Article Text

Abstract
A systematic review to determine if exercise alone or as part of a comprehensive intervention can improve self esteem in children and young people is described.
Twenty three randomised controlled trials were analysed. A synthesis of several small, low quality trials indicates that exercise may have short term beneficial effects on self esteem in children and adolescents. However, high quality research on defined populations with adequate follow up is needed.
- SMD, standardised mean difference
- CI, confidence interval
- children
- exercise
- self esteem
- systematic review
- meta-analysis
Statistics from Altmetric.com
Between 10% and 20% of children and adolescents have psychological and behavioural problems and about 7% need psychological treatment.1,2 Resilience research has led to an increasing awareness of positive factors in the environment, social relations, and individuals that protect against the development of problems.3–,5 Among individual qualities, self concept is one of the indicators given most attention. Self concept is defined as an “organised configuration of prescriptions of the self which are admissible to awareness”.6 The evaluative component of self concept used in this article, self esteem, is “the degree to which individuals feel positive about themselves”.6
Systematic reviews indicate a positive effect of physical activity on depression, anxiety, and behavioural problems in children and adolescents.7–,9 The effect of physical activity on self esteem in children has also been investigated,10 and one meta-analysis concluded that directed play and/or physical education programmes contributed to the development of self esteem in elementary school age children.11 This and other reviews have not been updated and lack description of systematic search and quality assessment of the included studies.8,9
The aim of this systematic review is to determine if exercise interventions can improve self esteem among children and young people.
METHOD
Searching
Searches were conducted in the Cochrane Controlled Trials Register (CENTRAL) (Issue 1, 2004), Medline (1966–2002), Embase (1982–2002), CINAHL (1982–2002), PsycINFO (1887–2002), and ERIC (1965–2002). The search terms were a wide range of terms about children and young people, physical activity, and self esteem. The complete search strategy is available in the original publication.12 The authors of included studies were contacted, and the Journal of the American Academy of Child and Adolescent Psychiatry was hand searched (1998–2002). There were no language restrictions.
Selection
Inclusion of studies was restricted to randomised controlled trials and “quasi-randomised” trials—that is, a study that uses methods of allocation that are subject to bias in assignment, such as alternative allocation, case record numbers, dates of birth—with children from 3 years of age to young people up to 20 years old. Trials with children and young people with psychotic or borderline conditions, autism, physical handicap, eating disorders, and chronic somatic/physical diseases were excluded. The interventions had to be gross motor, energetic activity with minimum duration four weeks.
Two reviewers judged independently whether the studies fulfilled the inclusion criteria. If there was uncertainty or disagreement, a third reviewer was consulted.
Validity assessment
Two reviewers independently assigned these five quality criteria to each selected study:13
Concealment of allocation
Outcome assessment (assessor unaware of the assigned treatment when collecting outcome measures)
Co-intervention (interventions other than exercises avoided, or used similarly across comparison groups)
Losses to follow up
Intention to treat
Uncertainty or disagreement was resolved by discussion with the third reviewer. Studies were then grouped as studies with a low risk of bias (all criteria met), studies with a moderate risk of bias (three to four criteria met), and studies with a high risk of bias (fewer than three criteria met). As there is no clear evidence that some criteria are more important than others, they were given equal weight.
Data extraction and study characteristics
Each reviewer independently extracted data on population, age, baseline characteristics, characteristics of activity, compliance, and outcome measures. In cases of missing information, one author of the paper was contacted.
