Article Text

Abstract
The objective of the present systematic review was to investigate whether physical fitness in childhood and adolescence is a predictor of cardiovascular disease (CVD) risk factors, events and syndromes, quality of life and low back pain later in life. Physical fitness-related components were: cardiorespiratory fitness, musculoskeletal fitness, motor fitness and body composition. Adiposity was considered as both exposure and outcome. The results of 42 studies reporting the predictive validity of health-related physical fitness for CVD risk factors, events and syndromes as well as the results of five studies reporting the predictive validity of physical fitness for low back pain in children and adolescents were summarised. Strong evidence was found indicating that higher levels of cardiorespiratory fitness in childhood and adolescence are associated with a healthier cardiovascular profile later in life. Muscular strength improvements from childhood to adolescence are negatively associated with changes in overall adiposity. A healthier body composition in childhood and adolescence is associated with a healthier cardiovascular profile later in life and with a lower risk of death. The evidence was moderate for the association between changes in cardiorespiratory fitness and CVD risk factors, and between cardiorespiratory fitness and the risk of developing the metabolic syndrome and arterial stiffness. Moderate evidence on the lack of a relationship between body composition and low back pain was found. Due to a limited number of studies, inconclusive evidence emerged for a relationship between muscular strength or motor fitness and CVD risk factors, and between flexibility and low back pain.
Statistics from Altmetric.com
Cardiovascular disease (CVD) is the leading cause of global mortality.1 CVD events occur most frequently during or after the fifth decade of life; however, there is evidence indicating that the precursors of CVD have their origin in childhood and adolescence.2 3 Adverse CVD risk factors during childhood seem to track into adulthood.4 5 The most recognised CVD risk factors are obesity, high levels of triglycerides and blood cholesterol, insulin resistance, inflammatory proteins, high blood pressure, physical inactivity and low physical fitness.
Musculoskeletal problems and conditions are common and have important consequences for both the individual and society. Approximately 50% of the population report musculoskeletal pain at one or more sites in the past month,6 and the figures for young people are similar.6 Population surveys reported that back pain is the most common site of regional pain in young people and middle-aged adults. In adolescents, the lifetime prevalence of low back pain ranges from 7% to 72%.6
Quality of life refers to the degree of wellbeing felt by an individual or group of people. Quality of life has a physical component that includes aspects such as health, diet, as well as protection against pain and disease. It also has a psychological component that includes aspects related to stress, worries, pleasure and other positive or negative emotional states. Several cross-sectional studies have reported an association between fitness and wellbeing in youth.7 8 9 10
Whether physical fitness is an important marker of health already in childhood and adolescence is still under debate,11 12 13 because most of the evidence comes from cross-sectional studies. In the past few decades, several longitudinal studies in children and adolescents reported on the relationship between physical fitness-related exposures and the risk of developing an unhealthy cardiovascular or musculoskeletal profile later in life. Understanding whether low/high physical fitness in young people is a predictor of future disease/better health status would clarify the debate as to whether physical fitness should or should not be assessed in health monitoring systems.
The objective of the present systematic review was to investigate whether physical fitness in childhood and adolescence is a predictor of CVD risk factors, type 2 diabetes, metabolic syndrome and cardiovascular events later in life. We also examined whether there is evidence that physical fitness in childhood and adolescence is a predictor of quality of life and low back pain later in life.
Methods
The present systematic review is produced as a part of the ALPHA (instruments for Assessing Levels of PHysical Activity and fitness) study. The ALPHA study aims to provide a set of instruments for assessing levels of physical activity as well as health-related physical fitness in a comparable way within the European Union.
Selected health outcomes
Based on recent knowledge of major health problems and their risk factors, several health outcomes were selected to seek evidence for associations between physical fitness and health status in children and adolescents.
The main question was “does low/high fitness in youth predict future disease/better health status? We selected longitudinal cohort studies examining the association between physical fitness in children and adolescents and future: (1) CVD risk factors: blood lipids, blood pressure, insulin sensitivity, inflammatory markers and overall and central adiposity; (2) CVD/syndromes: obesity, hypertension, dyslipidaemia, diabetes and the metabolic syndrome; (3) low back pain; (4) quality of life and wellbeing, also called positive health outcomes: school performance, self-esteem, mood status, socialisation, resilience (ie, the positive capacity of people to cope with stress) and risk-avoidance behaviour.
