Article Text

Abstract
Background Next to the school environment, the family and community environment are key for young people's behaviour and for promoting physical activity (PA).
Methods A review of reviews was conducted, after which a literature search was conducted (in PubMed, Scopus and PsychInfo) from August 2007 (search date of the most recent review) to October 2010. Inclusion criteria were study population aged 18 years or younger, controlled trial, no PA control condition, PA promotion intervention and reported analyses of a PA-related outcome. Methodological quality was assessed, and data on intervention details, methods and effects on primary and secondary outcomes (PA, body composition and fitness) were extracted.
Results Three previous reviews were reviewed, including 13 family-based and three community-based interventions. Study inclusion differed for each review, but all concluded that the evidence was limited, although the potential of family-based interventions delivered in the home and including self-monitoring was highlighted. A further six family-based and four community-based interventions were included in the updated review, with a methodological quality score ranging from 2 to 10 and five studies scoring 6 or higher. Significant positive effects on PA were observed for one community-based and three family-based studies. No distinctive characteristics of the effective interventions compared with those that were ineffective were identified.
Conclusions The effect of family- and community-based interventions remains uncertain despite improvements in study quality. Of the little evidence of effectiveness, most comes from those targeted at families and set in the home. Further detailed research is needed to identify key approaches for increasing young people's PA levels in family and community settings.
Statistics from Altmetric.com
Introduction
The current generation of young people are generally believed to be insufficiently active to benefit their health,1 2 with levels of physical activity (PA) declining throughout childhood and adolescence.3 Effective strategies are therefore needed to encourage changes in PA behaviour among young people, whether it is promoting maintenance of PA levels in younger children, preventing decline of PA levels in primary school-aged children or promoting increased PA in adolescents. School is often the preferred setting for health promotion in young people, given the large amount of time they spend there.4 However health behaviours are known to be influenced by a variety of factors at a number of ecological levels, of which the school setting is only one.5 The family environment and the community in which young people live in or belong to are also believed to have an important influence on their health behaviours. This ecological perspective on health behaviour has gained in popularity in the past decade, whereas simultaneously PA promotion in young people was identified as a key focus of efforts to promote population health in various international policy documents.6 7 This has resulted in an increase in efforts to evaluate PA promotion interventions in young people in various settings. This review therefore explores the effectiveness of interventions to promote PA in children and adolescents, delivered in the family and community setting, summarising previous reviews and updating the evidence with findings from recently conducted controlled trials (CTs).
Methods
This review applies a mixed-methods strategy. Three systematic reviews on PA promotion in children and adolescents, with a focus on family and community interventions,8,–,10 will be reviewed in the first part of this review, covering the available evidence up to the date of the most recent search (August 2007).10 In the second part of this review, an updated literature review will be conducted covering publications between August 2007 and October 2010 to establish the effectiveness of more recent efforts.
Updated literature review
Literature search
A literature search was conducted based on the methods of a previous review.9 Using the same search terms, with a limited focus on community and family settings, we searched PubMed, Scopus and PsychInfo in November 2010 (see online supplementary table 1). Inclusion criteria were (1) study population of healthy young people (≤18 years); (2) promotion of PA through behaviour change as a main intervention component; (3) intervention delivered outside of the school or primary care setting; (4) the control group received no or a non-PA intervention; (5) reported statistical analyses of a PA outcome measure. Weight status was not an exclusion criterion, although we excluded studies solely recruiting from clinical settings or studies including children with other health problems. One reviewer (EvS) checked the titles obtained from the searches, after which each of the two reviewers reviewed half of the resulting abstracts. Full text studies were obtained and reviewed by both reviewers independently, and discrepancies were resolved after discussion.
For the purpose of this review, we considered all interventions that were outside of the school setting and not delivered in a clinical setting to be community interventions. Interventions set in the school and including a family or community component are reviewed in a related review in this special issue.11 We further classified some of these interventions as family interventions if they included the active participation of one or more family members of the child. All interventions targeted at the individual child only were categorised as community based. After-school interventions offered only to children at that specific school were considered to be an extension of the school setting and were therefore not included in this review. Interventions that used school facilities but were made available to all children in the neighbourhood/community (irrespective of whether or not they attended a specific school) were also considered community-based interventions.