Quantitative data synthesis
Self esteem was measured with similar, but not identical, instruments across studies, and standardised mean differences (SMDs) and 95% confidence interval (CI) were calculated. The SMD expresses the size of the treatment effect in each trial relative to the variability observed in that trial.13 There was clinical heterogeneity between trials, with differences in study quality, the type or length of the intervention, and participant characteristics. Statistical heterogeneity was assessed using the χ2 test of heterogeneity along with a visual inspection of the graph. Such heterogeneity was identified. Overall effects were therefore calculated using a random effects model. When the primary studies provided several measures of self esteem, the overall self esteem score, often called global self esteem score in the papers, was used in the analysis. The effect sizes were translated back into clinically relevant values by using the 80 mm Piers-Harris children’s self-concept scale.14 On the basis of data from one of the included studies,15 we used standard deviation (SD) of 11 points for this calculation. To further enlighten the interpretation of the effect magnitude, we calculated the percentage difference between control and intervention groups by using the back translated Piers-Harris scores and post-treatment value in the control group as the basis.
To assess the robustness of conclusions as to quality of data and clinical heterogeneity, sensitivity analyses were performed according to levels of methodological quality, the type or length of the intervention, and participant characteristics. In the protocol we also specified age, sex, and compliance as potential important variables in the sensitivity analyses. However, because of limited information in the included studies, it was not possible to explore further the influence of these variables.
None of the included cluster randomised studies provided data on intra-cluster correlation and could therefore not be included in the meta-analyses. For these and other trials that did not provide sufficient data to calculate overall effects, a qualitative summary was provided.
RESULTS
Trial flow
We identified 7299 citations, retrieved 212 potentially relevant papers, and assessed 58 in detail (fig 1⇓). In the end, 23 were included.15–,37 The excluded studies were those not randomised, with short term interventions, no gross motor activity, or without self esteem as the outcome measure.

Selection of eligible randomised controlled trials (RCTs) from all identified citations.
Study characteristics