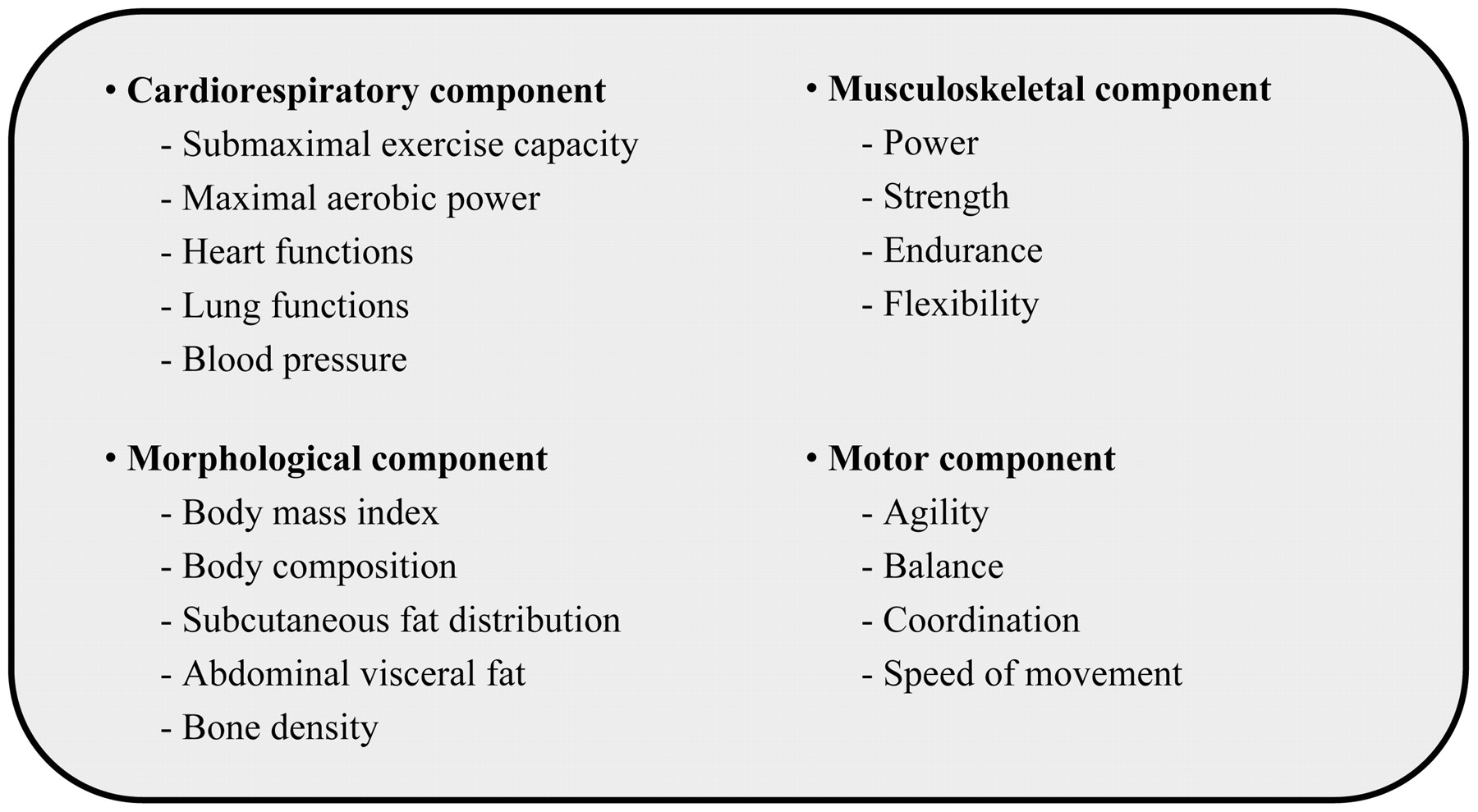
The health-related fitness components and factors/traits are depicted in fig 1.14 Definitions of the concepts used in the manuscript can be seen in the supplemental material (available online only).
{kind=link}
Health-related fitness components and factors/traits. Modified from Bouchard et al14 with permission.
Procedures
The electronic databases MEDLINE, EMBASE, SCOPUS and SPORTS DISCUS were screened for longitudinal studies (either prospective or retrospective cohort studies) in children and adolescents in which one or more fitness tests were carried out, and the outcome measured was one of the selected health outcomes.
