Article Text

Abstract
Background It has been suggested that women who are regular exercisers have a tighter pelvic floor and thereby have more difficulty during childbirth than non-exercising women. We investigated whether women exercising before and during pregnancy have a narrower levator hiatus (LH) area than their sedentary counterparts. We also studied whether regular exercise at gestational week 37 influences delivery outcome.
Methods Cohort study of 274 nulliparous pregnant women assessed at mid-pregnancy and gestational week 37 by three-dimensional/four-dimensional transperineal ultrasonography of the LH area. Exercisers were defined as those exercising ≥30 min three times per week and non-exercisers as not exercising. Exercise data were collected via electronic questionnaire at mean gestational weeks 21 and 37. Labour and delivery outcomes were collected from the women's electronic medical birth records. Differences between exercisers and non-exercisers were analysed using independent sample t test or χ2 test. p Value was set to ≤0.05.
Results At gestational week 37, exercisers had a significantly larger LH area than non-exercisers at rest and during PFM contraction (mean difference −1.6 cm2 (95% CI −3.0 to −0.3), p=0.02 and −1.1 cm2 (95% CI −2.0 to −0.1), p=0.04, respectively). No significant differences were found between exercisers and non-exercisers at week 37 in any labour or delivery outcomes.
Conclusions The results of the present study do not support the hypothesis that women exercising regularly before or during pregnancy have a narrower LH area or more complicated childbirths than non-exercising women.
Trial registration number ClinicalTrials.gov: NCT01045135.
- Core stability
- Exercise
- Physical activity promotion in primary care
- Ultrasound
- Women
Statistics from Altmetric.com
Introduction
Current guidelines encourage healthy pregnant women to participate in regular physical activity including aerobic exercise and strength training throughout pregnancy.1 ,2 A Cochrane review concluded that aerobic exercise during pregnancy appears to improve or maintain physical fitness, but that available data are insufficient to infer possible risks or benefits for the mother and child.3 Dystocia is a condition characterised by the slow, abnormal progression of labour and is the leading indication for caesarean section.4 Some concern has been raised by obstetric caregivers that sports women have difficulties in labour, mainly prolonged second stage of labour.5 In a biomechanical study modelling and simulating childbirth, Li et al6 concluded that the force required to push the baby's head through the pelvic floor was 45% greater in athletes compared with non-athletes.
The effect of general physical activity and exercise training on the pelvic floor muscles (PFM), fascia and ligaments is not well investigated or understood. One hypothesis is that general exercise training, for example, jogging or strength training of the abdominal muscles, strengthens the PFM by simultaneous unconscious co-contraction.7 This may reduce the levator hiatus area (the opening in the levator muscles which allows for the passage of the urethra, vagina and rectum) and possibly prolong the second stage of labour, and thereby increase the risk of instrumental deliveries (caesarean section, forceps and vacuum). A higher mean diameter of the PFM has been found in athletes compared with controls.8 ,9 However, a contradictory hypothesis is that general physical activity may stretch, fatigue and weaken the PFM.7 This may in turn increase the levator hiatus area, which may facilitate vaginal delivery. Several studies have shown high prevalence rates of urinary incontinence in physically active women and elite athletes,7 but there is scant knowledge about the link between general exercise, the levator hiatus area and birth outcome.5
Therefore, we investigated whether women who exercise regularly before and during pregnancy have a smaller levator hiatus area than their sedentary counterparts. Furthermore, we studied whether regular exercise at gestational week 37 influenced delivery outcome.
Materials and methods
This is a prospective cohort study following 300 nulliparous pregnant women at Akershus University Hospital, Norway. The women participated in a longitudinal study from mid-pregnancy to 12 months postpartum. The time period for inclusion was from December 2009 until October 2011. All women gave written informed consent to participate. The study followed the STROBE guidelines for observational studies.