Methodological quality
We assessed the methodological quality for descriptive purposes using a previously applied 10-item rating system.9 The assessment focused on internal validity and statistical analyses, including randomisation, validity of the PA measure, blinding and intention-to-treat analyses. All items were scored as ‘positive’, ‘negative’ or ‘not, or insufficiently, described’ by two reviewers independently. In cases of disagreement, consensus was reached by discussion. Only positive scores were accumulated; studies were considered to be of high quality if they scored 6 or more for randomised controlled trials (RCTs) or 5 or more for CT.
Summarising the evidence
Information on the intervention content, target population, evaluation methods and results on PA (and body composition and fitness where provided) were extracted by one reviewer (AM). A narrative account of the evidence is provided. We compared interventions and their evaluations on the intervention strategies applied, the populations targeted and methodology used to help identify whether there were common components potentially explaining the intervention effect.
Results
Summary of previous reviews
Table 1 provides an overview of the methodology and results of the three recent systematic reviews on PA promotion in children and adolescents. Using the definitions described earlier for our updated review, a total of 13 family-12,–,24 and three community-based25,–,27 studies were included across the three previous reviews, with no single review including all studies. Six of the family-based interventions were reported to have a significant positive effect on PA,16 19 21,–,24 whereas none of the community-based interventions had a significant positive effect on PA. Below we summarise the findings from each review; however it should be noted that the interpretation of family- and community-based interventions varied across the reviews, leading to the same intervention being classified differently in some cases. In addition the reviews differed in their assessment of methodological quality, evidence synthesis, inclusion and exclusion criteria and the stratification for presenting the results (based on age or weight status). However despite these differences, the reviews drew broadly similar conclusions.
Summary of previously published reviews on PA promotion in children with a focus on family- and community-based interventions (presented in chronological order)
Salmon et al8 reviewed the available evidence up to June 2006 and included both controlled and uncontrolled studies. In their narrative account of the literature, they highlighted the strategies applied and potential methodological strengths and weaknesses. Of the nine included interventions conducted in the family setting,12,–,17 19 23 28 29 seven were classified as short term (average duration: 12 weeks), of which two showed significant positive results. One of these studies evaluated an intervention in which print materials were sent to families,16 whereas the other (the only study in adolescents) encouraged mothers and adolescent daughters to exercise together.23 However both were uncontrolled studies, and the reliability of their results should be questioned. One of the two long-term interventions, a 3-year Finnish intervention in children aged 4 years at baseline, involving annual sessions with parents along with information posted out twice yearly,17 was found to be effective in increasing very active outdoor play in a CT. With a few exceptions, compliance and retention rates in the family-based interventions were found to be high overall. The authors concluded that “the evidence was not overwhelming” (p 155)8 and argue a need for testing generalisability of interventions, sustainability of the effect and effective strategies for engaging families.
Three community-based interventions25 30 31 were reviewed by Salmon et al,8 all targeting children. They concluded that studies were limited by design issues (retrospective design or no true control condition) and low participation and response rates. One study, a retrospective cross-sectional evaluation of environmental changes to the area surrounding schools,31 showed a positive effect, whereas no overall effects were observed for the other two studies. Overall, the authors concluded that “further evidence of efficacy and sustainability of interventions promoting young people's PA in the family and community settings is needed.” (p 155)
Van Sluijs et al 9 reviewed the available evidence up to December 2006, only including controlled studies and assessing methodological quality using a 10-item scale. A system of levels of evidence was used to arrive at conclusions, whereby only those studies with the best available design and highest methodological quality within a category contributed to the conclusion. Conclusions were drawn separately for children and adolescents. Five family-based interventions13 15 17 18 20 were reviewed. Two involved educational sessions and information only, whereas the remaining three additionally included activity sessions. Four were targeted at children, with only one targeting adolescents. On the basis of the three highest-quality studies in children and the one study in adolescents, none of which showed a significant positive effect, the authors concluded that there was no evidence for effect of family-based interventions in children and that the evidence for effect in adolescents was inconclusive.9 The three community-based interventions14 26 27 were all classified as educational interventions, focusing on information provision and activity sessions. Two were delivered to scout groups; one targeting adolescent boys for 9 weeks,27 and the other targeting primary school-aged girls over a period of 2 years.26 The remaining intervention was a pilot study targeting African American 8-year-old girls and delivering the intervention during a summer camp.14 None showed a significant positive effect, leading to the conclusion of no evidence for effect of community-based interventions in children and inconclusive evidence for effect in adolescents.
