostic challenge.1–4
Athletic groin pain probably relates to an overuse syndrome involving the symphysis pubis and the converging tendons and aponeuroses of the abdominal, inguinal and adductor compartments.5 All of these structures have been suggested as potential sites of failure in groin pain in athletes, and since, it is also believed that multiple structures are commonly affected, clinical sensitivity is further decreased.2 ,4 Some authors believe inguinal aponeurotic injury initiates the process leading to symphyseal, rectus abdominis and adductor change developing later while others believe the process occurs in reverse.5–7
Radiologically, a spectrum of findings are described for symptomatic athletes involving the inguinal canal, symphyseal bone marrow, entheses and tendons.6–14 The most reproducible MRI findings described are pubic bone marrow oedema (diffuse or linear subcortical) and capsule/tendon oedema or disruption. Ultrasound evaluation has also been described in symptomatic athletes for detecting inguinal hernias, inguinal canal ‘ballooning’ or adductor tendinopathy.10 ,12 ,15 Already some studies have described MRI findings in asymptomatic athletes.16 ,17
We prospectively studied a cohort of young male elite professional soccer players with sequential symptom questionnaires, ultrasound and MRI of the anterior pelvis to determine the prevalence and severity of previously described imaging abnormalities.
Subjects and methods
Institutional ethics approval was granted and all participants gave informed consent. Over a 4-year period (2004–2010), 36 male athletes were recruited from four elite professional soccer academies (mean age at entry16 years 7 months, range 16 years 4 months to 18 years 1 month). Players were not excluded if they had previous or current groin symptoms.
Examination, history and symptom questionnaire
On entry to the study each athlete underwent clinical examination by a single examiner (author 4 with over 20 years experience) blinded to the clinical details. The examination protocol (see online supplementary appendix 1) included pubic tubercle palpation (present or absent)18 any loss on hip rotation was measured using a goniometer and hip adduction strength was assessed manually with the player supine with knee both flexed and extended. Hip examination findings were recorded as normal, or abnormal if hip internal rotation <40° and manually detected weakness or pain with testing of hip abduction or thigh adduction. Thus range of motion, tenderness, weakness and pain during testing were recorded as dichotomous variables. The players also completed a history and symptom questionnaire (see online supplementary appendix 1) and underwent a standardised ultrasound and MRI evaluation of the anterior pelvis. Subsequently athletes underwent annual questionnaire and ultrasound evaluation with additional MRI and questionnaires performed every 18 months.
Ultrasound evaluation
All ultrasound examinations (13–17 MHz transducer, Antares, Siemens Healthcare, Erlanghan, Germany) were performed together by two of three experienced musculoskeletal radiologists (authors 1, 2 and 5 experience 14–19 years) blinded to the questionnaire and MRI results with agreement by consensus.
Ultrasound evaluation included examination of the anterior hip joint, anterior hip muscles and tendons (iliopsoas and quadriceps group), lower abdominal muscles, inguinal canal, symphysis pubis and adductor group muscles and tendons.
