Article Text

Abstract
Background: Longstanding groin pain is a difficult diagnostic challenge for sports physicians, and the lack of consensus on diagnostic criteria and taxonomy makes comparison of published studies difficult.
Aim: To determine the usefulness and validity of the clinical classification proposed by Holmich et al in a primary care sports medicine population.
Design: Prospective cohort study.
Setting: Private sports medicine clinic in London, UK.
Participants: 218 consecutive cases presenting with longstanding groin pain.
Interventions: Clinical assessment, diagnostic investigations and follow-up.
Results: Groin pain patients (173 men, 45 women) presented from 23 sporting codes from professional athletes to the recreational exerciser. Men most commonly played soccer (football) (22%) and rugby (21%), while women were most often runners (40%). 12 month follow-up was successful in 65% of cases; an accurate diagnosis was made in 89% of cases. Hip pathology (50.4%) was the most common form of injury, with pubic pathology seen in 21% of cases. Pubic pathology was most often seen in kicking sports (58%), and straight line activities most often resulted in hip pathology (39%). Those patients diagnosed with hip pathology were less likely to return to pre-morbid levels of activity than those diagnosed with pubic pathology (28% vs 15%).
Conclusion: This series shows a different breakdown of injuries in a sporting population presenting with groin pain than previously reported. This reflects diagnostic difficulties in the area. The high incidence of hip pathology and the poor prognosis which this confers are worthy of note.
Statistics from Altmetric.com
Groin pain is a common complaint among the sporting population, accounting for between 5 and 15% of all football (soccer) related injuries.1 It is also commonly seen in Australian football,2 ice hockey,3 American football,4 and other sports where running, cutting, and kicking are part of the game.5–7
It is a difficult diagnostic challenge for sports physicians to diagnose, and, in part, this relates to the lack of agreement of diagnostic criteria and nomenclature.8–16 This is reflected in the fact that there are regional trends in which one country or region has a predominance of a certain diagnosis, whereas another region may show a statistical leaning towards another diagnosis.1 4 10 17–19
Based on prospective clinical series, a diagnostic categorisation has been proposed20 which separates groin pain into three broad groupings: (1) adductor related pain/osteitis pubis; (2) hernia and lower abdominal pain; and (3) iliopsoas related pain. There is also acknowledgement that approximately one third of groin pain patients had multiple clinical diagnoses. While potentially useful, this patient cohort was derived from presentations to a single orthopaedic surgeon with expertise in groin pain. Whether the concept is generalisable to other patient populations is unknown.
This study seeks to examine the usefulness of this diagnostic classification in a primary sports medicine setting.
METHODS
Subjects
A cohort of consecutive cases of groin pain presenting to a private sports medicine practice in London, England, between February 2004 and May 2006 were enrolled in the study. The subjects were either self-referred or referred for an opinion and management by physiotherapists, general practitioners, other sports physicians, and orthopaedic and general surgeons.
Study conditions
Subjects were studied in a standardised format by a single sports physician. A working diagnosis was recorded after the first consultation and diagnostic investigations ordered. Once the diagnosis was confirmed, the patient was referred for definitive management.
All patients who reported groin pain were included in the study. It is standard practice for patients of this private clinic, before their consultation, to consent to their data being used for research purposes. The patients were then contacted by email and phone to assess the outcome of the treatment between the months of February 2006 and March 2006 (average follow-up 17 months, minimum 8 months). A separate sports physician performed the follow-up using a standardised proforma. The patients were assessed as to their current or ongoing symptoms and their return to pre-morbid activity level.
