Article Text

Abstract
This study reports the time to sustain a mild traumatic brain injury (mTBI) among a cohort of community rugby union players. Demographic and player characteristics were collected and players followed up for between one and three playing seasons. 7% of the cohort sustained an mTBI within 10 h of game time, increasing twofold to 14% within 20 h. The mean time to first mTBI was 8 h with an SD of 6.2 (median 6.8 h; IQR: 2.9–11.7 h). Players reporting a recent history of concussion were 20% more likely to sustain an mTBI after 20 h of game time compared with those with no recent history of concussion. Players were likely to sustain an mTBI in shorter time if they trained for <3 h/week (HR=1.48, p=0.03) or had a body mass index <27 (HR=1.77, p=0.007). The findings highlight modifiable characteristics to reduce the likelihood of shortened time to mTBI.
Statistics from Altmetric.com
Introduction
With rugby union having one of the highest participation levels in contact sports1 2 and reporting the third highest incidence of mild traumatic brain injury (mTBI),3 the incidence and management of mTBI requires detailed investigation.3,–,5 Although much of the literature describes the incidence and risk factors for mTBI occurring in contact sports like rugby, no study to date has investigated the time to mTBI for rugby players at a community level. Given the incidence of mTBI in community rugby players,4 there is a need to identify if mTBIs are sustained at a particular time within a playing season and if key factors exist that shorten the injury-free period or time to mTBI. Such information is needed to inform the timing of interventions to reduce the incidence of mTBI.
Methods
A cohort of 3207 male community rugby players (aged 15–48 years) was recruited preseason from schools or rugby clubs (grade or suburban competition level) throughout the Sydney metropolitan area. This prospective cohort study has been described in detail previously.4 In brief, players were asked to complete a questionnaire relating to demographic and personal information and questions relating to player characteristics such as principal playing position, amount of training, previous rugby experience and the use of protective equipment. Players were also asked whether they had a history of recent concussion (in the previous 12 months) and if so, how many were sustained.
All players were followed for up to three seasons during 2005–2007, and players were recorded as sustaining an mTBI during the game if they received a knock to the head that resulted in dizziness, confusion, loss of coordination and/or loss of consciousness and required (1) stoppage of play, (2) stoppage of play with the player receiving medical attention or (3) the player to leave the field. The main outcome measure was the time to first mTBI, namely the total number of hours of game exposure played up to the time the player sustained an mTBI. For the purposes of this study, we use the terms ‘mTBI’ and ‘concussion’ interchangeably.
The final dataset comprised 1958 players after removing cases due to incomplete study data (n=195), missing exposure or injury data (n=429), unreliable observations of mTBI (n=215) or if players were in a different football code (rugby league) (n=410). Preliminary analysis showed that comparison of baseline characteristics between players included in the final dataset and those excluded from the cohort showed no significant differences in height, weight, body mass index (BMI), impulsivity score, years of rugby experience, training volume and concussion history. A significant age difference, however, was found with the mean player age of 23.1 years (SD 5.6) in the final dataset compared with 21.6 years (SD 5.5) in the excluded group. Age has subsequently been adjusted for in all analyses.
Statistical analysis
Statistical analyses were performed using SAS version 9.26 and Stata version 10.7 Kaplan–Meier survival curves were constructed to describe time to first mTBI. An adjusted regression analysis was performed using the Cox proportional hazards model stratified by competition level.
Results
The mean player age was 23.1 years (range: 15–48) with a median BMI of 27 kg/m2 (range: 18–51). Of the 1958 players, 10% (n=187) sustained ≥1 mTBI throughout the study with a total of 215 mTBIs sustained overall. Of the 187 concussed players, 87% (n=163) of players sustained one mTBI and 13% (n=24) sustained two or more mTBIs (range: 1–4). For the 187 players who sustained ≥1 mTBIs, the mean time to the first mTBI was 8 h with an SD of 6.2 (median 6.8 h; IQR: 2.9–11.7 h).
After adjustment for censoring, 7% of the cohort had sustained their first mTBI within 10 h of game time (just under the average number of hours played in one season), increasing twofold to 14% within 20 h of game time (the approximate total length of one season/20 games for adults).