The hip was scored for the absence or presence of effusion, osteophytes and labral abnormality (irregularity and/or cyst). Muscles were scored for the absence or presence of acute oedema, tear and/or scarring. Tendons were scored for the presence or absence of tear and graded for tendinopathy using a four-point scale (0—normal, 1—mild, 2—moderate, 3—severe). Tendinopathy was defined as thickening, loss of fibrillar structure and hypoechoic signal change. The symphysis pubis was scored for the absence or presence of effusion and cortical bony irregularity. The inguinal region was scored for the absence or presence of hernia (direct, indirect or femoral), inguinal ligament or aponeurotic abnormality (tear and/or thickening). The athlete was asked to perform a controlled valsalva manoeuvre and the canal movement and any change in canal shape recorded as; no change, expansion (but no hernia), convex posterior wall bulging and expansion (‘ballooning’).10
MRI technique and evaluation
All MRI was performed on a 1.5 T system (Intera, Philips, Best, Netherlands or Avanto, Siemens, Erhlangen, Germany). For each MRI examination axial T2-weighted fast spin echo (TR/TE 6021/100, echo train length 8), coronal T1-weighted conventional spin echo (TR/TE 420/14) and coronal short tau inversion recovery (TR/TE 1500/17, TI 160) sequences were performed of the entire pelvis with the patient prone using the body coil (7 mm slice thickness, matrix 256×256, field of view 37.5 cm). Oblique axial (parallel to the superior aspect of the symphysis pubis and superior rami) T1-weighted conventional spin echo (TR/TE 645/20, matrix 256×256), T2-weighted fast spin echo fat suppressed (TR/TE 2269/120, matrix 512×512, echo train length 8) and T1-weighted conventional spin echo fat suppressed (TR/TE 675/20, matrix 512×384) postintravenous dimeglumine gadopentetate (Magnevist, Schering AG, Berlin, Germany) sequences were performed of the anterior pelvis using a flexible surface coil (all slice thickness 4 mm with 0.4 mm spacing, field of view 22 cm).
All examinations were prospectively evaluated independently by two experienced musculoskeletal radiologists blinded to all clinical details. Each sequence was independently assessed for abnormality in a number of anatomical areas namely; symphysis pubis assessed for spurring, effusion and cortical irregularity, capsule/tendon junction (defined as junction of capsule and enthesis of adductor/rectus abdominis tendons) assessed for soft tissue oedema but scored as a cleft if partial avulsion at tendon/capsular/enthesis junction present6 ,17 pubic body assessed for bone marrow oedema defined as subcortical only, main body or diffuse (>2 cm)16 adductor group (enthesis, tendon, muscle) and rectus abdominis assessed for soft tissue muscle or tendon oedema, inguinofemoral soft tissues assessed for soft tissue oedema or presence of a hernia and the remainder of the pelvis (including quadriceps, hamstrings, pelvic cavity, hip and sacroiliac joints) assessed for the presence of soft tissue oedema or for joints periarticular bone oedema, joint effusion and joint ganglia.
The capsule/tendon, tendon, muscle and bone marrow signal was graded using a four-point scale (0—normal, 1—mild, 2—moderate, 3—severe) for oedema (on T2-weighted sequences and enhancement (on T1-weighted postcontrast sequences)).11 ,16 Tendinopathy was scored as present if a tendon showed oedema within its substance but thickening was not considered diagnostic on its own.
Statistical analysis
The MRI scores were initially evaluated for interobserver agreement by κ analysis and then where disagreement occurred agreement for subsequent analysis was obtained by consensus. Interobserver agreement was rated as poor for a κ <0.21, moderate 0.21–0.40, substantial for 0.61–0.80 and excellent for >0.81.
For descriptive analysis where abnormality was originally graded on a four-point scale (eg, oedema or tendinopathy) scores were simplified to normal (original grade 0 or 1) or abnormal (original grade 2 or 3).17 All ultrasound and MRI features were reported relative to player symptoms which were recorded as present, absent or absent but previous symptoms.16 ,19 In players who had never been injured and also had two or more consecutive assessment results of repeated imaging assessments over time reported.
Results
We began the study with 34 players, each attending between two and four visits summarised in figure 1. All player withdrawals were due to release or transfer and none because of groin injury.

Summary flow chart of patient participation (*36 players enrolled but 2 withdrew immediately. **Withdrawals were due to transfer/release, none due to injury).
History and symptom questionnaire
At entry no players had undergone previous groin, hip or pelvis surgery. Four players were left footed, 30 right footed, 8 were strikers, 14 midfielders and 12 defenders.
At the first visit, 21 players had no current symptoms and reported no previous injuries. The examination findings showed weak or painful hip abduction and thigh adduction in 2 players, restricted hip internal rotation in 1 player with the other 18 players having a completely normal examination.
