Article Text

Abstract
Objectives The short QT syndrome is a cardiac channelopathy characterised by accelerated repolarisation which manifests as a short QT interval on the ECG. The definition of a short QT interval is debated, ranging from <390 to ≤320 ms, and its clinical significance in healthy young individuals is unknown. We assessed the prevalence and medium-term significance of an isolated short QT interval in a diverse young British population.
Methods Between 2005 and 2013, 18 825 apparently healthy people aged 14–35 years underwent cardiovascular evaluation with history, physical examination and ECG. QT intervals were measured by cardiologists using 4 recommended guidelines (Seattle 2013, Heart Rhythm Society 2013, European Society of Cardiology 2010 and American Heart Association 2009).
Results The prevalence of a short QT interval was 0.1% (26 patients, ≤320 ms), 0.2% (44 patients, ≤330 ms), 7.9% (1478 patients, <380 ms), 15.8% (2973 patients, <390 ms). Male gender and Afro-Caribbean ethnicity had the strongest association with short QT intervals. Athletes had shorter QT intervals than non-athletes but athletic status did not predict short QT intervals. Individuals with short QT intervals ≤320 ms did not report syncope or a sinister family history, and during a follow-up period of 5.3±1.2 years, there were no deaths in this group.
Conclusions The prevalence of a short QT interval depends on the recommended cut-off value. Even at values ≤320 ms, there was an excellent medium-term prognosis among 14 people followed. We conclude that a definition of ≤320 ms is realistic to prevent overdiagnosis and excessive investigations.
- Cardiology
Statistics from Altmetric.com
Introduction
The short QT syndrome is a relatively novel hereditary cardiac ion channel disorder associated with sudden cardiac arrest in individuals with a structurally normal heart. The disease is characterised by accelerated repolarisation which manifests as a short QT interval on the resting ECG. The definition of a short QT interval by various learned expert consensus panels varies greatly from <390 to ≤320 ms).1–4 In contrast to the long QT syndrome, data relating to the prevalence, diagnosis, risk stratification, treatment and prognosis of the short QT syndrome are scarce.
Population studies in middle-aged individuals reveal that extremely short QT intervals (<320 ms) are uncommon, and their association with symptoms or adverse events is exceedingly rare.5 Conversely, other reports suggest that short QT syndrome has an unfavourable natural history.6 ,7
Whether short QT intervals pose a risk of sudden cardiac death in apparently healthy adolescent and young adult populations has not been established; however, sudden cardiac arrest in this cohort, particularly in athletes, is highly scrutinised.8 There are sex differences in the prevalence of short QT intervals, but the influence of ethnicity and athletic status on the prevalence of short QT interval is not established.
The purpose of this study was to establish the prevalence and significance of a short QT interval in a large population of healthy young individuals (age 14–35 years) in the UK, which included a high proportion of athletes.
Methods
Setting
The UK does not support a national, state-sponsored cardiac screening programme. However, many sporting organisations and an increasing number of high schools recommend cardiac evaluation to help identify young persons who harbour a potentially serious cardiac condition that may trigger a fatal arrhythmia during exercise. Most evaluations in elite athletes competing at the regional or national level are funded by sporting associations, whereas high school children are tested through a self-funded but highly subsidised programme conducted by the charity Cardiac Risk in the Young (CRY). The charity also provides subsidised screening for conditions predisposing to sudden cardiac death in individuals aged 14–35 years in the UK who wish to be tested, irrespective of athletic status, symptoms or family history of premature cardiac disease. Screening events are advertised in the local media and on the CRY website (http://www.c-r-y.org.uk). Individuals from the general population, including those from local high schools, self-present to screening events, whereas competitive athletes attend specified screening events endorsed by their relevant sporting bodies. From this approach, CRY assesses individuals who self-refer and who attend via sporting clubs, with the vast majority being those who self-refer from the general population. The senior author (SS) is the cardiac expert for the CRY screening programme.
Participants
Between 2005 and 2013, 19 742 consecutive individuals aged 14–35 years underwent cardiac evaluation by CRY, comprising a health questionnaire and a 12-lead ECG. Individuals with T-wave inversion, ST segment depression, bundle-branch block or pre-excitation were excluded from the study (N=917) because these electrical patterns are markers of cardiac diseases implicated in arrhythmogenic sudden cardiac arrest or sudden cardiac death in the young population. Bundle-branch block also affects the length of the QT interval. The total number of individuals studied was 18 825.