Although the focus on methodological quality is a strength of the review by Van Sluijs et al,9 it limited their potential to explore the strategies evaluated and the potential of intervention strategies used in studies with weaker designs. On the basis of their review of the evidence, the authors questioned the usefulness of “carrying out family-based… interventions, as most studies identified did not report positive results, but also suggested that ‘it is necessary to identify and learn from the limitations of these interventions and their evaluations’.” (p 10, web paper9)
National Institute for Health and Clinical Excellence (NICE)10 reviewed the literature up to August 2007, and similar to Salmon et al,8 the authors provided a narrative account of both controlled and uncontrolled studies, although additionally included a methodological quality rating for descriptive purposes (high, good or low quality). Eleven family-based interventions were included,13,–,16 18 19 21,–,24 32 33 most of which were conducted in children and four specifically targeted children who were (or were at risk of becoming) overweight or obese. These four studies were considered to be of good or high quality, and two reported positive results, both of which were conducted by the same research group. They involved similar intervention strategies targeting the whole family and including self-monitoring with pedometers.21 24 In their conclusion, the review authors highlighted that “characteristics of successful interventions [in overweight/obese children] included being located in the home… and focused on small, specific lifestyle changes.” (p 40)10 In contrast, unsuccessful interventions required regular attendance at a site external to the home. Seven family-based interventions targeted young people regardless of weight status, three of which were of low quality, and four showed positive changes (three studies of good quality and one of low quality). Two of these successful studies were small-scale interventions of female family members exercising together.22 23 One study was uncontrolled. Again, successful interventions were found to be located in the home and involving information packs, whereas less effective strategies required attendance of regular sessions outside the home.
The two community-based interventions27 34 included in the NICE review targeted boys (because of the specific nature of this review, the results for the girls in one of the studies were included elsewhere35). One study, delivered to Boy Scout groups,27 was considered to be of good quality. The second, low quality, study involved the provision of Heart Health information, mainly in schools.34 Neither of the two studies was able to show a significant positive intervention effect. However the authors concluded that “there is no immediate or obvious reason why interventions in community groups such as boy scouts or church groups should not be successful and further research should be encouraged in this area.” (p 75)10