Three players had current symptoms and all showed clinical pubic tenderness with 1/3 also having weak or painful hip abduction and thigh adduction. All other findings were normal.
The remaining 10 players were asymptomatic at the time of examination but had experienced at least one episode of groin pain in the previous 2 years. Of these 10, 5 had restricted hip internal rotation and the remainder were normal on examination.
Clinical examination
At study entry clinical examination 22/34 athletes had normal findings. Three of 34 athletes had clinical pubic tenderness, 6/34 restricted hip internal rotation and 3/34 weak or painful hip abduction and thigh adduction. No players had abnormal spine, sacroiliac, hip external hip rotation or leg length examination. No players were tender on sit-up, had a cough impulse, dysaesthesia or dilated superficial ring.
Ultrasound and MRI
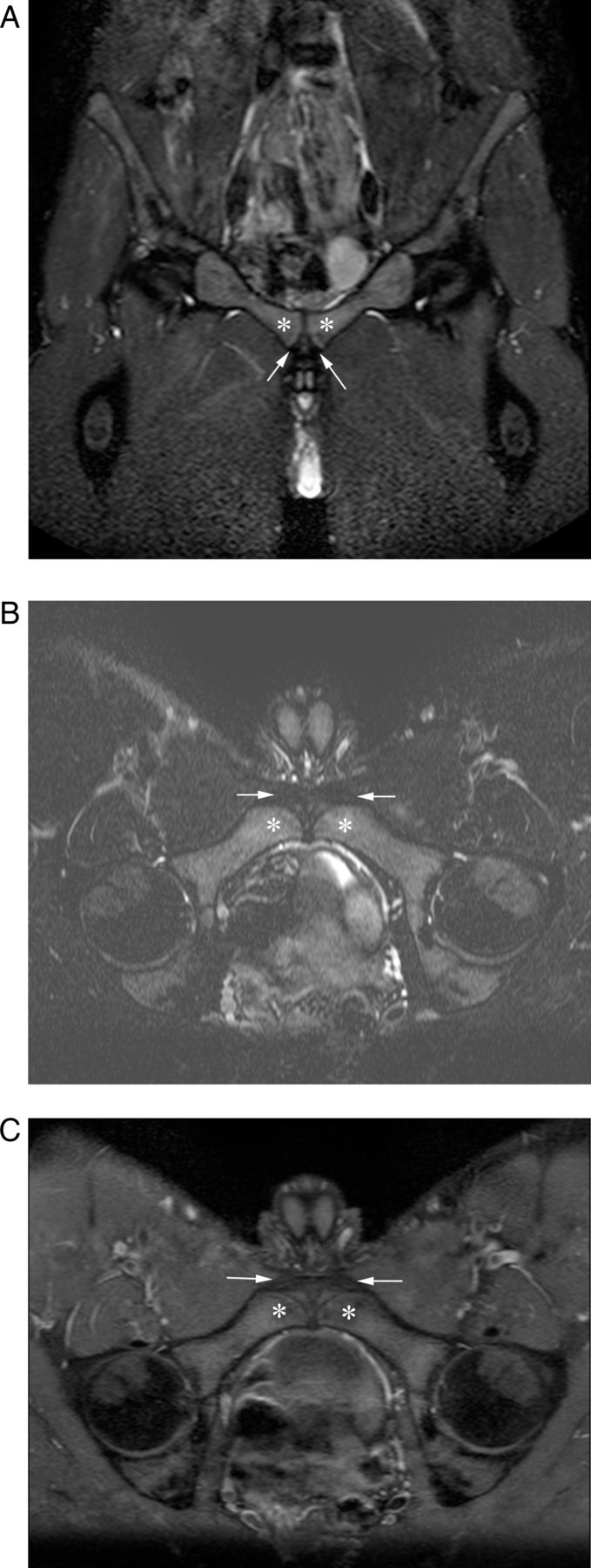
At study entry the 21 players with no current symptoms and no previous injuries MRI findings were normal (8/21), pubic bone marrow oedema (13/21; figure 2A–C), capsule/tendon oedema (4/21), cleft (2/21). Ultrasound findings were normal (8/21; figure 3A,B), inguinal canal bulging (13/21; figure 4A,B).