Definitions
Athletes were defined as individuals competing in organised team or individual sports at regional, national or international levels with a high premium on athletic excellence. Individuals who exercised recreationally more than 10 h/week were also included in the athlete cohort. Ethnicity was self-reported, with particular focus on Caucasians and Afro-Caribbeans who constitute the two largest ethnic cohorts in the UK.
Twelve-lead ECG
A resting 12-lead ECG was performed in a supine position using a Philips Pagewriter Trim III recorder (Philips, Bothell, Washington) with a paper speed of 25 mm/s and amplification of 0.1 mV/mm. The QT interval was measured by the tangent method.9 The highest QT value was quoted as the absolute QT value. The QT interval was corrected for heart rate using Bazett’s formula.10 Short QT intervals were defined using recommended cut-offs recommended in four relevant guidelines:the Seattle criteria (2013)4 (≤320 ms), Heart Rhythm Society (2013)3 (≤330 ms), European Society of Cardiology (2010)2 (<380 ms) and the American Heart Association (2009)1 (<390 ms).
Each ECG was read by 1 of 12 cardiologists trained in inherited cardiac diseases, including the ion channelopathies. These cardiologists read the ECGs in the course of their normal clinical work after a consensus meeting to ensure uniform measurements of the QT duration. A selected sample of 1800 ECGs which included 180 ECGs with a QT interval ranging from <320 to <390 ms was used to test agreement between two qualified observers. In cases of disagreement, the senior author (SS) and ERB adjudicated by consensus.
Individuals with a QT interval ≤320 ms were followed up for an adverse cardiac event through an e-mailed patient questionnaire or interaction with a primary care physician on a 2-yearly basis.
Statistical analysis
Statistical analysis was performed using SPSS software revision 17 (Chicago, Illinois, Chicago, USA).The Kolmogorov-Smirnov test was used to test the normality of distribution. Values are expressed as mean±SD or percentages as appropriate. The comparison of means of heart rate and QT intervals between groups was performed using two-sample t tests. The proportion of patients with short QT intervals was compared between groups using χ2 tests. The effects of covariates (including sex, ethnicity and athletic status) on short QT intervals were investigated using a logistic regression model. A two-tailed p value <0.05 was considered to define statistical significance.
Ethical approval
Ethical approval was granted by the Essex 2 Research Ethics Committee. Written consent was obtained from individuals ≥16 years of age and from a parent/guardian for those 15 years of age and below. Individuals also consented to be contacted for follow-up at any time from the initial screening.
Results
Demographics
Of the 18 825 participants, the majority were male (72%) and Caucasian (89%). The proportion of athletes and non-athletes was similar (table 1).
Demographics of the study population
Heart rate
Athletes had a lower heart rate than non-athletes (63.6±11.4 vs 69.6±12.6; p<0.0001). Among non-athletes, males had a lower heart rate than females (67.9±12.5 vs 72.6±12.2; p<0.001), but there was no difference in heart rate between Caucasians and Afro-Caribbeans (69.4±12.7 vs 69.1±11.3; p=0.759).
The QT interval
The mean QT interval was 412±23 ms (range 310–535 ms). The mean QT intervals for Caucasian men and women were 410±23 and 419±22 ms, respectively. The mean QT intervals for Afro-Caribbean men and women were 394±25 and 407±24 ms, respectively. Males and individuals of Afro-Caribbean origin had QT intervals 10.0 and 16.5 ms shorter than female and Caucasian counterparts, respectively (table 2). Individuals aged ≥16 years also had shorter QT intervals than those who were younger (410.8 vs 414.5 ms; p<0.001).
Mean QT intervals per population demographic
Short QT intervals
The prevalence of short QT intervals in the cohort studied depending on the definition used was 15.8% (n=2973; America Heart Association, <390 ms), 7.9% (n=1478; European Society of Cardiology (ESC) criteria; <380 ms), 0.2% (n=44; Heart Rhythm, ≤330 ms) and 0.1% (n=26; Seattle criteria, ≤320 ms) (figure 1). In all four short QT interval ranges, the prevalence of males was higher than that of females and the prevalence of Afro-Caribbeans was higher than that of Caucasians (table 3).