Statistical analysis
Statistical analysis was performed using the SPSS software program (version 13). For the purposes of analysis, various categories were grouped during analysis. Diagnosis was categorised according to the primary site of the pathology; pubic pathology, hip pathology, and pathology of neurovascular and muscular structures. Sport was categorised according to the prime aetiological action involved such as kicking (soccer, rugby, Gaelic football), twisting (racquet sports, hockey, skiing, martial arts), and straight line (running, walking, swimming, triathlon). This manner of grouping activities represented an effort to differentiate between those sports which would (a) primarily load the adductors and pelvic stabilisers (kicking), (b) those where repetitive flexion at the femoro-acetabular joint might predispose to impingement (running, cycling), and (c) those which involved upper body torsion implicating activity of abdominals and pelvic stabilisers (hockey, racquet sports).15
RESULTS
Demographics
A total of 218 consecutive cases of groin injury were enrolled in the study. One hundred and seventy-three (79.4%) were male, and 45 (20.6%) were female. Median age in men was 32 years (11–73 years) and 35.5 years in women (21–77 years). Those attending represented 23 activities. Men most commonly played soccer 37 (22%) or rugby 36 (21%) followed by running 28 (16%). Women were most often runners (n = 18 (40%)) with gym activity the next most popular (n = 5). Nine patients reported no regular sporting activity. Table 1 gives details of the presentation demographics broken down by site of pathology. It was noted that there was significant delay to presentation, with 20/214 (10%) of patients having symptoms for more than 2 years before presentation.
Investigations
Diagnostic investigations were performed in 141/218 subjects. Magnetic resonance imaging was performed in 87 patients; 52 patients had local anaesthetic injections performed for both therapeutic and diagnostic purposes; two had ultrasounds; three had computed tomography (CT) scans; two had nerve conduction studies; one had an x ray only; and one had an isotope bone scan (some patients had more than one investigation).
Diagnoses