Sixteen-year-old male asymptomatic soccer player with normal clinical examination. (A) Coronal short tau inversion recovery, (B) axial oblique T2-weighted fat saturated and (C) axial oblique T1-weighted fat saturated post intravenous gadolinium MRI show pubic bone marrow oedema (arrows) and left capsular/tendon enhancement (arrowheads).

Sixteen-year-old male asymptomatic soccer player with normal clinical examination. (A) Transverse extended field of view and (B) sagittal sonogram show normal pubic apophyseal irregularity (arrows), echogenic capsule (arrowheads) and hypoechoic adjacent rectus abdominis and adductor longus tendons (*).

Eighteen-year-old male asymptomatic soccer player with normal clinical examination. Sagittal sonograms performed at (A) rest and (B) during Valsalver manoeuvre show the left oval inguinal canal (arrowheads) undergoing content expansion and posterior wall convexity (arrows) (‘ballooning’).
Of the three players with current symptoms MRI findings were normal (2/3), pubic bone marrow oedema (1/3) and capsule/tendon oedema (1/3). Ultrasound findings were normal (1/3), inguinal canal bulging (2/3) and labral abnormality (1/3).
Of the remaining 10 players were asymptomatic at the time of examination but had experienced at least one episode of groin pain for the five with restricted hip internal rotation MRI findings were normal (3/5), pubic bone marrow oedema (2/5), capsule/tendon oedema (2/5; figure 5A,B), cleft (1/5). Ultrasound findings were normal (2/5), inguinal canal bulging (3/5), labral abnormality (2/5). For the 5 with normal clinical examination MRI findings were normal (3/5), pubic bone marrow oedema (2/5), cleft (1/5). Ultrasound findings were normal (2/5), inguinal canal bulging (3/5).

Eighteen-year-old male asymptomatic soccer player with restricted internal right hip rotation on clinical examination. (A) Axial oblique T2-weighted fat saturated and (B) axial oblique T1-weighted fat saturated post intravenous gadolinium MRI show bilateral oedema (arrows) and enhancement at the capsular/tendon enhancement (arrowheads).
κ Analysis for MRI scoring showed excellent interobserver agreement (0.84–0.96) for radiologist scoring of pubic bone marrow oedema, subcortical oedema, secondary cleft, capsule/tendon oedema, capsule/tendon enhancement and fair to good (0.59–0.79) for all other areas including tendinopathy.
Questionnaire follow-up
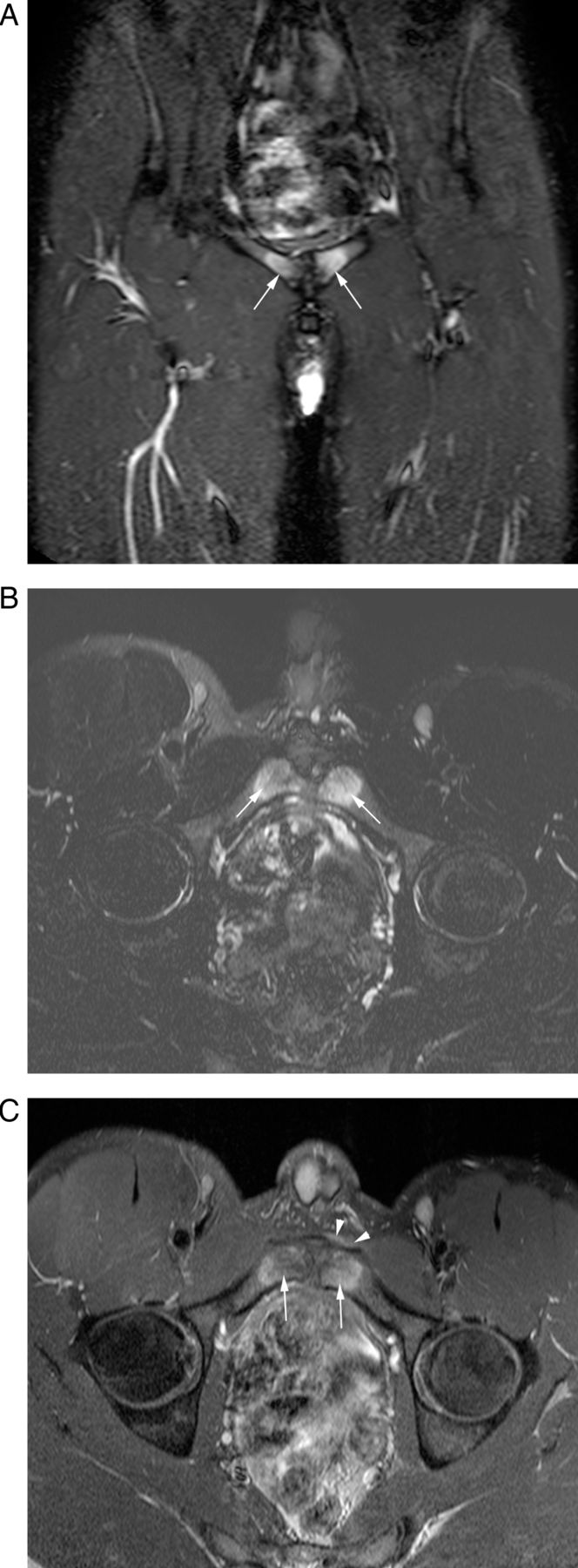