The included studies involved 24–288 participants aged 3–19.8 years. The participants were healthy, had learning disabilities and/or emotional disturbances, low self image, gross motor problems, or were young offenders. Most of the interventions lasted for 4–20 weeks, but one study had an intervention period of nine months.21 The interventions included aerobic, strength training, skills training, and combinations of these (tables 1⇓ and 2⇓). Two of the included studies25,28 compared two different interventions versus control, and the analysis therefore includes 25 comparisons.
Characteristics of randomised controlled trials comparing exercise as a single intervention with no intervention
Characteristics of randomised controlled trials comparing exercise as a part of a comprehensive intervention with no intervention
Outcomes were measured at the end of the interventions, and no further follow up results were given for any of the studies. There was variation in the quality of the studies (table 3⇓), and only one study met all five methodological criteria.16
Methodological quality of included studies
Synthesis of quantitative data
From a clinical point of view, the context in which the physical activity was carried out may be of importance to the outcomes. We therefore differentiated between studies that focused on exercise only and studies explicitly focusing on skill training, counselling, the social setting, or other motivational factors as a part of the exercise intervention.
Exercise as a single intervention versus no intervention
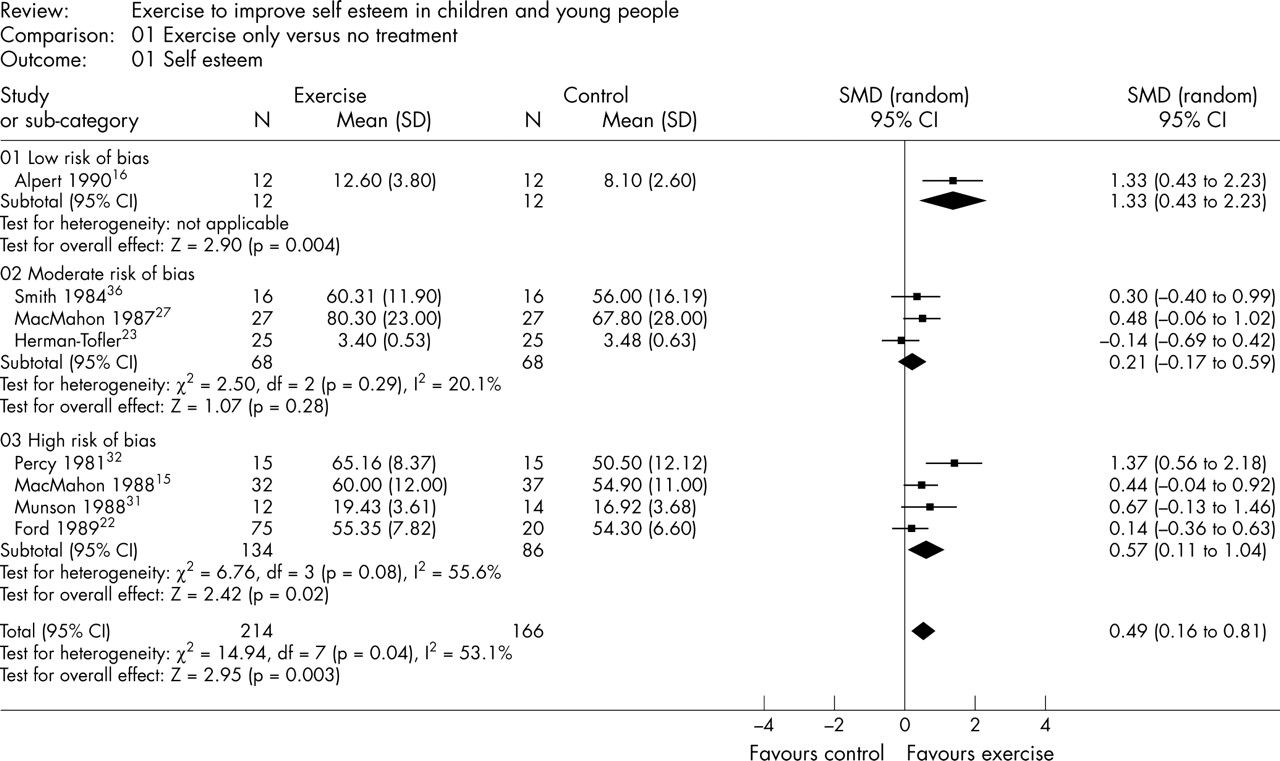
This comparison included 13 studies (table 1⇑) with eight in the meta-analysis (fig 2⇓). The overall SMD was 0.49 (95% CI 0.16 to 0.81) in favour of the exercise intervention. This corresponds to a difference of 5.4 points on a 0–80 scale, or about a 10% difference between the intervention and the control group. The subtotals for the study with a low risk of bias showed a SMD of 1.33 (95% CI 0.43 to 2.23), which corresponds to a difference of 14.6 points on the same scale.16 The studies with a moderate risk of bias showed a non-significant SMD of 0.21 (95% CI −0.17 to 0.59), and the studies with a high risk of bias had a SMD of 0.57 (95% CI 0.11 to 1.04). Five studies in this comparison were not included in the meta-analysis. Hilyer and Mitchell25 with high risk of bias found a significant improvement (p<0.01) for those with a low self concept at baseline. One study with a moderate risk of bias34 reported a significant effect (p = 0.05), whereas one with moderate risk of bias,37 and two with high risk of bias17,28 reported no significant effect.

Meta-analysis of studies comparing exercise as a single intervention with no intervention. SMD, Standardised mean difference; CI, confidence interval.
The sensitivity analysis showed that the effect size was not significant when the studies of healthy children were analysed separately. There were little or no differences when we analysed the results without the strength training studies or excluded the studies with interventions less than 10 weeks or with great baseline differences.