In general all reviews highlighted common methodological issues, including lack of long-term follow-up, poor validity of PA measures used, small study samples and limited information on intervention fidelity and implementation. In addition Salmon et al8 and Van Sluijs et al9 stressed the need to study mediators of change to better understand why an intervention did (or did not) work. Despite the observed lack of effectiveness, further high-quality work was encouraged.
Update of evidence
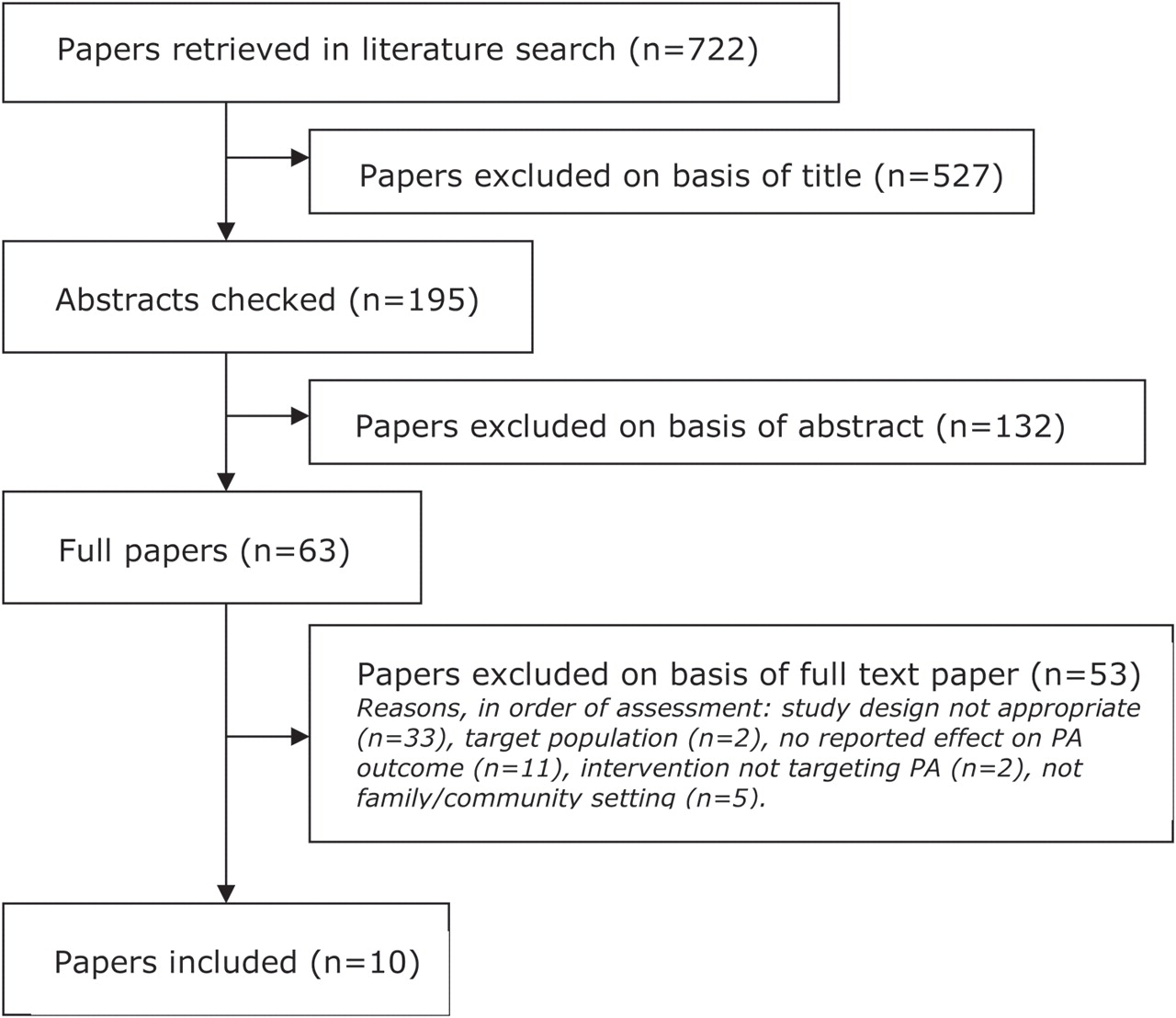
Figure 1 provides an overview of the flow of the literature search. A total of 10 studies were included, nine RCTs, most of which were published in 2010 and included children rather than adolescents. Six studies were classified as family-based interventions,36,–,41 whereas the remaining four were community based42,–,45 (table 2 and online supplementary table 2). The methodological quality of the studies ranged from 2 to 10, with five studies classified as high quality (table 3 and online supplementary table 3). In general randomisation procedures were described appropriately, and most studies used intention-to-treat analyses. However only four studies reported on the validity of the measure of PA, and three had a follow-up after intervention completion of 6 months or longer.
{kind=link}
Identification of included studies in updated review (August 2007 to October 2010).
Summary of key characteristics of studies included in update review (shaded studies reported a significant positive effect on PA)
Key methodological indicators of studies included in updated review (shaded studies reported a significant positive effect on PA)
Effect on PA
Three of the six family-based interventions reported a significant positive effect on PA.36 38 40 One was a high-quality RCT of an 8-month intervention based on social cognitive theory in which the children attended eight weekly 45 min sessions and the parents attended two 2 h workshops.36 The other two were low-quality RCTs, targeted at overweight fathers and their children38 and at families of obese children.40 No consistent differences in terms of intervention (such as theoretical basis), target population or methodology could be identified between the effective and ineffective interventions (see tables 2 and 3).
One of the four community-based interventions, a low-quality CT of an environmental intervention,43 reported a significant positive effect on a PA-related outcome measure. In this study the playground of a local primary school was made available during out-of-school hours (including weekends) and supervision was provided during these periods. The three other interventions, including two mentoring schemes42 44 and an intervention targeting female scouts,45 were ineffective in increasing overall activity. The latter intervention was shown to significantly increase objectively measured PA during the troop meetings, but no intervention effect was observed for overall, self-reported, PA.