The key words used (in various combination) were: physical fitness, fitness, aerobic capacity, maximum oxygen consumption, cardiorespiratory fitness, cardiovascular fitness, strength, flexibility, motor, endurance, speed, agility, balance, body composition, anthropometry, body mass index (BMI), waist circumference, overall adiposity, central adiposity, overweight, obesity, risk factors, risk score CVD, metabolic syndrome, blood glucose, glucose tolerance, insulin resistance, insulin sensitivity, blood lipids, dyslipidaemia, diabetes, blood pressure, hypertension, inflammatory markers, bone mineral density, bone mineral content, school performance, self-esteem, mood status, socialisation, resilience, risk avoidance behaviour, mental health and low back pain.
Search limits were: papers published from January 1990 to July 2008, written in English, in “humans” and “all child” (0–18 years). An additional search using adolescents (13–18 years) was also performed. There were no exclusion criteria with regard to ethnic origin. Additional studies were indentified from reference lists.
The abstracts of longitudinal studies proposed to be included in the review were checked for the following criteria: (1) the study was a full report published in a peer-reviewed journal; (2) the study design was a longitudinal study; (3) the study population was a healthy community-based population; (4) one or more fitness tests were carried out; (5) the outcome measure was one of the selected health outcomes. Articles were included if they met all these five criteria. Two independent reviewers (JRR, JCP) read all the abstracts, and a consensus meeting was arranged to sort out differences between both of them.
The results of the most recent reviews were summarised first, and then the studies potentially relevant for the selected topics were screened for retrieval. Finally, a snowball search was done, in which reference lists of the selected articles were checked for titles including physical fitness and selected health outcomes.
Quality assessment
The quality of the selected studies was scored using a quality assessment list for longitudinal studies.15 The list included five items on population, designs, methods and report of the results. The items on the list were rated as “1” (positive), “0” (negative) or “?” (unclear), see table 1. For all studies, a total quality score was calculated by counting up the number of positive items (a total score between 0 and 5). Studies were defined as high quality if they had a total score of 3 or higher. A total score of 2 was defined as low quality, and a score of less than 2 was defined as very low quality. Two reviewers (JRR and JCP) separately evaluated the quality of the studies. A consensus meeting was arranged to sort out differences between both reviewers. The articles were not blinded for authors, institution and journal, because the reviewers who performed the quality assessment were familiar with the literature.
Quality assessment list for prospective cohort studies
Levels of evidence
Three levels of evidence were constructed:16 (1) strong evidence: consistent findings in three or more high-quality studies; (2) moderate evidence: consistent findings in two high-quality studies; (3) limited or conflicting evidence: consistent findings in multiple low-quality studies, inconsistent results found in multiple high-quality studies, or results based on one single study.
Data extraction
Information on design, statistical procedures, population characteristics, years of follow-up, fitness tests, outcome and risk estimates and main results was extracted from all studies. Data extraction was separated for CVD risk factors, low back pain and for quality of life. We regarded results with a p⩽0.05 as statistically significant.
Results
Health-related physical fitness predictive validity for CVD risk factors and disease
A total of 42 longitudinal studies was included (table 2). Cardiorespiratory fitness was assessed in 20 (48%) studies, musculoskeletal fitness was assessed in eight (19%), motor fitness in three (7%) and body composition in 21 studies (50%). One study examined the association between perceived physical fitness and weight gain from adolescence to early adulthood.17
List of included longitudinal studies with quality scores with reference to predictive value of physical fitness for CVD risk factors and disease in children and adolescents
Quality assessment
Table 2 shows the list of included longitudinal studies with quality scores. The overall agreement between the two reviewers was 90% (κ = 0.809). Disagreement was solved in a consensus meeting. We defined 33 studies as high quality (score ⩾3) and four as low quality (score 2). There were no studies with a quality score below 2. A total of 21 studies had the highest score (score 5), from which seven dealt with cardiorespiratory fitness, one with motor and musculoskeletal fitness and 15 with body composition.
Levels of evidence
Table 3 shows the results of the data extraction of the studies reporting the predictive validity of health-related physical fitness for CVD risk factors and disease in children and adolescents.