Exercise as a part of a comprehensive intervention versus no intervention
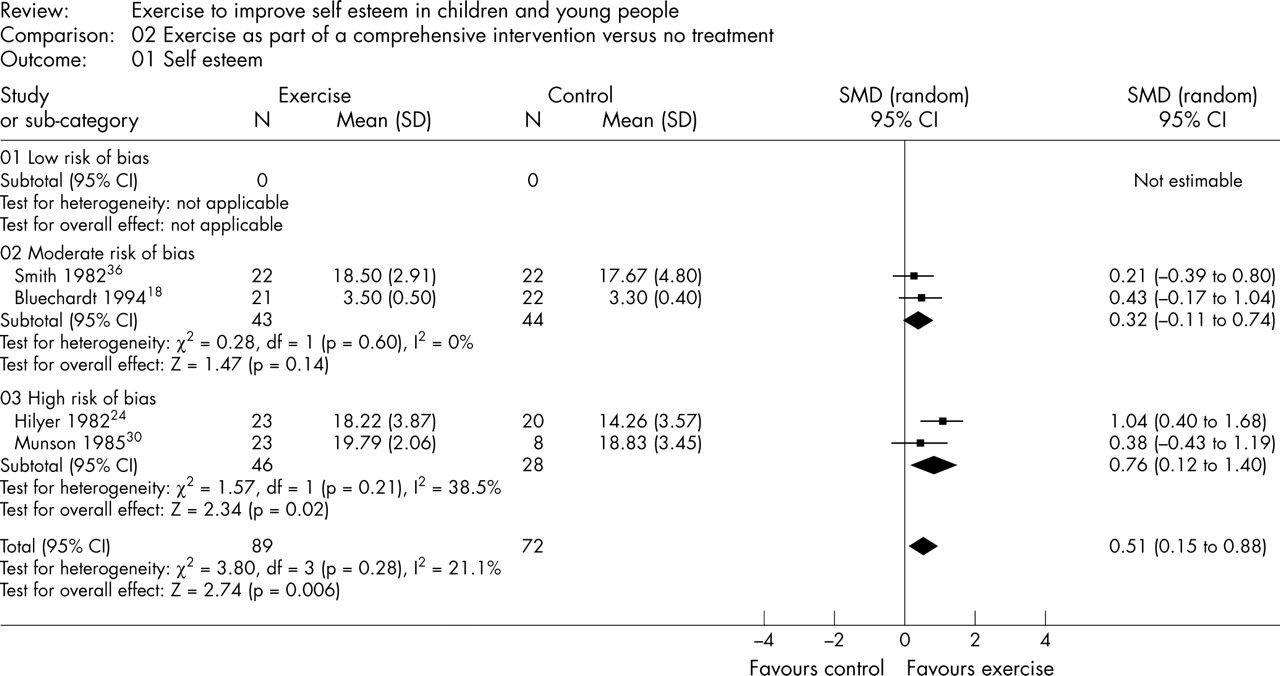
This group of interventions included 12 studies (table 2⇑), with only four in the meta-analysis (fig 3⇓). The results show an overall SMD of 0.51 (95% CI 0.15 to 0.88), which corresponds to a difference of 5.6 points on a 0–80 scale, or about a 10% difference between the intervention and the control group. No studies in this group had a low risk of bias, but in studies with a moderate risk of bias the SMD was non-significant at 0.32 (95% CI −0.11 to 0.74), and in those with a high risk of bias, the SMD was 0.76 (95% CI 0.12 to 1.40). Studies not included in the meta-analysis all had a high risk of bias. Four studies19,21,25,33 found a significant treatment effect, and four20,26,28,29 did not.

{kind=link}
{kind=link}
{kind=link}
Meta-analysis of studies comparing exercise as a part of a comprehensive intervention with no intervention. SMD, Standardised mean difference; CI, confidence interval.
In this comparison, it was not possible to categorise the interventions, and no studies had interventions less than 10 weeks. When the single study with healthy participants was excluded from the meta-analysis,35 the SMD increased to 0.64 (95% CI 0.22 to 1.06) which corresponds to a difference of 7.3 points on a scale from 0–80. When the study with obvious baseline differences in self esteem30 was excluded, there was no clear difference (SMD 0.55 (95% CI 0.07 to 1.03)).