The prevalence of a short QT interval as per consensus definition values.1–4
Short QT intervals and pre-participation screening guidelines for athletes
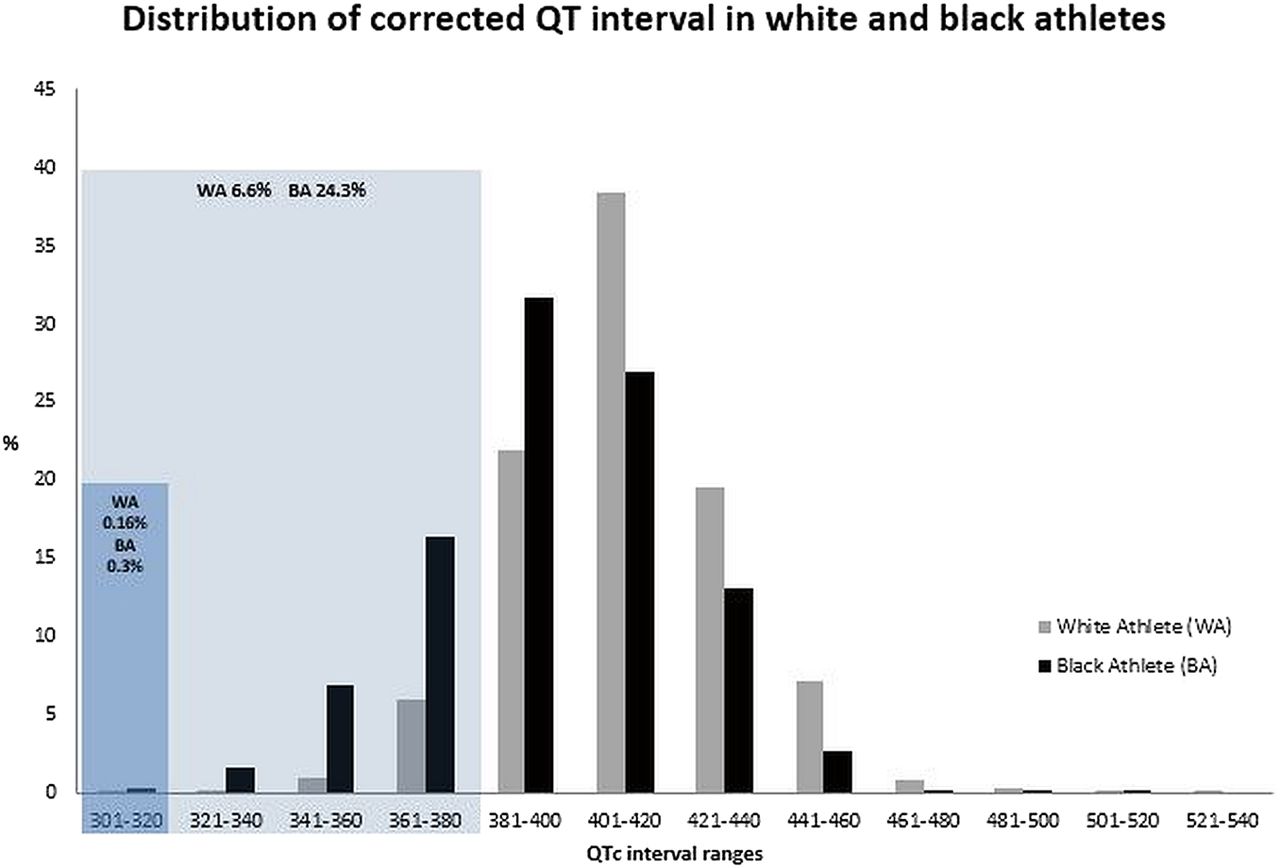
The proportion of athletes with a short QT interval using the ESC criteria definition (<380 ms) and the Seattle Criteria definition (≤320 ms) was 8.62% and 0.17%, respectively. The discrepancy was greatest among athletes of Afro-Caribbean origin (24.3% vs 0.3%) (figure 2). There were no significant differences in the prevalence of a short QT interval between athletes and non-athletes according to the Seattle criteria definition of QT ≤320 ms.

Histogram depicting the distribution of values for corrected QT intervals in Caucasian and Afro-Caribbean athletes. The percentages of athletes exhibiting QT intervals according to the 2010 European Society of Cardiology recommendations (light blue) and Seattle criteria (dark blue) are demonstrated.2 ,4
Association of short QT intervals
Using the Seattle criteria definition based on the shortest QT interval (≤320 ms) and adjusting for all demographic variables, male sex (OR=2.9; 95% CI 0.9 to 9.9; p=0.0434) and Afro-Caribbean ethnicity (OR=4.6; 95% CI 1.8 to 11.5; p=0.0003) were the strongest predictors for a short QT interval.