Longitudinal studies on predictive validity of physical fitness for CVD risk factors and disease in children and adolescents
Cardiorespiratory fitness
Seventeen high-quality studies18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 reported on the prospective relationship between cardiorespiratory fitness and CVD risk factors and disease in children and adolescents. Several studies reported that cardiorespiratory fitness in childhood and adolescence is a predictor of CVD risk factors, such as abnormal blood lipids,18 19 20 24 25 28 29 30 31 33 high blood pressure,18 20 30 35 and excess of overall and central adiposity18 19 20 21 24 25 28 29 34 36 later in life. Two studies reported that cardiorespiratory fitness in childhood and adolescence is a predictor of the metabolic syndrome30 33 and arterial stiffness26 31 later in life. Two studies examined the association between changes in cardiorespiratory fitness and changes in CVD risk factors, such as total cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides and total and central adiposity.18 25 One study examined the association between changes in cardiorespiratory fitness and changes in intima media thickness (IMT), carotid distension and compliance,31 and Carnethon et al30 studied the relationship between changes in cardiorespiratory fitness and diabetes, metabolic syndrome and weight gain over 7 and 15 years.
Carnethon et al30 reported that adolescents with low cardiorespiratory fitness (<20th percentile) were three to sixfold more likely to develop the metabolic syndrome as well as to develop diabetes and hypertension than adolescents with high cardiorespiratory fitness (⩾60th percentile; all p<0.001). They also reported that improved cardiorespiratory fitness over 7 years was associated with a reduced risk of developing the metabolic syndrome (hazard ratio (HR) 0.5; 95% CI 0.3 to 0.7; p<0.001) and diabetes (HR 0.4; 95% CI 0.2 to 1.0; p = 0.04) but the strength and significance of these associations was reduced after accounting for changes in body weight. Furthermore, they reported that among those who became obese earlier in life (possibly during childhood or adolescence), cardiorespiratory fitness did not protect against developing diabetes or the metabolic syndrome. Increasing cardiorespiratory fitness between visits was associated with a lower risk of developing both diabetes and the metabolic syndrome, suggesting that two very important risk factors for coronary heart disease and mortality may be modified by improving fitness over time.30
Overall, these findings are consistent for both boys and girls, although there is one high-quality study showing that cardiorespiratory fitness was not a significant predictor of change in body fat after controlling for changes in pubertal status, lean tissue mass and age in girls (β = 0.0005, p = 0.37).34 There is also one high-quality study showing that cardiorespiratory fitness at the age of 16 years is not associated with markers of overall and central adiposity, HDL cholesterol, or systolic blood pressure at the age of 34 years.23
Results from low-quality studies are consistent with those observed in high-quality studies, except the study by McGavock et al37 (low-quality study), which reported that cardiorespiratory fitness is not associated with changes in systolic blood pressure.
In summary, there is strong evidence indicating that cardiorespiratory fitness in childhood and adolescence is a predictor of CVD risk factors such as abnormal blood lipids, high blood pressure and overall and central adiposity later in life. There is moderate evidence indicating that cardiorespiratory fitness in childhood and adolescence is a predictor of the metabolic syndrome and arterial stiffness later in life. Finally, there is moderate evidence indicating that changes in cardiorespiratory fitness are associated with CVD risk factors. Due to a limited number of studies (one for each outcome), there is inconclusive evidence indicating that changes in cardiorespiratory fitness are associated with changes in IMT, carotid distension and compliance, weight gain, diabetes and the metabolic syndrome.
Musculoskeletal fitness
Four high-quality studies,18 23 25 28 and one low-quality study38 reported on the prospective relationship between musculoskeletal fitness and CVD risk factors and disease in children and adolescents. Changes in muscular strength from childhood to adolescence seem to be negatively associated with changes in overall adiposity,18 23 25 28 whereas the association between changes in muscular strength and changes in central adiposity are less evident.18 25 Janz et al25 reported that changes in muscular strength were negatively associated with changes in systolic blood pressure (p<0.05) after controlling for age, gender, fat-free mass and pubertal status in both boys and girls, whereas no associations between changes in muscular strength and changes in blood pressure, total cholesterol, HDL or triglycerides were observed in Danish youth.18
In summary, there is strong evidence indicating that muscular strength changes from childhood to adolescence are negatively associated with changes in overall adiposity, whereas there is moderate evidence indicating such an association for central adiposity. There is inconclusive evidence that muscular strength changes are associated with changes in other CVD risk factor such as systolic blood pressure or blood lipids and lipoproteins.