Nine players later presented with a groin injury at some point during follow-up (figure 6A–C). Questionnaires of players with current injuries all reported pain during at least one type of activity, with the number of painful activity types (out of a possible 10, see online supplementary appendix 1) ranging from 1 to 10, median 5. The most frequent painful activities were sprint (78%), weights (67%), sit-ups (67%), jog (67%), twist/cut (50%), kicking (50%), cough/sneeze (50%). The least frequent were rest, rising and walking (all 33%). Four (44.4%) reported pain at night, two (22%) reported scrotal pain, two (22%) reported back pain and six (67%) had missed training.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Nineteen-year-old male symptomatic soccer player. (A) Coronal short tau inversion recovery, (B) axial oblique T2-weighted fat saturated and (C) axial oblique T1-weighted fat saturated post intravenous gadolinium MRI show normal pubic bone (*), apophyseal and capsular/tendon junction (arrows).
Imaging follow-up
No ultrasound or MRI measures differed substantively between the players with no previous injury and those with a history of previous injury, with the possible exception of labrum abnormality (6.2% vs 31.2%). A summary of the imaging features are presented in table 1 but all other imaging features on ultrasound including anterior hip joint (apart from labrum), anterior hip muscles and tendons (iliopsoas and quadriceps group), lower abdominal muscles and adductor group muscles and tendons were normal. For MRI rectus abdominis, inguinofemoral soft tissues and the remainder of the pelvis (including quadriceps, hamstrings, pelvic cavity, hip and sacroiliac joints) were normal.
Comparison of clinical and imaging findings in players with no previous injury and players with a previous or current injury
Table 2 displays the data comparing players with and without current injury at assessment time. Only nine patients had a current injury making it difficult to assess differences between the imaging (MRI and ultrasound) assessments of those with and without injury.
Comparison of clinical and imaging findings in players with and without current injuries
In players who had never been injured findings were not completely stable over time; although the numbers with pubic bone marrow oedema decreased over time and the proportion with posterior wall bulging and capsular/entheseal soft tissue enhancement increased (table 3). There were too few players with injuries who had a subsequent scan available to provide meaningful summary data regarding changes after injury.
