Article Text

Abstract
Objective: To characterise Achilles tendon structure and thickness a minimum of 8 years after intratendinous surgery.
Material and Methods: Fourteen patients (16 tendons; nine men and five women, mean age 43 years, range 27–55) surgically treated (intratendinous surgery) for chronic painful midportion Achilles tendinosis, were followed with clinical examination and grey-scale ultrasonography for a minimum of 8 years (range 8–16, mean 13).
Results: All patients were satisfied with the result of surgery and were active in Achilles tendon loading activities without restrictions. In all operated tendons, structural abnormalities remained and tendons remained thicker than normal tendons.
Conclusions: Resection of tendinosis is associated with persistent structural abnormalities and thickening of the tendon 13 years after surgery, despite successful clinical outcomes.
Statistics from Altmetric.com
For many years intratendinous resection of macroscopically abnormal tendon tissue was the treatment of choice for patients with midportion Achilles tendinosis that did not respond to conservative treatment.1 2 3 4 5 The results of those operations varied. A critical review concluded that scientifically poor studies often showed good clinical results, whereas scientifically good studies often showed poor clinical results.6 At our clinic in the 1990s, surgical treatment for midportion Achilles tendinosis was intratendinous resection of macroscopically abnormal (tendinosis) tissue, followed by a period of immobilisation and specific rehabilitation exercises.7 During the past 10 years new treatment methods for midportion Achilles tendinosis have included painful eccentric calf-muscle training8 and sclerosing polidocanol injections;9 10 these methods have markedly reduced the need for intratendinous surgical treatment. Interestingly, follow-ups of patients treated with eccentric training and sclerosing polidocanol injections have indicated that clinically successful outcomes are associated with remodelling of the tendon (return towards normal appearance).8 11
To our knowledge, no studies have evaluated Achilles tendon structure and thickness in the long term after intratendinous surgical treatment for Achilles tendinosis. Therefore, we studied the ultrasound appearance of the Achilles tendon after intratendinous surgical treatment.
Material and methods
Fourteen patients (16 tendons in nine men and five women, mean age 43 years, range 27–55) surgically treated (intratendinous surgery) for chronic painful midportion Achilles tendinosis between 1992 and 1999, were included. All patients had tendon pain not allowing them to participate in their desired Achilles tendon loading activity. The patients were active in varying activities on a recreational level, such as walking, jogging and basketball. Clinically and sonographically all patients had tendinosis affecting the midportion of the Achilles tendon.
All patients were examined clinically and their Achilles tendons were imaged using grey-scale ultrasonography. A single experienced musculoskeletal radiologist used a linear multifrequency (8–13 MHz) probe to image tendon structure and measure thickness in the saggital plane. The test–retest reliability for the radiologist was evaluated by examining one tendon 10 times during a short period of time, with repositioning between investigations. The coefficient of variation was 1.1%.
At follow-up calf muscle circumference was measured 10 cm below the knee joint line at standing. Calf muscle strength was tested by asking each patient to perform the maximum number of single leg heel raises. Heel raises were done to a height of 5 cm with the knee braced into full extension.
Results
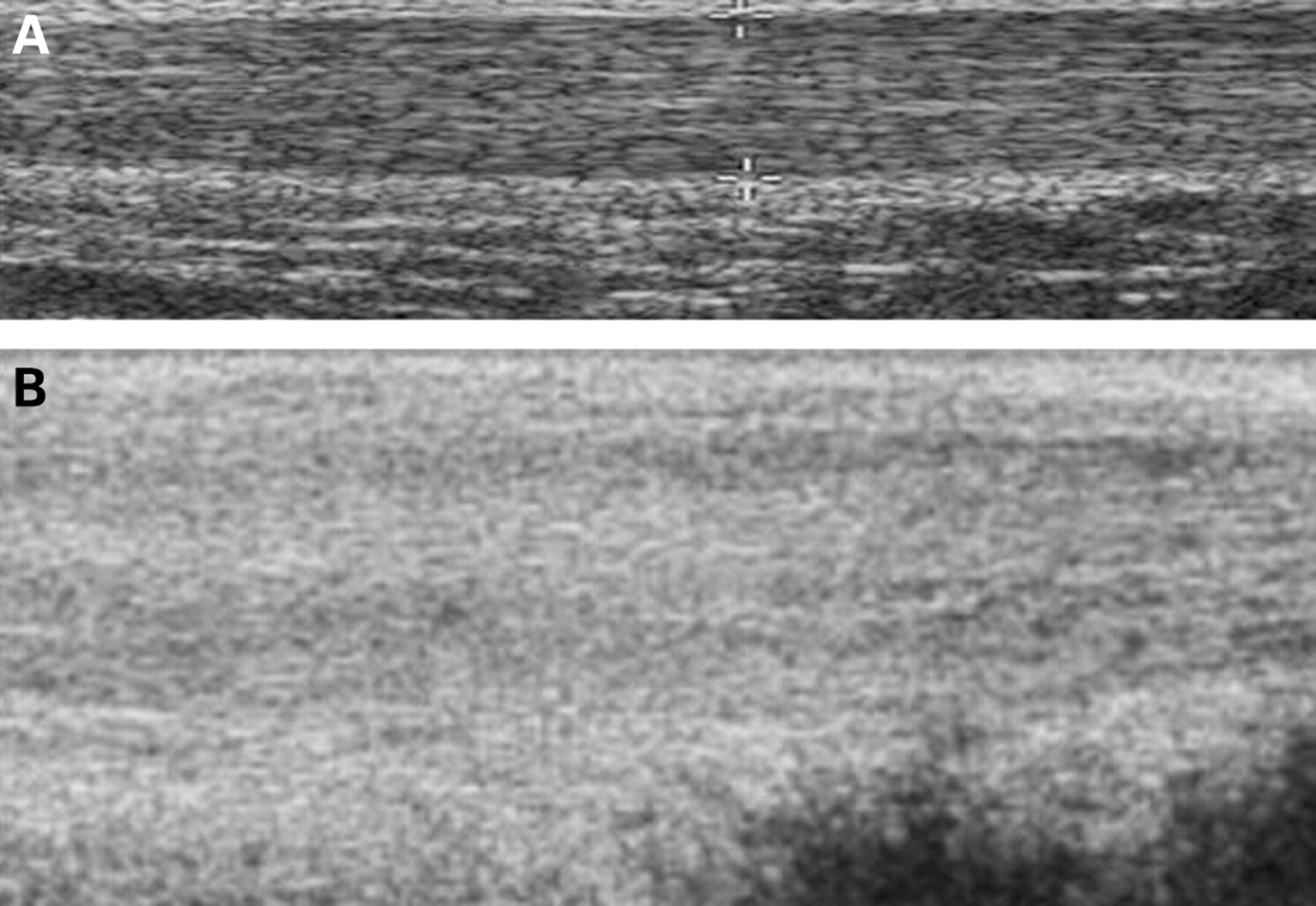
During surgery we excised between 25% and 75% of the tendon thickness. At follow-up, a mean of 13 years after surgery (range 8–16), all patients were clinically satisfied with the result of surgery and were active in Achilles tendon loading activities without restrictions. All patients had structural abnormalities in the surgically treated tendons, and the tendon thickness was thicker (mean 9.3 mm, range 5.9–13.0) than normal tendons in general, that are approximately 5 mm (fig 1A and B).12 There were no significant differences in calf muscle circumference or in functional calf muscle strength tests between the operated and non-operated sides.

{kind=link}