The women were invited to participate when they attended their routine ultrasound examination at mid-pregnancy (gestational weeks 18–22). Inclusion criteria were: being in their first ongoing singleton pregnancy and being able to understand a Scandinavian language. Exclusion criteria were: multiple pregnancies or previous miscarriage after gestational week 16. Ongoing exclusion criteria were: premature birth <32 weeks, stillbirth or serious illness to mother or child. An a priori power calculation was performed for the cohort study using results from a previous study where a sample size of 47 was required to detect a 5% change in levator hiatus area at rest with a two-sided α of 0.05 and a power of 80%.10
Background variables including detailed questions on participation in exercise training were answered in an electronic questionnaire at gestational weeks 18–22 and 37. Questions covering pre-pregnancy exercise training were asked retrospectively at gestational weeks 18–22. For the purpose of the present study, exercisers were defined as women participating in regular exercise training ≥30 min×≥3 times per week. Women doing some exercise (but less than the ‘exercisers’) were excluded from the analysis. Women reporting no regular exercise were defined as non-exercisers.
A correct PFM contraction was defined as a squeeze around the pelvic openings and a lift of the perineum. Two trained physiotherapists taught the participants how to contract the PFM and ability to perform correct contractions was verified by visual observation of inward perineal movement and vaginal palpation.11