The initial clinical diagnosis is presented in fig 1. Pathology of the hip joint was the most common cause of groin pain diagnosed in 100 cases (45.9%), with 45 cases of osteitis pubis diagnosed (20.6%), and a combination of these conditions was recognised in 10 cases (4.6%).

In the 141 cases that had diagnostic investigations, the final diagnosis is shown in fig 2. The injury profile is similar to that of the main group shown in fig 1. Diagnosis was correct in 127/141 cases (89%). Hip pathology again featured prominently with acetabular labral pathology present in 27 cases; osteoarthritis and chondral injury present in 22 cases; and six patients were diagnosed with hip capsule pathology.

Analysis of diagnoses stratified by site and activity
Review of diagnoses when stratified by post-injury level of activity (fig 3) shows a similar distribution of pathologies in the group who had a good result compared to the whole group, with hip pathology, osteitis pubis, and a combination of the two accounting for 39.5%, 22%, and 3% of diagnoses, respectively. Though numbers are small, the group who failed to return to pre-morbid level of activity suffered from a far higher percentage of hip pathologies (59%).

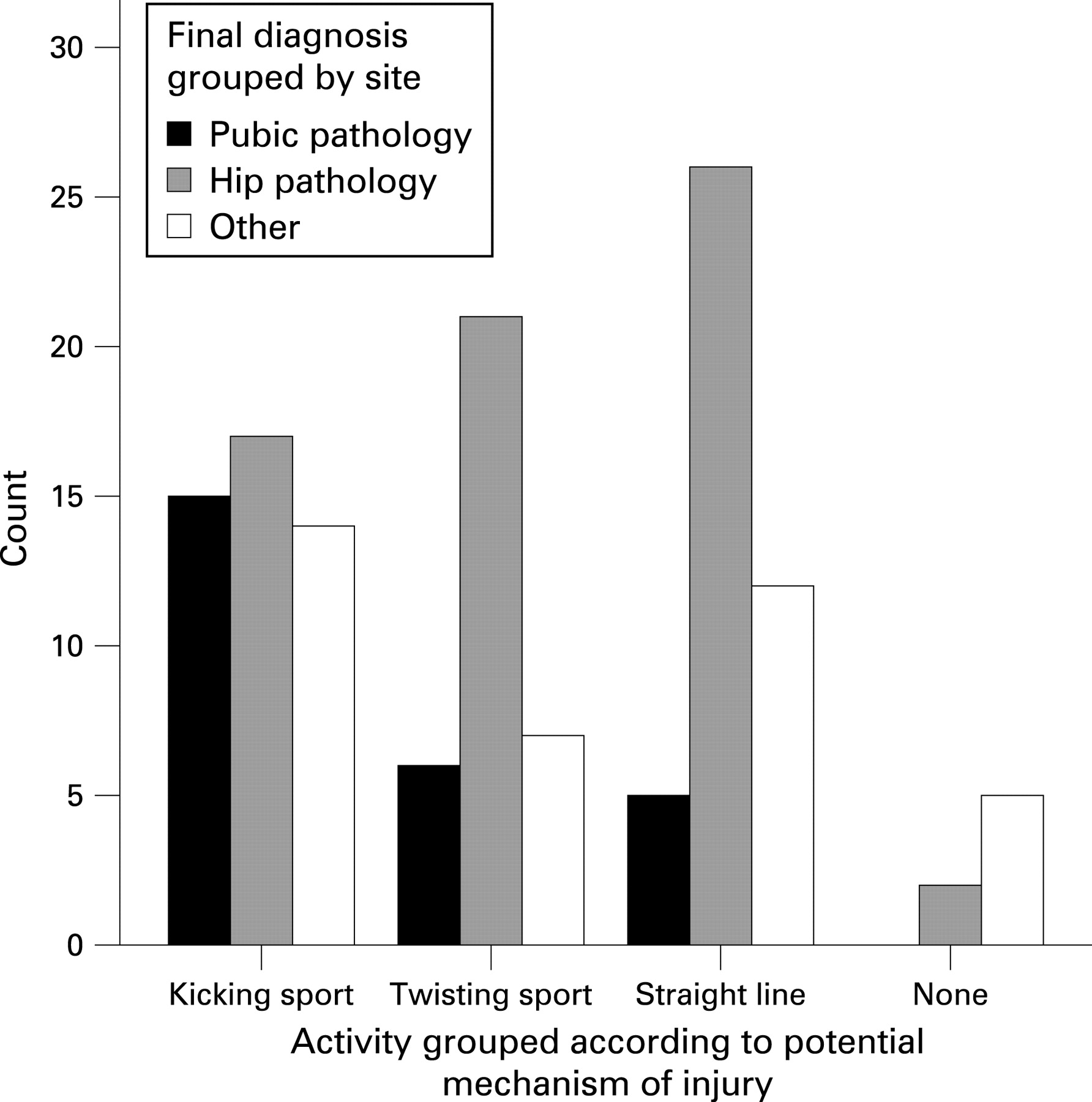
The sports played by those who failed to return to pre-morbid activity levels was similar to the main group, with running the most frequently seen (22.9%) followed by football (19.1%) and rugby (14.5%). A review of the confirmed pathologies when stratified according to sport is shown in fig 4. Fifty-seven per cent of all pubic pathology diagnosed occurred in patients involved in kicking sports. The pathologies were spread evenly in this category (pubic pathology n = 15, hip pathology n = 17, neurovascular and muscular n = 14). This was not seen in the other categories, with hip pathology causing 62% of twisting sport injuries and 61% of straight line running injuries—by far the dominant pathology (p<0.015).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Follow up
One hundred and forty-one patients (65%) were successfully contacted for follow-up at 12 months. Median length of follow-up was 17 months (4–35 months). Reasons for patients not being contacted included failure to reply to email/call (55 patients), change of address (11 patients), and incorrect contact details (eight patients). Three patients declined to be involved in the follow-up.