Motor fitness
There is one high-quality study28 and one low-quality study38 reporting the prospective relationship between motor fitness and CVD risk factors in children and adolescents. Twisk et al28 computed an index of neuromotor fitness with measures of muscular strength, flexibility, speed of movement and coordination, and they reported that neuromotor fitness was positively related to systolic blood pressure (β = 0.11; p<0.01) and inversely to the sum of four skinfolds (β = 0.21; p<0.01). They also reported that neuromotor fitness was not associated with total cholesterol, HDL cholesterol, or the ratio of both.
In summary, there is inconclusive evidence indicating that motor fitness in childhood and adolescence is a predictor of CVD risk factors later in life.
Body composition
There are 14 high-quality studies,4 21 22 33 39 40 41 42 43 44 45 46 47 48 and three low-quality studies37 49 50 reporting the prospective relationship between body composition and CVD risk factors and disease in children and adolescents. Several studies reported that body composition in childhood and adolescence is a predictor of CVD risk factors, such as blood lipids22 39 42 and carotid artery IMT.4 40 41 47 Garnett et al39 reported that children who were overweight or obese at 8 years of age were seven times (odds ratio (OR) 6.9; 95% CI 2.5 to 19.0; p<0.001) as likely to have CVD risk clustering in adolescence as were their peers who were not overweight or obese. They also reported that those with an increased central adiposity (measured with waist circumference) at the age of 8 years were four times (95% CI 3.6; 1.0 to 12.9; p = 0.061) as likely to have CVD risk clustering in adolescence as were children with a smaller waist circumference.
Several high-quality studies51 52 53 54 reported an increased risk of death in those individuals with higher BMI in adolescence. Mortality among men whose baseline BMI was between the 85th and 95th percentiles and above the 95th percentile in the US reference population was 30% and 80% higher, respectively, than that among those whose baseline BMI was between the 25th and 75th percentiles. The corresponding rates among women were 30% and 100%.54 Findings from the same cohort revealed that higher BMI at adolescence was associated with an increased relative risk of death from endocrine, nutritional and metabolic diseases, and from diseases of the circulatory system.53 These findings apply to both boys and girls. Must et al52 reported that overweight in adolescents was associated with an increased risk of mortality from all causes and disease-specific mortality among men. The relative risks among men were 1.8 (95% CI 1.2 to 2.7; p = 0.004) for mortality from all causes and 2.3 (95% CI 1.4 to 4.1; p = 0.002) for mortality from coronary heart disease. They also reported that the risk of morbidity from coronary heart disease and atherosclerosis was increased among men and women who had been overweight in adolescence.
In summary, there is strong evidence indicating that body composition in childhood and adolescence is a predictor of CVD risk factors such as blood lipids and carotid artery IMT. There is also strong evidence indicating that high BMI in childhood and adolescence increases the risk of death later in life.
Health-related physical fitness predictive validity for low back pain
A total of five longitudinal studies were included (table 4). Musculoskeletal fitness was assessed in four studies and body composition in two studies. There were no studies examining the prospective association between cardiorespiratory or motor fitness and low back pain.
List of included prospective cohort studies with quality scores with reference to predictive value of physical fitness for low back pain in children and adolescents
Quality assessment
Table 4 shows the list of included longitudinal cohort studies with quality scores. The overall agreement between the two reviewers was 100% (κ = 1). We defined five studies as high quality (score ⩾3). One study had a score of 3,55 two studies had a score of 4,56 57 and two studies had the maximum score, that is 5.58 59 There were no studies with a score below 3.
Levels of evidence
Table 5 shows the results of the data extraction of the studies reporting the predictive validity of physical fitness for low back pain in children and adolescents.
Prospective studies on predictive validity of physical fitness for low back pain in children and adolescents
Musculoskeletal fitness
Four high-quality studies reported on the prospective relationship between musculoskeletal fitness and low back pain in children and adolescents, with inconsistent results.55 56 57 60
Kujala et al55 reported that tightness of the hip flexor muscles was associated with lifetime cumulative incidence of low back pain, whereas Burton et al57 reported that lumbar sagittal flexibility was not associated with self-reported low back pain. Likewise, Barnekow-Bergkvist et al56 did not observe an association between flexibility and low back pain except for the back extension test, which was negatively associated with low back symptoms in women. Only one study reported that muscular strength, measured by the two-hand lift test at the age of 16 years, was associated with a significantly decreased risk of low back problems in adulthood in women.56
In summary, there is inconclusive evidence indicating that flexibility or muscular strength in childhood and adolescence is a predictor of low back pain later in life.