Levator hiatus dimensions were assessed at mid-pregnancy and gestational week 37 at rest and during attempts of maximal PFM contractions with a GE Kretz Voluson E8 system, 4–8 MHz curved array three-dimensional/four-dimensional transperineal ultrasound transducer (RAB4–8l/obstetric) in the lithotomy position. The levator hiatus area was measured in the axial plane of minimal hiatal dimensions using render mode. The method has shown good inter-rater reliability.12 ,13 Data on delivery outcomes were collected from the women's electronic medical birth records at the hospital. The investigators were blinded to results from the electronic questionnaire and the birth records when performing the ultrasound assessments.
Statistical analyses
Data are presented as means with SDs and differences as means with 95% CIs. Differences between groups are analysed using independent sample t test or χ2 test. Cohen’s d for independent groups was used to calculate effect size (0.2=small, 0.5=moderate, 0.8=large). p Value was set to ≤0.05.
Results
Background variables for women defined as exercisers and non-exercisers at gestational week 37 are presented in table 1. There were no statistically significant differences between exercisers and non-exercisers in age, pre-pregnancy body mass index, number of women with higher education, weight gain from before pregnancy until gestational week 37 and numbers smoking or working.
Background variables for exercisers and non-exercisers at gestational week 37
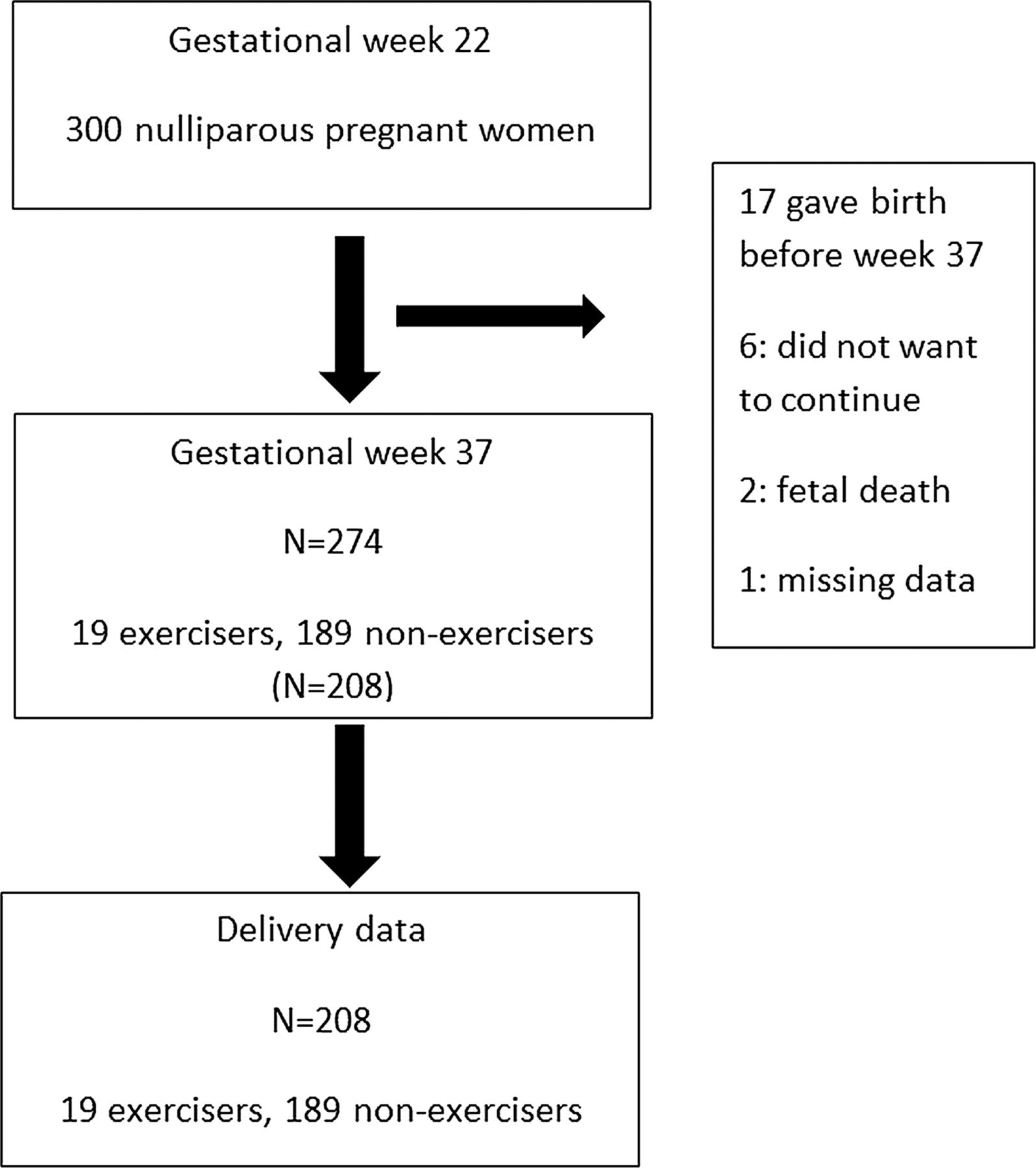
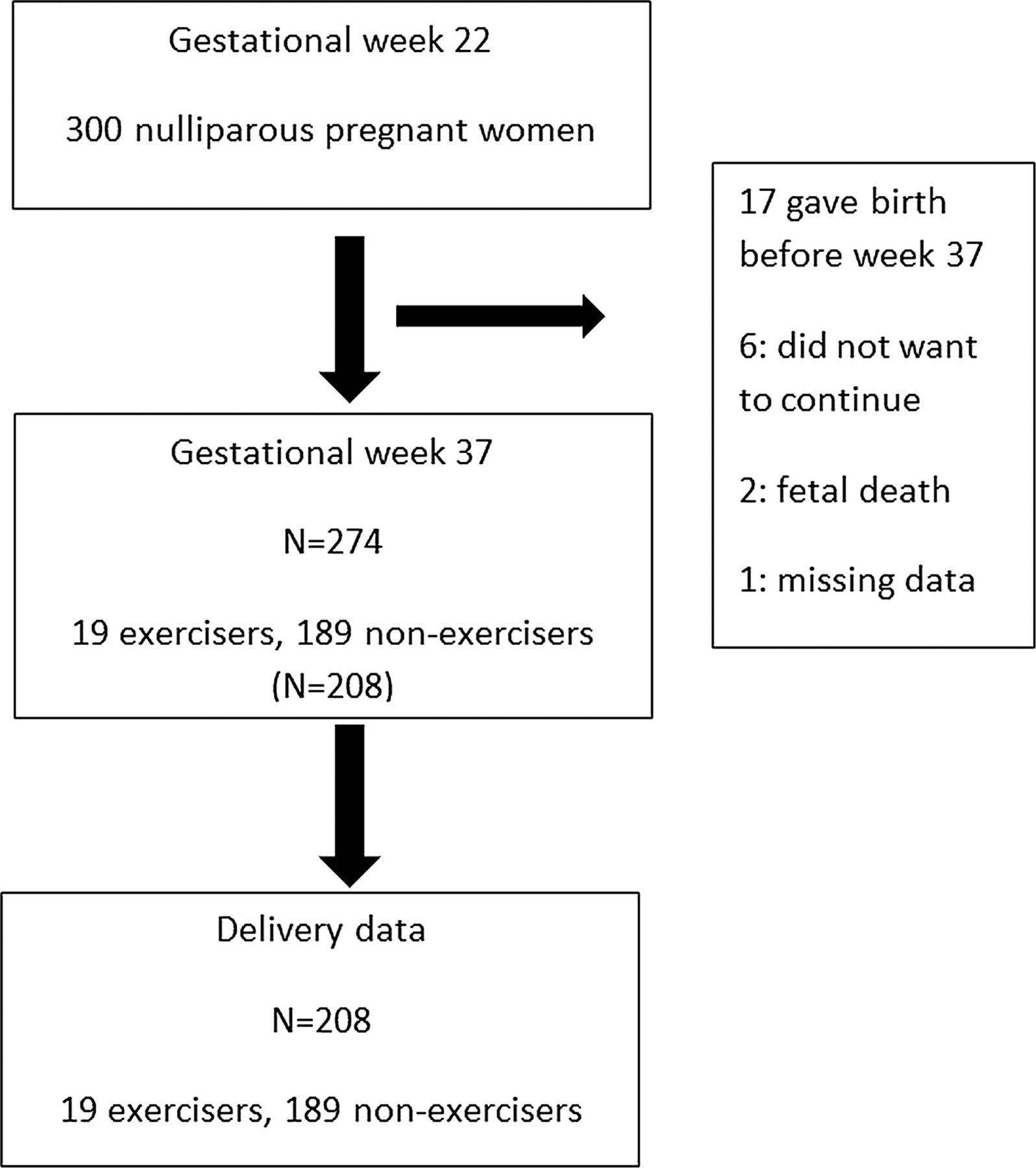
Figure 1 shows flow chart of the study. Seventeen women gave birth before their appointment at week 37, six did not want to continue and two were excluded due to intrauterine fetal death. One data set was missing at week 37 leaving 274 for follow-up at week 37. At pre-pregnancy, 136 women fulfilled the definition of being an exerciser, whereas 77 were