Effect on secondary outcomes
Five of the six family-based interventions reported on changes in anthropometry.36 38,–,41 Only one did not report a significant effect on anthropometry,38 despite a reported effect on PA. In addition one study reported a significant decrease in body mass index in the intervention group and a significant increase in the control group, but no between-group tests were conducted.39 The only study reporting on a fitness-related outcome measure, heart rate recovery, reported a significant positive effect.40 Interestingly, interventions targeted at overweight or obese populations were more likely to report positive effects on anthropometry, irrespective of the effect on PA levels.
All studies evaluating community-based interventions reported on anthropometry outcomes. Only one, a home-based mentoring scheme, reported a significant positive effect.42 No study reported on a fitness-related outcome.
Discussion
PA promotion in young people is currently a key public health strategy. Schools are often the preferred setting for these initiatives, not least because young people spend many hours at school, and it provides researchers with a captive population. Nonetheless, considering the variety of influences on young people's behaviours, interventions in other settings should also be considered. The aim of this article was to present an overview of the effectiveness of family- and community-based PA interventions using a mixed-methods review strategy. Previous reviews of the literature highlighted the paucity of evidence in this area, especially from community-based interventions, and the limited methodological quality of the studies. The updated review of the evidence shows important progress, with an additional 10 controlled studies published since August 2007, which were generally found to be of higher methodological quality than previous work. However there remains a lack of (good quality) evaluations of community-based interventions and identifying the components of family-based interventions associated with effectiveness proved challenging. This was also highlighted by a previous review studying how to engage parents to increase youth PA,46 where they concluded that no obvious pattern could be identified. However they suggested that a medium-to-low level engagement, such as parent training, family counselling or telephone-based interventions, as opposed to actually engaging parents in a family PA programme with their children, may be effective.
In the updated review, three of the six family-based studies reported significant positive effects, such as 2327 more steps per day38 or 3.9 h of additional PA per week.40 However comparisons of the interventions, target populations or evaluation methods did not identify common components across the effective and ineffective interventions. As in the previous reviews, most studies targeted children, which may be a reflection of the perception that families become less of an influence throughout adolescence. Neither of the two studies including adolescents, a community-based mentoring scheme42 and family-based educational intervention,39 showed a positive effect. Only one community-based intervention43 was shown to be effective, which was the only environmental intervention and the only intervention solely targeting PA. On the other hand, the evaluation of this intervention, where the school playground was made available during out-of-school hours, had a low methodological quality score, raising doubts about the validity of the conclusions.
The earlier reviews tentatively showed that family-based interventions may be more likely to be effective if they are set in the home and include self-monitoring (using pedometers) and goal setting for specific lifestyle changes (such as increasing baseline steps by 2000 steps per day). These strategies, however, were not replicated in more recent research. Instead most interventions focused on provision of information in group settings and activity sessions for the children. Although a few studies included elements of self-monitoring, these were only minor intervention components and unlikely to have made substantial contributions to a potential intervention effect. Self-monitoring with pedometers can be effective in increasing PA levels in both adults and young people, especially when combined with goal setting.47 48 However the few pedometer-based studies conducted in young people to date have tended to be set in schools and were of medium-to-low methodological quality.48 A recent review of behaviour change strategies in family-based childhood obesity prevention interventions also highlighted ‘prompting specific goal setting’, ‘prompting self-monitoring’, ‘setting graded tasks’ and ‘providing performance feedback’ as common components of effective interventions.49 Based on the previously identified potential of these strategies, it is important that their applicability in the family or community setting is further explored and tested, using high-quality research with longer-term follow-up.
Intervention implementation is known to affect outcomes,50 and eight different aspects of implementation can be identified: fidelity, dosage, quality, participant responsiveness, program differentiation, monitoring of control condition, programme reach and adaptation. Few of the studies included in this review reported on attempts to assess aspects of implementation beyond attendance rates. Where reported in the family-based interventions,37,–,40 attendance was generally found to be high, despite none of them being delivered in the home. The required attendance of both children and parents at locations outside the home has previously been suggested to affect compliance,10 but this does not seem to have been the case in the more recent studies. Intervention delivery in general was poorly described, and only one study45 reported on the quality of implementation of the intervention, as assessed by the intervention deliverers. One area of concern in this literature is the reach of the intervention programme. Studies often reported using wide-ranging recruitment methods, with the potential to reach a large population, such as media campaigns, brochures and flyers. However no study reported on the recruitment rates compared with those eligible or invited to participate or on representativeness of the study sample to the target study population, raising questions regarding the generalisibility of the results to wider populations and the potential for wider implementation.