Body composition
Two high-quality59 60 studies reported on the prospective relationship between body composition and low back pain in children and adolescents. BMI was the only component available in these studies. Mikkelsson et al60 did not observe an association between BMI and low back pain in either boys or girls. Likewise, Hestbaek et al59 reported that adolescent overweight was not associated with adult low back pain.
In summary, the findings indicate that there is no association between BMI and low back pain, and the evidence is moderate.
Health-related physical fitness predictive validity for quality of life and wellbeing
We were not able to find any longitudinal study reporting on the associations between physical fitness and quality of life in children and adolescents. One longitudinal study explored the links between participation in physical activity and global self-esteem among girls from childhood into early adolescence.61 They reported that participating in physical activity can lead to positive self-esteem among adolescent girls, particularly for younger girls and those at greatest risk of overweight. Knowing the association between physical activity and cardiorespiratory fitness in children and adolescents,62 63 64 we could presume that high levels cardiorespiratory fitness during childhood might be a predictor of positive self-esteem later in life. This issue warrants further investigation.
Discussion
The present systematic review shows that there is strong evidence indicating that: (1) higher levels of cardiorespiratory fitness in childhood and adolescence are associated with a healthier cardiovascular profile later in life; (2) muscular strength improvements from childhood to adolescence are inversely associated with changes in overall adiposity; and (3) a healthier body composition in childhood and adolescence is associated with a healthier cardiovascular profile and a lower risk of death later in life.
We have also shown that there is moderate evidence indicating that: (1) higher levels of cardiorespiratory fitness in childhood and adolescence reduce the risk of developing the metabolic syndrome and arterial stiffness later in life; (2) increasing cardiorespiratory fitness is inversely associated with changes in blood lipids and lipoproteins; (3) muscular strength improvements from childhood to adolescence are inversely associated with changes in central adiposity; and (4) there is no association between body composition (ie, BMI) and low back pain.
Finally, due to a limited number of studies, the results also suggest that there is inconclusive evidence showing that: (1) changes in cardiorespiratory fitness are associated with changes in IMT, carotid distension and compliance, weight gain, diabetes and the metabolic syndrome; (2) changes in muscular strength are associated with changes in systolic blood pressure or blood lipids and lipoproteins; (3) motor fitness in childhood and adolescence is a predictor of CVD risk factors later in life; and (4) motor fitness in childhood and adolescence is a predictor of low back pain later in life.
Heterogeneity
The results of the present systematic review should be interpreted with caution due to the variety of tests used to assess physical fitness, the outcomes measures, follow-up time (from one year to 57 years), age of the participants and adjustment for confounders.
Physical fitness tests
Cardiorespiratory fitness was assessed by means of six different tests: 20 m shuttle run test,21 29 32 37 1.5 mile run/walk test,23 maximal treadmill test,19 24 28 30 31 33 34 49 maximal25 and submaximal18 20 26 27 cycle ergometer test and the 1600 m run test.38 The outcome of the tests was also expressed in different ways: measured maximum oxygen consumption (Vo2max),18 19 20 24 25 28 31 33 34 estimated Vo2max,23 26 27 32 duration of the test30 38 49 and number of completed laps in the 20 m shuttle run test.21 29 Finally, Vo2max was expressed in absolute terms (l/minute),20 24 28 31 34 or in relative terms as ml/kg per minute,18 20 23 26 28 31 32 33 37 as ml/minute per kg of fat-free mass27 or as ml/minute per kg2/3.19 25 31
Musculoskeletal fitness was assessed by the handgrip strength test,19 28 38 55 bent arm hang,38 bench press,19 56 standing broad jump,38 sit-ups,19 38 curl-ups,55 sit and reach28 38 55 56 and the shoulder stretch test.38
Motor fitness was assessed by the 4 × 10 m shuttle run test,19 28 38 the 50 m run test19 28 38 and the standing balance test.56
Body composition was mainly assessed by BMI,4 22 33 39 41 43 44 45 46 47 48 49 50 51 52 53 54 60 yet several studies also included measures on skinfold thickness,22 33 40 42 50 55 and waist circumference.33 39 48 49
What is already known on this topic
Physical fitness is emerging as an important marker of health already in childhood and adolescence, yet most of the evidence comes from cross-sectional studies.
What this study adds
There is evidence coming from longitudinal studies that a higher level of physical fitness (ie, cardiorespiratory fitness, muscular strength and body composition) in childhood and adolescence is associated with a healthier cardiovascular profile and with a lower risk of developing CVD later in life.