classified as non-exercisers. At gestational week 21, 54 women were classified as exercisers and 157 as non-exercisers. At gestational week 37, 19 were exercisers and 189 non-exercisers. All 19 pregnant women exercising at gestational week 37 had been regular exercisers also pre-pregnancy and at mid-pregnancy. There was no statistically significant difference in numbers performing PFM training ≥3 times per week between exercisers and non-exercisers pre-pregnancy and at mean gestational weeks 21 and 37; 2.2% vs 0% (p=0.38), 14.8% vs 14.6% (p=0.23) and 42.1% vs 43.2% (p=0.89), respectively.
{kind=link}
Flow chart.
Comparing pre-pregnancy exercisers (n=136) with non-exercisers (n=77), there was no significant difference in the levator hiatus area at rest or during PFM contraction at mean gestational week 21: mean difference: −0.2 cm2 (95% CI −0.8 to 0.4) and −0.1 cm2 (95% CI −0.6 to 0.4), respectively. Neither was there any significant difference among pre-pregnancy exercisers and non-exercisers in the levator hiatus area at rest or during PFM contraction at mean gestational week 37: mean difference: −0.2 cm2 (95% CI −0.9 to 0.6) and 0.3 (95% CI −0.5 to 0.6), respectively.
Table 2 shows the levator hiatus area at rest and during PFM contraction at mean gestational weeks 21 and 37 among exercising and non-exercising women at these timepoints. There were no statistically significant differences at gestational week 21. At gestational week 37, exercisers had a significantly larger levator hiatus area than non-exercisers both at rest (mean difference: −1.6 cm2 (95% CI −3.0 to 0.3) and during PFM contraction (mean difference: −1.1 cm2 (95% CI −2.0 to 0.1). The effect sizes were 0.3 at rest (Cohen's d: 0.56) and 0.2 during contraction (Cohen's d: 0.47).