Of the 126 patients who reported on their return to activity post injury, 91 (72%) returned to their pre-morbid level of activity, 26 (21%) to a lower level, while eight were not active at all. Analysis of whether the site of injury had any bearing on this was not statistically significant. When looking at specific diagnoses, 84% of pubic pathology compared to 71.4% of hip pathology returned to pre-injury level of competition. In hip problems, with femoro-acetabular impingement and labral pathology, 19 of 26 (73%) returned to full activity, while only 12 of 21 (57%) of those with osteochondral damage retained their activity level, and five of six of those with capsular issues regained full activity. All stress fractures returned to full activity (n = 12).
DISCUSSION
The current study demonstrated that in a population of groin pain subjects presenting to a primary care sports medicine clinic, the most prevalent condition was hip joint pathology. Common diagnoses included acute labral tears and impingement syndromes, with cam impingements outnumbering the pincer impingements.21 In the follow-up cohort, those who suffered hip pathologies tended to present later and were over represented in the group of patients who had failed to return to their pre-injury level of activity. This was particularly true of osteochondral injury. Hip injury was very common in straight line activities and also what we termed twisting activities, such as racquet sports and hockey. Of the patients with a primary diagnosis of osteitis pubis, none were female, and their overall management was dictated by whether they exhibited a predominantly bony presentation, a predominantly degenerative presentation, or a predominantly inflammatory presentation. Eight patients, all male, were deemed to have coexisting hip joint pathology and osteitis pubis. The absence of any female patients with the diagnosis of osteitis pubis is interesting. We recognise that post-partum mothers with true pubic symphysis instability exhibit signs of osteitis pubis and can be difficult to treat. However, none were seen in this patient population.22
Overall, there appears to be an overwhelming bias towards male patients with the diagnosis of osteitis pubis of all sub-categories. It is obvious that many female athletes play sports, such as soccer, which involve twisting and turning and kicking. It therefore follows that there may be anatomical differences in the female pelvis which is protective against pubic stress when compared with the pelvic anatomy of their male counterparts. The obvious difference is the patency of the inguinal canal in males. It is probably therefore not surprising that male patients, seemingly with a clinical diagnosis of osteitis pubis, can be significantly improved by some form of inguinal repair surgery—“tightening” the inguinal canal.18
In this series, there were no patients diagnosed with either “sportsman’s hernia”23 or conjoint tendon pathology.24 Likewise, no true inguinal hernias were seen. This may reflect referral bias in this geographic setting. There were a number of cases of obturator neuropathy reported, comprising roughly 6% of cases followed up. The prevalence of this condition is consistent with the published literature on this topic.8 25 It is thought that these cases are a subset of those with osteitis pubis, and that the fascial dysfunction is very important. This series had a large number of femoral neck stress fractures. This may have been because the study was conducted over a time period that spanned three London marathons.
There were also a number of interesting causes of groin pain, including one case of external iliac artery endofibrosis that presented with exercise related adductor pain, and a case of stress fracture of the acetabulum in a young soccer player. The authors recognise that groin pain as a clinical problem has varied presentations and aetiology. A systematic approach to the diagnosis of groin pain will be presented in a future paper.
In the orthopaedic classification of groin pain proposed by Holmich et al,20 it was noted that 58% of cases were adductor related, 35% were iliopsoas related, and 7% were “other” clinical entities. This differs notably from the findings in this study and reflects both the taxonomic difficulties in the diagnosis of chronic groin pain, but more importantly the huge variation in presentation depending on the referral source of the published study. While it is understandable that an orthopaedic specialist would more likely be referred conditions amenable to definitive orthopaedic intervention, the breakdown of cases in the published study is likely to reflect this bias. Our paper, however, is in the setting of a primary care sports medicine clinic that explains the different case mix of patients.
Summary
This study demonstrates the different pathological diagnoses that may present as chronic groin pain and, more importantly, highlights both the high prevalence of hip joint related pathology in this setting and the relatively poor prognosis of these entities in the likelihood of return to sport.
REFERENCES
Footnotes
Competing interests: None.
Patient consent: Obtained.