DISCUSSION
The objective of this review was to determine if exercise interventions can improve self esteem in children and young people. The results, based on 25 comparisons with participants aged 3–20 years, indicate that exercise can improve self esteem. This compares well with the meta-analysis of Gruber.11
Only one of the included studies was assessed to have a low risk of bias, and eight were categorised as studies with a moderate risk of bias. The remaining 14 studies had a high risk of bias. With these different methodological weaknesses in the studies, the analyses were carried out by categorising studies into three quality levels. In addition, the studies are grouped into two main comparisons, one where the intervention focus was exercise only (13 studies) and one where the exercise was combined with skills training, counselling, or social aspects (12 studies).
Because of cluster randomisation or insufficient data to calculate effect sizes, meta-analysis could be carried out for only 12 studies, eight that looked at exercise only and four that looked at exercise combined with other aspects. Both of these meta-analyses show a small overall significant treatment effect, corresponding to a difference of 5.4 and 5.6 points on a 0–80 scale, or about a 10% difference between the intervention and the control group. Of the studies not included in the meta-analysis, seven showed a significant treatment effect and six did not.
Because of the clinical and statistical heterogeneity, we performed sensitivity analyses. The only change in SMD of any possible important value was an increase in total SMD when the studies with children at risk were analysed separately. The effect size changed only marginally when weight lifting results, intervention with duration shorter than 10 weeks, or studies with differences in baseline measures of self esteem were excluded from the analysis. This is consistent with findings in many types of interventions or preventive programmes.38
Self esteem was reported by the children themselves on instruments that are well accepted and reasonably well tested for reliability and validity, with the possible exception of one study, where the quality of the method is not known.33 There were no follow up data to show the extent to which the effects of programmes were maintained over longer periods of time, and none of the studies included factors indicating the degree of fun or enthusiasm among participants in the programmes. Whether the treatment effects were of clinical importance remains unclear. Some claims that a SMD of 0.5, in this case corresponding to a difference of self esteem of 5.5 on a 0–80 scale, is a moderate effect.39 Still the important question of whether children with a difference in self esteem such as this have a different degree of robustness and protection against psychological problems remains unanswered.
What is already known on this topic
There is a high incidence of mental problems among children and young people, and high self esteem may protect against such problems
However, the effect of exercise on self esteem is largely unknown
All the included studies used more or less “ordinary activity” as control treatment. The comparisons are therefore not between exercise and complete physical inactivity. This means that the possible treatment effect of exercise might be underestimated in this review. The effect was also somewhat surprising considering the short duration of the interventions. The research included in this review cannot tell us anything about what kind of exercise might give positive effects, and in which setting.
The results of this review are limited because of the small number of participants in the included studies and the lack of studies with a low risk of bias. Despite the methodological problems referred to, the results indicate that exercise may be effective in improving self esteem in children and young people, at least in the short term and for children and young people at risk. As exercise has no known negative effects, and many positive effects, on somatic health, it is an important instrument in improving children’s health.
This review reflects the need for rigorous research evaluating the effectiveness of exercise on children’s self esteem. The field should be further investigated by well designed randomised controlled trials. There is a need for follow up data to show the extent to which the effects of programmes are maintained over time.
What this study adds
Several low quality trials indicate that exercise has positive short term effects on self esteem in children and young people
This study highlights the need for well designed, randomised controlled trials with long term follow up
Acknowledgments
The study is partly funded by The Norwegian Fund for Post-Graduate Training in Physiotherapy. The researchers are independent from the fund.
REFERENCES
Commentary
It is useful to have a good quality systematic review to summarise the state of the evidence in this area. Low self esteem in children can lead to a range of psychosocial problems. In view of both the economic cost of other interventions (such as any kind of talking or play therapy) and the additional health benefits for children of taking more exercise, this is a useful intervention to consider. It is hoped that the call for more high quality randomised controlled trials to assess effectiveness will be taken up by research commissioners.
Footnotes
Competing interests: none declared