Levator hiatus area at rest (LHrest) and during pelvic floor muscle (PFM) contraction (LHcontr) at mean gestational weeks (GW) 21 and 37 among exercisers and non-exercisers at GW 21 and 37
Table 3 shows no significant difference in labour and delivery variables or infants’ birth weight between exercisers and non-exercisers at mean gestational week 37.
Number of women with induction, prolonged second stage, elective and acute caesarean section, episiotomy, operative vaginal delivery, third and fourth degree perineal tear and infants’ birth weight among exercisers (N=19) and non-exercisers (n=189) at gestational week 37
Discussion
For some women, exercise during pregnancy, particularly PFM training is associated with a fear of ‘difficult delivery’. We showed that the levator hiatus area was larger in women exercising regularly at gestational week 37 than in non-exercisers at this timepoint. This difference was not associated with labour and delivery variables as there were no statistical significant differences between exercisers and non-exercisers at week 37 in numbers with induction, prolonged second stage, elective or acute caesarean section, episiotomy, operative vaginal delivery (vacuum and forceps), women with third and fourth degree perineal tears and infants’ birth weight.
Our data extend findings of decreased physical activity level during pregnancy in other larger cohort studies.14 ,15 In the Norwegian Mother and Child Cohort Study, women exercising ≥3 times per week decreased from 46% before pregnancy to 28% at gestational week 17 and to 20% at gestational week 30.15 Similar trends have been found in cohort studies from other countries.16 A low number of regular exercisers at gestational week 37 is consistent with the progressively increasing weight of the baby and postural changes which tend to limit physical activity. Exercise intensity and duration decreases as pregnancy progresses.16 A low number of exercisers at week 37 threatened to potentially influence our ability to find statistically significant differences for variables between groups. However, we found significant differences in the levator hiatus area; exercising women had a larger levator hiatus area (essentially the opening for the baby to pass through) than non-exercisers at rest and during PFM contraction.
Today, all pregnant women are encouraged to train the PFM to prevent and treat urinary incontinence.17 Previous randomised controlled trials (RCTs) and one large cohort study concluded that there were no negative effects of PFM training on delivery outcomes.18–21 There is scant knowledge on the effect of general exercise on second stage of labour and other delivery outcomes.16 Two recent RCTs did not find any effect of a combination of PFM training and aerobic exercise twice a week on second stage of labour.22 ,23 The present study adds information about the effect of general exercise alone on pelvic floor morphology during pregnancy, as the number of women performing PFM training did not differ between exercisers and non-exercisers.
As far as we have ascertained, this is the first study measuring the levator hiatus area in exercisers and non-exercisers during pregnancy. Our results indicate a wider levator hiatus area in exercisers compared with non-exercisers; this does not support the hypothesis that exercise training narrows the levator hiatus area.5 Importantly, at gestational week 37, there was no negative effect of regular exercise on duration of second stage of labour or other delivery outcomes.
A Cochrane review concluded that the few RCTs reporting effect of aerobic exercise during pregnancy on delivery outcomes were inconclusive.3 Melzer et al16 concluded that further studies with larger sample sizes are required to confirm the association between physical activity and labour and delivery outcomes. The results of the present study support the premise that regular exercise training before and during pregnancy does not negatively influence delivery outcome.
Supervised PFM training significantly narrowed the levator hiatus area by 4.6% in a group of middle-aged women with pelvic organ prolapse.10 To date, there are no data available on the effect of regular, supervised PFM training on the levator hiatus area during pregnancy. However, it is likely that the same effect would be found in pregnant women performing intensive PFM training. Narrowing of the levator hiatus area is considered positive in women with pelvic floor dysfunction such as urinary incontinence and pelvic organ prolapse. In the present study, the amount of unsupervised PFM training was equal in exercisers and non-exercisers and can therefore not be considered a confounding factor.
Our results do not support the findings obtained in a qualitative interview of nine obstetric caregivers who perceived that athletic women tended to have more difficult deliveries.5 They defined athletic women as women participating in high impact, frequent, intense training. However, their study was based on retrospective recall of such athletes, and no assessment of the PFM or birth outcome was presented. In another study, Kruger et al9 showed that although a higher mean diameter of one of the PFM was found in elite athletes, a greater bladder neck descent and a larger levator hiatus area was found during Valsalva compared with controls. Our study did not include elite athletes and we did not test the levator hiatus area during Valsalva. The results may be different in a group of women exercising more frequently and with higher intensity than what the case was in our study.