Previous reviews have highlighted the potential of environmental interventions both inside and outside the school setting.8 9 Most of these interventions aim to create safe opportunities for active play or travel. The only environmental intervention included in our updated review also elicited significant positive effects.43 Two recent reviews also showed that after-school programmes can be effective in promoting children's PA.51 52 These programmes generally also include the provision of safe and accessible opportunities for PA, next to health education. A small but growing body of evidence therefore seems to indicate that increasing safe opportunities for children to engage in play-based activities both at school and out of school may be a worthwhile strategy to pursue. Nonetheless the reported results must be interpreted cautiously because most studies used small sample sizes and were of poor quality, affecting the internal validity of the studies and the reliability of the conclusions drawn. The evaluation of environmental interventions or other natural experiments potentially affecting PA or other health behaviours is known to be challenging and fraught with difficulties.53 54 It is however crucial for future decision making that these collective interventions are evaluated with appropriate study designs and robust measures of the outcome to better estimate their effectiveness and allow for comparisons with other approaches.53
Several studies reported positive effects on anthropometry outcomes. Those studies that targeted overweight or obese participants were more likely to report significant positive effects, irrespective of the reported effect on PA. This is likely to be predominantly explained by the greater potential to obtain an effect on body composition among these participants than in the general population. Nevertheless several other issues may have contributed to this finding. Body composition can be measured more precisely and with less error than PA.55 Indeed, for many studies, body composition was the main outcome measure, and the sample size will have been determined accordingly. In addition, the interventions targeted both dietary and PA behaviour, and two of the studies targeting overweight or obese participants reported significant positive outcomes for dietary behaviour, but not for PA39 41 (the remaining study did not report on a dietary outcome40). It may be that for overweight or obese populations, improvements in dietary behaviour are – at least initially – more important to obtain improvements in body composition, although no mediation analyses were presented for the studies included in this review. However it is likely that for weight maintenance, improvements in both PA and dietary habits are necessary. Moreover, it is important to stress that PA has important health benefits independent from weight.1 56
Although the methodological quality of the more recently conducted evaluations seems to have improved, several challenges still remain. Only three of the 10 studies in the updated review used an objective measure of PA, and only four reported on the validity of their PA measure. We found that the type of PA measure used was not related to intervention effectiveness. However increasing the precision of the measurement of PA and studying how changes occur across the week and in different domains will allow for a more thorough investigation of the effects of interventions. Only three studies reported a follow-up of 6 months or longer, with one reporting a significant positive intervention effect. The long-term effect of family- and community-based interventions therefore also remains unclear. Indeed previous literature seems to suggest that repeated intervention efforts may be necessary to obtain established changes in PA habits.57 Few studies investigating PA promotion in young people have investigated mediation of the intervention effect,58 and to our knowledge, none of the studies in the updated review reported on mediation effects. Studying mediation is an important strategy to develop an understanding of effective intervention elements and the mechanisms of change, and it is recommended that future evaluations include measures along the causal pathway to study this.
As with the primary studies, this review has its strengths and limitations. We conducted a systematic literature search, assessed final study inclusion and methodological quality by two reviewers independently, assessed methodological quality and systematically investigated potential common components of effective interventions. Limitations include the restriction of the literature search to three databases, only one reviewer undertaking the initial reviewing stages and the potential for publication bias. However we aimed to minimise the effect of the former two issues by selecting the three key databases based on previous review experience9 and by using broad initial review criteria. We based our quality assessment on the published evidence rather than contacting all the primary authors to allow us to both study the quality of the studies and highlight continuing issues with the reporting of trials.
Conclusion
Using a mixed-method review strategy, this article shows that findings for the effectiveness of family- and community-based interventions remain uncertain, especially among adolescent populations. The limited evidence available comes from interventions targeted at families and set in the home. The efficacy and sustainability of environmental interventions and interventions including self-monitoring using pedometers outside of the school setting should be investigated further with high-quality evaluations and longer follow-up.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Funding The work of EMFvS was supported by the Centre for Diet and Activity Research (CEDAR), a UKCRC Public Health Research Centre of Excellence. Funding from the British Heart Foundation, Department of Health, Economic and Social Research Council, Medical Research Council, and the Wellcome Trust, under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.