Comparison of imaging abnormality stability over time in players who had never been injured and had two consecutive assessments available
During the study period three players underwent surgery. One player had right capsule/tendon oedema (MRI) and bulging (ultrasound) 11 months prior to surgery when asymptomatic. When asymptomatic again 18 months postbilateral inguinal mesh repair, the ultrasound was normal and MRI showed pubic bone marrow oedema. The second player who underwent the same surgical procedure had normal MRI 1 year before and after surgery. Ultrasound 1 year before showed bulging that was not present 1 year after surgery. The third player who underwent adductor tenotomy had no postoperative scanning with serial imaging in the 3 years before surgery; entry MRI showing initial right-sided bone marrow oedema and capsule/tendon oedema and enhancement progressing to bilateral abnormality 1 year prior to surgery. This player's ultrasounds performed prior to surgery showed: on entry—asymptomatic right indirect inguinal hernia, with the years 1 and 2 examinations both showing no hernia, but right labral irregularity.
Discussion
In this prospective cohort study of elite academy soccer players the findings on history, clinical examination, ultrasound and MRI pertaining to groin injuries were examined over a 4-year period. This current study involved elite professional soccer players from four different teams which would have resulted in variation in training patterns and intensity prior to and during the study. Increased T2 signal was found in asymptomatic and previously and currently symptomatic players with no clear substantive difference between the groups. There was a trend for this bone oedema to decrease with age. In addition findings previously reported as significant abnormalities in symptomatic soccer players such as symphyseal clefts, capsule/tendon oedema and enhancement were also frequently present in asymptomatic athletes. Two previous studies have evaluated clinical and MRI findings of the pelvis in asymptomatic athletic populations namely soccer and ice hockey players.16 ,17 One study evaluated serial MRI in 19 Australian elite junior soccer players from a single club over a 4-month period.16 Of 18 truly asymptomatic players 11 had increased pubic bone marrow oedema but there was no correlation detected with subsequent symptoms or training intensity/methods. Although other parasymphyseal areas were assessed in the methods no incidence was reported in the results.16
A study of 39 asymptomatic ice hockey players was more heterogenous consisting of professional and non-professional players with no age descriptors provided.17 MRI was performed on a 3 T system and evaluated bone oedema, secondary cleft (adductor origin and capsule) and rectus abdominis tears. Oedema was present in 9/39 with moderate agreement between readers for this finding, and 7/39 clefts were detected on consensus but one reader did report a cleft in 14/39 athletes. Labral tears (22/39) and femoral osteochondritis dissecans (7/39) were also reported. Reader agreement was higher in the current study with good agreement for oedema (17/34), clefts (8/34), capsule/tendon oedema and enhancement (9/34) in asymptomatic players. It is difficult to make comparison regarding differences seen in these two studies given the different sports involved and the inability to compare player age and experience. The increased detection of hip abnormality may relate to the 3 T scanner used and the young population enrolled in our study.
Another previous study did compare asymptomatic and symptomatic soccer and ice hockey players in the same series although only one symptomatic hockey player was evaluated and the breakdown of sport for the 20 asymptomatic players was not provided.20 The asymptomatic group had a mean age of 23 years and were evaluated on a lower strength 1 T MRI system. Pubic bone marrow oedema was evaluated in a similar manner to the current study with increases seen in 8/16 symptomatic and 4/20 asymptomatic athletes. A subsequent study by the same group also showed pubic bone marrow oedema in different types of asymptomatic athletes.21
Studies in symptomatic athletes have mainly reported symphyseal bone marrow oedema and parasymphyseal oedema and cleft changes on MRI.5 ,6 ,11 The cleft equates to disruption of the soft tissue complex at the anterior aspect of the symphysis where the capsule, capsular ligaments and the enthesis of the common aponeuroses of adductor longus and rectus abdominis merge. Various authors attribute this change to rectus abdominis tear, entheseal tear, common adductor partial avulsion and in our study we classified this as a secondary cleft while capsule/tendon oedema or enhancement was recorded when there was no evidence of avulsion. Although reported in previous series as a very specific sign for current symptoms the low incidence in controls may have related to their recruitment from sports not associated with athletic groin pain.6 ,22 However the current study's results show that these imaging findings can exist in athletes in sports prone to athletic groin pain when asymptomatic. These changes presumably relate to chronic overuse through this region and it was interesting that there appeared to be a trend for bone marrow changes to decrease and capsule/tendon changes to increase as the athletes matured from 16 to 21 years; however, only a small number of players had repeat scans available therefore this would need to be formally tested in a larger group.