The age-adjusted crude HRs for player characteristics showed that competition level was a significant risk factor for mTBI (at the univariate level) with schoolboys at a lower risk of mTBI (HR=0.61; 95% CI=0.39 to 0.97) compared with adult level of competition. At the multivariate level, players who reported a history of concussion within the previous 12 months were almost twice at risk of sustaining an mTBI compared with those who reported no recent concussion (HR=1.89; 95% CI=1.36 to 2.68). Players with a BMI less than the median for the cohort (<27 kg/m2) were at an increased risk (HR=1.77, 95% CI=1.30 to 2.42) of sustaining an mTBI compared with those with a BMI ≥27 kg/m2. Players who trained for <3 h/week had an almost 50% increased risk (HR=1.48, 95% CI=1.06 to 2.08) of sustaining an mTBI compared with those who trained for ≥3 h/week.
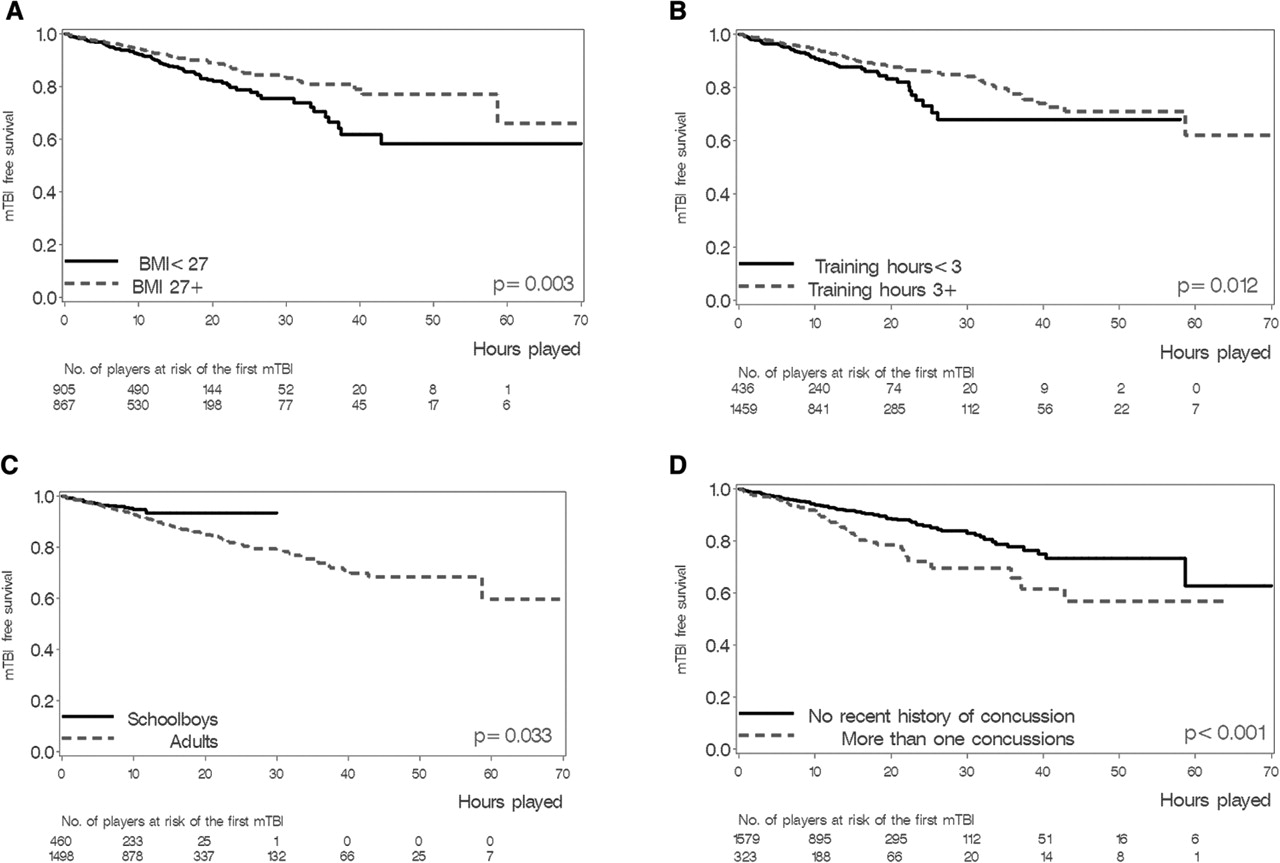
Figure 1 illustrates the proportion of players who remained mTBI-free during the hours of game played throughout the study. Players who trained for <3 h/week, had a BMI <27 kg/m2, or reported a recent history of concussion were most likely to sustain an mTBI in shorter time than others. Players with a BMI <27 kg/m2 were approximately 10% more likely to sustain an mTBI within the first 20 h of game time exposure (or equivalent to one total playing season) compared with those with a BMI ≥27 kg/m2. Players who trained for <3 h/week were 20% more likely to sustain an mTBI after 20 h of game time compared with those who trained for ≥3 h/week. Players in adult level competition were 10% more likely to sustain an mTBI within the first 20 h of game time compared with those in the schoolboy competition. Players who reported a recent history of concussion were 20% more likely to sustain an mTBI within the first 20 h of game time compared with those who reported no recent concussion.