Athletic status had some predictive value for the presence of a short QT interval ≤320 ms but this was not statically significant (OR 1.3 95% CI 0.6 to 3.3; p=0.2949).
Symptoms, family history and follow-up in individuals with QT≤ 320 ms
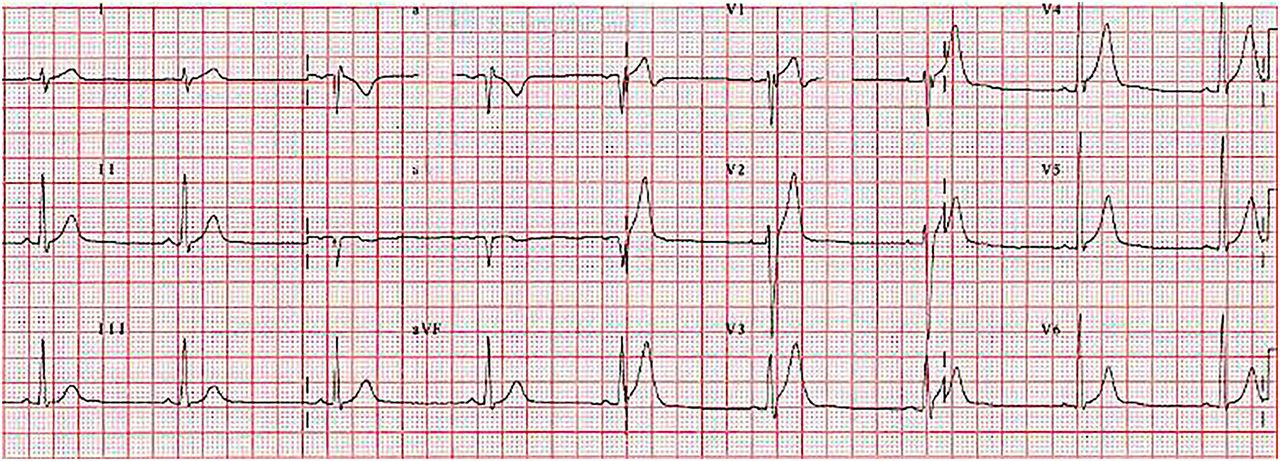
Twenty-six individuals (0.1%) had a QT interval of ≤320 ms (figure 3). Of these 20 (76%) were male. None reported syncope at the time of examination. A 20-year-old Afro-Caribbean man with a QT interval of 318 ms and a 16-year-old Caucasian boy with a QT interval of 320 ms reported chest pain and dyspnoea, but these were not considered to be of cardiac origin by the assessing clinician, and did not warrant further evaluation after physical examination. Only one individual, a 17-year-old Caucasian boy with a QT interval of 318 ms, had a family history of unexplained and unexpected death in a first degree relative aged <50 years; that relative had not undergone post mortem examination to determine cardiac structure. At the time of cardiovascular evaluation, none of the patients were taking prescription medication.
{kind=link}
{kind=link}
{kind=link}
A 12-lead ECG of a 17-year-old asymptomatic Caucasian man demonstrating a short QT interval (QT 318 ms)
Of the 26 individuals with a QT interval ≤320 ms, 21 consented to be followed up. Follow-up data over a period of 2–7 years (mean 5.3±1.2 years) from the initial evaluation was available for only 14 of these individuals, and was obtained either via the participant's primary care physician (n=8) or by direct patient questionnaire (n=6). There were no adverse symptoms such as syncope or deaths reported in any of these participants.
Interobserver variability
Samples of 1800 ECGs containing 10% cases of a short QT interval were reported by two qualified cardiologists. The raw numbers of ECGs per cut-off recommendations as assessed by the two observers are in table 4. There was substantial agreement between the observers for detecting short QT intervals (κ coefficient, 0.78±0.04).
Breakdown of ECGs per cut-off recommendations1–4 as assessed by two cardiologists
Discussion
The short QT syndrome has been reported to have an adverse natural history based on the relatively small series of patients.6 ,7 Our study is the first to address the prevalence and significance of a short QT interval in the young adult population. Our cohort included a high proportion of athletes. This is pertinent given that the prevention of sudden death in young athletes due to underlying cardiac conditions has emerged as a major focus for the sports cardiology community.