Further prospective studies are warranted in pregnant elite athletes. However, as pointed out, it is important that the maternal population, which by large is mostly inactive,24 can be reassured that recommended exercise ≥3 times per week before and during pregnancy does not negatively influence the pelvic floor, labour or vaginal delivery. In a recent study from our group, fewer than 15% of Norwegian pregnant women followed recommendations for exercise during pregnancy at gestational weeks 17–21.25 Hence, recommendation to the general pregnant population to start or continue regular exercise training is important.26
Our study fills in the missing link between general exercise training and the levator hiatus area, and supports that exercisers do not have a narrower levator hiatus area or more difficult births. More studies are needed to elaborate on a possible negative influence of a wider levator hiatus area in exercisers on prevalence and severity of urinary incontinence and pelvic organ prolapse.7
Strengths of the present study are a high number of participants, use of ultrasonography and blinding of investigators. We used an ultrasound measurement method found to have good intra-rater and inter-rater reliability, and trained gynaecologists performed the ultrasound assessments and analysis.12 ,13 Comparing possible known confounding variables between exercisers and non-exercisers at gestational week 37, no significant differences were found. Limitations are that the number of pregnant women exercising ≥3 times per week at gestational week 37 is low, and that level of exercise training was assessed with a questionnaire and not more objective measures. Self-report may overestimate training estimates, and recall bias is a possible threat to the accuracy of self-reporting in general.27 However, self-report is the most commonly used assessment method for surveillance, interventional and epidemiological studies during pregnancy, and it has been shown to have good reliability and validity in many studies.28 In the present study, the participants were asked about physical activity levels at the timepoints when the ultrasound assessment took place. The only retrospective data were on pre-pregnancy activity level. A limitation of our study is the design. RCTs comparing exercising and non-exercising women using ultrasonography to assess the levator hiatus area and other PFM variables are warranted.29 ,30 Addressing the influence of regular exercise training during pregnancy on delivery outcomes, our results are in line with those of Barakat et al,31 ,32 with no negative effects reported.24
Conclusions
Our results do not support the hypothesis that exercising in pregnant women reduces the levator hiatus area or negatively influences delivery outcomes. Exercising women at week 37 in the present study had a significantly larger levator hiatus area at week 37, and there was no difference between exercisers and non-exercisers on labour or delivery outcome. There is a need for further studies on a possible association between the levator hiatus area and pelvic floor dysfunctions such as urinary incontinence and pelvic organ prolapse in exercising pregnant women.
What are the new findings?
-
Exercising pregnant women do not perform more pelvic floor muscle training than non-exercisers.
-
Exercising women have a significantly larger levator hiatus area than non-exercisers at gestational week 37 (a larger levator area is associated with pelvic organ prolapse in other studies).
-
Participating in regular exercise at gestational week 37 did not narrow the levator hiatus area and had no influence on delivery outcome.
How might it impact on clinical practice in the near future?
-
Health personnel might stop telling physically active women that they may have difficult vaginal deliveries.
-
Health personnel may encourage women to be physically active throughout pregnancy.
-
Health personnel may encourage pregnant women to do pelvic floor muscle training.
Acknowledgments
The authors thank midwife Tone Breines Simonsen for recruiting participants and administering clinical appointments and electronic questionnaires; physiotherapist therapist Kristin Gjestland for clinical testing and data entering; and professor Ingar Holme, PhD, Norwegian School of Sport Sciences, for statistical advice.
References
Footnotes
-
Contributors KB planned, conducted and reported the study. She was the project leader and is the guarantor of the study. GH, JS-J and FS conducted and reported the study. MKT participated in data analysis and reported the study. MEE planned and reported the study.
-
Funding This study was supported by grants from the South-Eastern Norway Regional Health Authority and the Research Council of Norway.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Regional Medical Ethics Committtee (2009/170) and the Norwegian Social Science Data Services (2 799 026).
-
Provenance and peer review Not commissioned; externally peer reviewed.