(A) A normal Achilles tendon midportion. Regular structure and normal thickness (5 mm). (B) An Achilles tendon midportion 10 years after intratendinous surgery. Diffuse and irregular structure with thickening (10 mm).
Discussion
In this sonographic and clinical follow-up study of patients surgically treated for midportion Achilles tendinosis, there were no signs of normalisation of the tendon structure 13 years after successful treatment, even though all the patients were active on a recreational level without restrictions. In all patients in this study the surgical excision of abnormal tendinosis tissue was done through a longitudinal skin incision. This was followed by a longitudinal tendon incision and the excision of macroscopically abnormal tendon tissue. The amount of tendon excised ranged from 25% to 75% of the tendon thickness. We believe this to be the most common method of Achilles tendon surgery worldwide.1 2 3 4 7 Consequently, a relatively large part was excised locally in some of the tendons in our study. However, when evaluating these tendons separately, the remaining structural tendon changes at follow-up did not differ between the tendons in which a high percentage of the thickness had been resected, compared with tendons in which a lower percentage had been resected. The results in our study are in line with the results in studies by Svensson and colleagues, who used magnetic resonance imaging13 and tendon biopsies14 15 to demonstrate that the patellar tendon does not normalise within 6 years after harvesting its central third.13 14 15
What is already known on this topic
Eccentric training and sclerosing polidocanol injections are associated with structural remodelling of the Achilles tendon.
What this study adds
Intratendinous surgical revision to treat midportion Achilles tendinosis, a common procedure, is associated with structural tendon abnormalities and thickening even in the very long term. In this cohort, there were no signs of tendon remodelling despite the tendon being pain free and allowing all desired activity.
In patients successfully treated for midportion tendinosis with other methods, eccentric training and sclerosing polidocanol injections, sonographic and clinical follow-ups have shown signs of remodelling of the Achilles midportion, showing a more normal tendon structure and decreased thickness.8 11 Consequently, it seems that intratendinous surgery, in contrast to extratendinous methods (polidocanol injections, eccentric training), causes permanent structural tendon changes.
It could be speculated that the period with immobilisation most often used after intratendinous Achilles surgery is responsible for the remaining structural tendon changes. However, this is contradicted by the findings in the studies on the patellar tendon,14 15 showing remaining structural tendon changes despite the fact that early mechanical loading is instituted after harvesting the central third of the tendon.
It is important to note that all patients in our study were satisfied with the result of the surgical treatment. They were physically active at the desired level, and had no pain in the tendon or weakness in the calf muscle on the operated side. This suggests that the structural abnormalities and thickening of the tendon does not impair tendon function. However, even though our group of patients did not adjust their sporting choices because of their previous tendon surgery, they were involved in recreational activities such as walking and jogging, and not in heavy Achilles tendon loading sports. In a study by Silbernagel et al,16 a comprehensive functional test battery indicated substantial limitations in patients who had recovered from Achilles tendinopathy using an eccentric exercise programme. Our functional tendon testing after intratendinous surgical treatment was limited to the heel raise test. Whether elite athletes have functional deficits after intratendinous surgery that disturb the muscle–tendon capacity remains to be investigated.
We conclude that remodelling of tendons remains to be fully elucidated. Our novel descriptive data add to the clinical picture for which basic scientists seek mechanistic explanation. Why do some tendons appear to return to “normal” and others maintain an abnormal appearance that could be considered to be “scar”? What is the role of mechanical loading and mechanotransduction in this process?
REFERENCES
Footnotes
Competing interests None.