Prevalence of a short QT interval in various populations
The prevalence of a short QT interval ≤320 ms in this population was 0.1% (26 participants). This figure was at least five times higher than that reported in Swiss adults aged 18–19 years11 and a Japanese population aged 53±20 years.12 The prevalence we report is however comparable with that in a middle-aged Finnish population, where the prevalence of QT interval <320 ms was 0.1% and <340 ms was only 0.4%.5
Males had a shorter mean QT interval than females and a QT ≤320 ms was predominantly confined to males (table 3). This sex difference, postulated to be due to blood testosterone concentrations, has also been demonstrated in other population studies.5 ,11 ,13 We note that males aged ≥16 years had shorter QT intervals than younger participants did in our cohort. Sex differences are considered in cut-off values for a long QT interval,2 ,3 ,4 but there are no sex-based definitions for a short QT interval.
Our study is also the first to evaluate the impact of ethnicity on the prevalence of a short QT interval in a healthy population. We observed that both male and female individuals of Afro-Caribbean origin had shorter QT intervals than their Caucasian counterparts. The reason for these ethnic differences is unclear, but similar to sex differences, blood testosterone concentrations in Afro-Caribbean males are significantly greater than in Caucasian males.14 As far as the authors are aware, there are no studies reporting higher testosterone concentrations in Afro-Caribbean versus Caucasian females, suggesting that other confounding factors may be responsible.
Why has a short QT interval been flagged as a potentially fatal finding?
During the 30-year follow-up in the Finnish study above, abnormally short QT intervals <320 ms did not predict an increase in sudden cardiac death.5 Similarly, in more than 12 000 Japanese individuals,15 the prevalence of QT <300 ms was 0.03% and was not associated with symptoms or increased risk of SCD. In our diverse cohort of young individuals, we did not ascertain a history of syncope, a definitive family history or an increased risk of sudden cardiac death in participants with QT intervals ≤320 ms.
The interest in investigating short QT intervals has been generated by studies reporting a possible adverse natural history in individuals with short QT syndrome.6 ,7 In a series of 73 young patients with short QT syndrome who were followed for a period of nearly 5 years, Mazzanti et al6 reported that the probability of sudden cardiac arrest was 41% by the age of 40 years. This study differed from our study and other population studies in many respects. The investigators evaluated patients with a suspected diagnosis of short QT syndrome who were referred for evaluation in a tertiary specialist centre; therefore, the study was prone to unavoidable ascertainment bias. A considerable proportion of the cohort comprised symptomatic individuals including survivors of sudden cardiac arrest and patients with a family history of sudden cardiac arrest. This study also included infants, which is relevant because a significant number of cases of cardiac arrest (15%) occurred in the first year of life. Finally, the only predictor of a sudden death was a previous aborted cardiac arrest. These differences may explain why a short QT interval was not associated with adverse events in our cohort of adolescents and young adults, in whom symptoms or a family history of sudden arrhythmic death syndrome were absent.
Short QT interval as a marker of short QT syndrome
The overlap in the range of QT intervals between individuals with short QT syndrome and healthy members of the general population suggests that sole reliance on the ECG alone has poor diagnostic and prognostic value in short QT syndrome. These considerations have led to the development of scoring systems similar to those in patients with long QT syndrome16 to provide uniformity for the diagnosis of short QT syndrome. Gollob et al17 proposed ‘the Gollob score’ based on the ECG, clinical history and genotyping to improve the accuracy of the diagnosis of short QT syndrome in suspected individuals. The electrocardiographic section weight scores for QT interval corrected for heart rate as follows: 1 point for QT <370 ms, 2 points for QT <350 ms and 3 points for QT <330 ms. When applied to 61 symptomatic and asymptomatic patients with short QT syndrome, a Gollob score of ≥4 points identified 58 of these individuals providing a sensitivity of 95%.17
The scoring system is appealing; however, the Gollob criterion has not been validated in independent short QT syndrome populations. Furthermore, its efficacy of risk stratification has not been proven. Our study did not comprehensively evaluate individuals with short QT intervals with 24 h ECG and genetic testing; however, the absence of cardiac events in 14 asymptomatic young individuals with QT intervals ≤320 ms (which would represent the greatest weight for the criterion) in the medium term questions the prognostic value of the Gollob ECG criterion.