A healthier body composition in childhood and adolescence is also associated with a lower risk of death in adulthood.
Improvements in physical fitness from childhood to adulthood are associated with positive changes in CVD risk factors.
Outcome measures
Most of the studies used single and continuous CVD risk factors, such as blood lipids, blood pressure, insulin sensitivity, inflammatory markers, or overall and central adiposity, whereas others gave clear details of the presence of the disease/syndrome (eg, obesity, hypertension, dyslipidaemia, diabetes, or the metabolic syndrome). In the studies related to low back pain, the outcome was dichotomous, as the presence or absence of low back pain, which was self-reported.
Follow-up
The follow-up time of the selected studies ranged from one to 5 years,17 21 24 25 32 34 37 38 44 55 57 to more than 5 years,18 20 27 39 48 more than 10 years,22 23 29 30 43 46 47 49 56 more than 20 years,4 28 31 33 40 41 42 45 50 60 more than 30 years53 54 and more than 50 years.51 One study followed the participants for 60 years.52 The longest studies are those investigating the prospective association between BMI and the risk of death.51 52 53 54
Adjustment for confounders
Most of the studies adjusted for confounders, whereas several studies did not adjust for any confounder.17 18 19 20 21 22 27 37 38 39 49 50 Not adjusting for potential confounders such as sex (if applicable), age, pubertal status, baseline health status or socioeconomic status, could lead to a different results, that is, to an under or an overestimation of the findings. The overall findings of the present systematic review would not have materially changed if we had restricted the analyses to those studies with satisfactory adjustment for potential confounders.
Quality assessment
The cut-off points and assumptions established to define the levels of evidence might have influenced the results. To investigate the influence of these cut-offs on the findings, we performed sensitivity analyses after varying those assumptions. Due to the limited number of studies, this was not performed on the low back pain studies.
We calculated total quality score by counting up the number of positive items. All the items had the same weight, despite the fact that some items might be more relevant for the quality assessment than others. The quality items on the time between the measurement of physical fitness test and the health outcome, adjustment for confounders and standard errors and/or confidence intervals might be more important for the level of evidence than the items on the selection of the population or the description of the health outcomes.
We gave to those more relevant items a double weight, that is, we multiplied them by 2, which led to a maximum total score of 8. We defined studies as high quality if they had a total score of 6 or higher, and we defined studies as low quality if the total score was between 4 and 5. This would have excluded from the high-quality list the studies by Andersen et al,20 Hasselstrom et al,18 Psarra et al,21 Twisk et al19 and Srinivasan et al.22 However, this would not have affected the overall conclusions.
Changing the cut-off points regarding the qualification of studies as high or low quality would have also affected the number of high-quality studies. We changed the cut-off points needed to score a study as high quality from a total score of 3 to a score of 4. Five studies18 19 20 21 22 would have been excluded, yet this would not have changed the overall conclusions.
Overall, the conclusions do not materially change after modifying the cut-off points and assumptions used to rank the longitudinal studies. Therefore, the findings of this systematic review can be considered stable and robust.
Implications
These epidemiological observations should inform experimental/mechanistic studies the exploration of biological mechanisms that link physical fitness in children and adolescents with health/disease/death later in life. We still need further studies to know whether effective interventions to improve physical fitness in the first decades of life will reduce the burden of CVD-related morbidities and mortality later in life. This knowledge will also allow the formulation of public health strategies to prevent obesity-related morbidities worldwide.
Acknowledgments
The authors would like to thank Professors Willem van Mechelen, Pekka Oja, Han CG Kemper, Kari Bo and Jorge Mota for their valuable contribution to the conception and strategy of the review.
REFERENCES
Footnotes
Additional material is published online only at http://bjsm.bmj.com/content/vol43/issue12
Funding This work was supported by the European Union, in the framework of the Public Health Programme (ALPHA project, ref 2006120), the Swedish Council for Working Life and Social Research (FAS) and the Spanish Ministry of Education (EX-2007-1124, AP-2004-2745 and AP2005-4358).
Competing interests None.
Contributors JRR drafted the manuscript. JRR and JC-P read all the manuscripts and scored each of them. JRR and JS contributed to the concept and design of the systematic review. All the authors contributed to the interpretation and discussion of the results. JRR, JS, MS and MJC contributed to the concept and design of the ALPHA study. All the authors critically revised the manuscript.