{kind=link}
Proportion of players who remained mTBI-free over time (hours of game exposure) comparing binary categories within the four key variables in the adopted regression model: (A) player BMI; (B) number of training hours; (C) competition level and (D) recent concussion history. *Please note that in Figure 1c the truncation of the curve at 30 h for schoolboys is due to the difference in the average number of game hours played by adults (mean 14.8 h; 95% CI: 14.2 to 15.5) compared with schoolboys (mean 10.4 h; 95% CI: 9.9 to 10.8).
Discussion
The findings from this study highlight that for every 10 h of game time played, approximately 7% of players sustained an mTBI. Also, on playing all games within a rugby season (approximately 20 h for adults), an estimated 14% of players in this cohort sustained an mTBI. These proportions highlight the need for rugby clubs to have comprehensive medical/health support for non-professional players to ensure timely identification and management of mTBI.
The results also highlight the linear incidence of mTBI with little change in the incidence of mTBI between the first or second half of the season, dissimilar to rugby union studies reporting higher injury rates at the beginning of the season.8,–,11 Also, players who reported having a recent history of concussion were at a 20% increased risk of sustaining an mTBI within 20 game hours. This supports a number of recent studies suggesting concussion history as a risk factor for repeat concussion.12,–,16 The study also identified that players had a 10% increased risk of sustaining an mTBI within 20 h if they had a BMI less than the median of the cohort (<27) or trained for <3 h/week. Both these findings contrast with that reported for studies of other rugby injuries. Players with a BMI >26.5 had a higher rate of injury17 and amateur players with greater levels of training experienced more match injuries albeit not solely mTBI injuries.17 18 Although only significant at the univariate level, schoolboy competition level having a lower risk of mTBI compared with adult level is currently a particularly pertinent issue in rugby, and highlights the need for further investigation specific to schoolboy level rugby.
What is already known on this topic?
A high incidence of mild traumatic brain injury (mTBI), or concussion, among non-professional (community) rugby players has been reported. Recent research has highlighted the incidence (8/1000 game exposure hours) and management of mTBI, particularly among community rugby players, as areas requiring further investigation.
What this study adds
The study is the first to determine time to mTBI in community rugby players and risk factors that increase the likelihood of mTBI within 20 h, namely concussion history, player size and training volume. The findings highlight characteristics that, if targeted, could reduce the likelihood of shortened time to mTBI.
Conclusion
The findings highlight the proportion of community rugby players who sustain an mTBI within 20 h of game exposure time. Moreover, the risk factors for time to mTBI — a recent history of concussion, the player's body size and the amount of training undertaken during the season — increase the likelihood of an mTBI occurring within 20 h or one season observed in our study. Given the incidence of mTBI and that approximately 14% of players had sustained an mTBI within the first 20 h of play in the study, there is a need for timely identification and management of this injury.
References
Footnotes
-
Funding SJH was supported by postgraduate scholarship funding from the Australian Government's National Health and Medical Research Council, and scholarship funding from the NSW Sporting Injuries Committee. MRS was also supported by funding from the Australian Government's National Health and Medical Research Council. LL was funded by the New South Wales Health Biostatistical Training Program. This study was supported by the US Centers for Disease Control and Prevention grant 5R49CE323155 to the University of Pittsburgh Center for Injury Research and Control.
-
Competing interests None.
-
Ethics approval Approval was obtained from the Human Research Ethics Committee at The University of Sydney.
-
Provenance and peer review Not commissioned; externally peer reviewed.