Clinical implications for sports medicine and pre-participation screening guidelines
To identify young athletes at risk of exercise-related sudden cardiac death, pre-participation screening is recommended by a growing number of sporting bodies and scientific organisations worldwide.18 The 2010 ESC recommendations and the 2013 Seattle Criteria have proposed guidelines for the interpretation of the athlete's ECG.2 ,4 The ESC and Seattle criteria define a short QT interval to raise suspicion of the short QT syndrome as <380 and ≤320 ms, respectively. The Seattle recommendations use a cut-off value that represents the first centile of the QT distribution in the general population;19 therefore, only 1% of individuals will continue to remain as outliers.
On the basis of these values, nearly 9% of athletes had a short QT interval if the ESC recommendations are applied, which is likely to overestimate the prevalence of short QT syndrome given the rarity of the condition, and could lead to anxiety, unnecessary investigations or even erroneous disqualification for the athlete. Implementation of the Seattle criteria would result in only 0.17% of athletes having a short QT interval, a 50-fold lower number compared to the ESC recommendations. Among athletes of Afro-Caribbean ethnicity, the prevalence of a short QT interval is 80-fold lower when the Seattle criteria are applied compared with the ESC recommendations. Given the lack of any association between a QT interval ≤320 ms and symptoms or sudden cardiac death, we suggest that the ≤320 ms cut-off is appropriate.
Our results and data from other population studies justifiably question the value of a short QT interval in isolation as a marker of short QT syndrome in low-risk populations and its inclusion in any ECG interpretation criteria in young athletes. While athletes in our cohort had slightly shorter QT intervals than non-athletes, the association between athletic status and the presence of QT interval ≤320 ms was not statistically significant. Therefore, we do not recommend more specific short QT ranges in the athletic population compared to the general population.
Limitations
Our study has some important limitations that warrant mention. The follow-up of patients with a short QT interval ≤320 ms was limited to a maximum of 7 years, and medium-term follow-up data were available in only 54% of individuals; therefore, we cannot claim with confidence that a short QT interval is always benign. However, deaths from the CRY screening programme are highly scrutinised by the charity through self-reporting and media searches, and none of the individuals with a QT interval ≤320 ms feature in the fatality list over the past 10 years. All the ECGs were undertaken at a single moment in time, whereas it is well recognised that the QT interval varies throughout the day.
Summary
In our study of 18 825 young individuals, a short QT interval (≤320 ms) was rare (0.1%) and was not associated with adverse cardiac events in the medium term (2–7 years). This study suggests that in adolescents and young adults, a short QT interval in isolation is not sufficient to make a diagnosis of short QT syndrome. For ECG interpretation in athletes, a short QT definition of ≤320 ms seems to be most pragmatic to avoid a large number of false-positive results.
What are the findings?
The prevalence of a short QT interval varies widely, from 15.8% (<390 ms) to 0.1% (≤320 ms), depending on which of four current guideline definitions are applied.
Gender and ethnicity influence the QT interval. Males are three times more likely to have a short QT interval (≤320 ms) than females, and Afro-Caribbean individuals are five times more likely to have a short QT interval than Caucasians.
Even when QT intervals are ≤320 ms, they are associated with an excellent medium-term prognosis. This questions the value of a short QT interval as a marker of short QT syndrome in adolescents and young adults in the absence of symptoms or of a family history of sudden arrhythmic death syndrome.
Applying the 2013 Seattle criteria for ECG interpretation results in a 50-fold lower rate (8.62% vs 0.17%) of athletes with suspected short QT syndrome compared to the 2010 European Society of Cardiology recommendations.
How might it impact on clinical practice?
A short QT interval in isolation has poor medium term diagnostic and prognostic value, and should not be solely relied on to diagnose short QT syndrome in young individuals.
The European Society of Cardiology definition for a short QT interval in athletes (<380 msec) is associated with a high false positive rate. The Seattle criteria definition (≤320 msec) is more pragmatic for ECG interpretation guidelines in athletes.
References
Footnotes
Twitter Follow Harshil Dhutia at @harshil_dhutia
Contributors HD contributed to study design, planning data collection, conduct and preparation, reporting of manuscript. AM, VG, GF, GM, AM, LM, RN and NS contributed to design, data collection and preparation of manuscript. SP contributed to statistics and methodology preparation. MP and ERB contributed revision of manuscript for intellectual content. SS was involved in study design, data collection, quality control of data, preparation of manuscript and responsible guarantor of overall content.
Funding HD, AM, VG, GF, GM, AM, LM, RN, NS and MP were funded by research grants from CRY. ERB and SS have been co-applicants on previous grants from CRY to study athletes and young individuals in the general population.
Competing interests None declared.
Ethics approval Essex 2 Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.