Ultrasound and clinical correlation/prediction of symptoms
We evaluated serial ultrasound in this athletic group. Ultrasound for assessment of athletic groin pain can be controversial with previously proposed inguinal canal bulging and ballooning subsequently not shown to be reproducible in other symptomatic series.10 ,12 Our results confirmed a variation in inguinal canal movement, including frequent bulging/ballooning, in asymptomatic players as well as inguinal hernias in three players. None of these features neither pubic cortical irregularity nor adductor tendinopathy23 correlated with subsequent symptoms but in some players posterior wall bulging and labral abnormality developed as a player aged: these findings, too, would need to be confirmed in a larger sample. Pubic cortical irregularity, probably relates to normal variation in the degree of ossification at the pubic body apophysis and was better seen on ultrasound than MRI which may relate to its higher superficial resolution however its presence had no significant relationship to symptoms as also shown in previous studies.11 ,24
Strengths and limitations
Limitations of this study include the relatively low numbers decreasing over time which did not provide good estimates of the prevalence of imaging abnormalities in the subgroups of interest. It is difficult to determine if the results of this study could provide accurate information for powering future studies because of the low incidence of injured players however our results would suggest that to determine a significant difference for the presence or absence of an imaging finding between symptomatic and control athletes would require at least 60 patients in each group. Full clinical examination was only performed on study entry as coordinating standardised examination by the same clinician over the study duration was not possible. The study started before validated scoring systems for this area were developed (eg, HAGOS) and therefore could not be used.
Conclusions
Imaging findings including pubic bone marrow and parasymphyseal abnormalities (cleft, capsule/tendon oedema) on MRI or inguinal canal ballooning on ultrasound were frequently found in asymptomatic soccer players and those with injury.
Imaging findings did not predict injury or symptom development.
What are the new findings?
-
Young elite asymptomatic athletes can have MRI abnormality in the groin.
-
Some features described as relatively specific for groin pain such as cleft and parasymphyseal capsule/tendon oedema or disruption were also present in asymptomatic athletes.
-
Bulging and ballooning inguinal canal movement on ultrasound also occurred in asymptomatic athletes.
-
The presence of abnormal imaging features did not predict future symptoms, injury or the need for surgery.
How might it impact on clinical practice in the near future?
-
Sports clinicians should be aware when referring high level athletes for MRI of the pelvis that parasymphyseal oedema can occur normally.
-
Imaging must be assessed and reported in the full context of the clinical findings and diagnosis.
-
Ultrasound evaluation of the inguinal canal does not appear reliable for detecting clinically significant movement abnormalities.
Acknowledgments
The authors would like to thank Dr P Batty, Dr S McNally, Dr M Stone, Dr C Mowbray and Dr M Waller for their help in administering the questionnaires and attendance for examination.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors PR participated in design, recruitment, image analysis, manuscript preparation and editing. PJOC and AJG participated in image analysis, manuscript preparation and editing. EMAH participated in design, statistical analysis, manuscript preparation and editing. MEB participated in clinical examination and analysis, manuscript preparation, and editing.
-
Funding The research aspects of this work were supported by grants from National Institute for Health Research, UK. The Football Association, Professional Footballers Association. British Society of Skeletal Radiologists.
-
Competing interests EMAH is supported by grants awarded to her employing institution by Arthritis UK and the National Institute for Health Research (NIHR).
-
Ethics approval University of Leeds.
-
Provenance and peer review Not commissioned; externally peer reviewed.