Article Text

Abstract
Aim To analyse postmortem cases of myocardial infarction (MI) with normal coronary arteries in terms of patient characteristics, features of the MI and risk factors.
Methods This retrospective non-case controlled study was carried out at a specialist cardiac pathology department at a tertiary cardiac referral centre. Cases of histologically confirmed MI and normal coronary arteries during the period 1996–2010 were identified and analysed for the presence of risk factors.
Results Nineteen cases of histologically confirmed MI and normal coronary arteries were identified with a similar gender ratio 1:1.1 (male:female) and mean age of 33±12 years (range 14–58). All patients died suddenly. The location of the infarct was variable, with left anterior descending artery territory being the single most prevalent (47%). Risk factors were identified in the majority of cases (n=14), with some cases experiencing more than one association, including alcohol and/or predominately class A drug use (n=7), including cocaine, inflammation (n=2), hypercoagulable state (n=3) and exertion (n=2).
Conclusions Current data regarding prognosis in MI with normal coronary arteries suggests a favourable outcome in the context of major cardiovascular events. No large series of fatal cases have been reported. This study highlights that this entity can be fatal and its prognosis may be less favourable than currently considered. This autopsy series also demonstrates that the causation of MI with normal coronary arteries is complex and multifactorial, including a history of alcohol and/or drug use. It also highlights the importance of accurate epidemiological data from referring pathologists.
- Autopsy
- autopsy pathology
- cardiothoracic pathology
- coronary artery spasm
- histopathology
- hypercoagulability
- myocardial infarction
Statistics from Altmetric.com
- Autopsy
- autopsy pathology
- cardiothoracic pathology
- coronary artery spasm
- histopathology
- hypercoagulability
- myocardial infarction
While the leading cause of myocardial infarction (MI) in patients with coronary heart disease is plaque rupture, MI with normal coronary arteries has been recognised for many years. Its prevalence ranges from 1% to 12% according to the angiographic definition of normal or near-normal used. Some studies define ‘normal’ as coronary arteries with smooth contours and no focal luminal reduction.1 Others view a less than 30% stenosis as insignificant,2 while many more studies have considered only greater than 50% stenoses as significant in causing acute coronary syndrome.3–5 Patients with MI and normal coronary arteries tend to be younger,6 and have a lower prevalence of cardiovascular risk factors compared with patients with obstructive coronary artery disease.7–9
A number of mechanisms have been postulated to account for this phenomenon, including coronary artery vasospasm, concealed atherosclerosis, thrombosis and hypercoagulability, embolisation and inflammation.1 10 Furthermore, coronary artery spasm can be induced by catecholamine excess, alcohol and cocaine abuse, cigarette smoking, withdrawal of calcium antagonists, minimal but diffuse coronary atherosclerosis and endothelial dysfunction. Thrombosis secondary to hypercoagulability can be inherited, such as factor V Leiden mutation, or acquired, for example, oestrogen therapy, pregnancy or postoperative state. Embolisation is thought to account for a very small percentage of cases, and may be caused by the presence of native or prosthetic valve disease, endocarditis or left atrial myxoma. Patients with MI and normal coronary arteries have also been shown to have significantly more frequent upper respiratory tract infections within 2 weeks before MI. However, the mechanism linking this type of inflammation to MI is unknown.10 MI with near normal coronary arteries following strenuous exercise has also been reported.11
Begieneman et al12 reported basement membrane thickening in intramyocardial arteries in acute MI, identified electron microscopically, indicating a further contributing mechanism.
Prognosis in patients with MI and normal coronary arteries is often viewed as favourable. A recent paper by Ong et al5 found that during a 3-year follow-up there was no cardiac death or non-fatal MI in a group of 76 patients without a culprit lesion, defined as a greater than 50% stenosis. Other groups have also demonstrated an excellent prognosis with no major cardiac events at follow-up.2 9 Other studies disagree; major cardiac events including death, heart failure, stroke or re-infarction occurred in 25% of a cohort of 91 patients during a 3-year follow-up.1 Also, Raymond et al8 found that nine of 74 (12%) patients with MI and normal coronary arteries died of a cardiovascular cause, with six dying suddenly.
To date no large autopsy series has been published on this entity. We report all cases of sudden cardiac death (SCD) with MI and in whom the coronary arteries were entirely normal on detailed examination referred to our tertiary cardiac pathology centre.
Methods
Criteria for case selection
Our database includes 1980 cases of non-atheromatous SCD referred to a specialist tertiary cardiac pathology centre, part of the National Heart and Lung Institute and the Royal Brompton Hospital. From this database we retrieved cases of MI with normal coronary arteries.
Pathological analysis of all cardiac tissue including the histology was performed by MNS with the consent of the coroner and the family of the deceased. Heart tissue was examined thoroughly and MI was confirmed using histological criteria for acute and chronic ischaemic damage.13 Major epicardial coronary arteries, including left main stem, left anterior descending, left circumflex and right coronary arteries (RCA) were cross-sectioned at 3–5-mm intervals and verified to be entirely normal macroscopically and histologically, with no atherosclerotic plaques. The presence of other pathologies, including myocarditis, inflammatory cell infiltration of the endothelial layer of the coronary arteries or abnormalities in the intramyocardial vessels, was excluded by light microscopic examination of H&E stained slides.
This study was approved by the ethics committee of the Royal Brompton Hospital, reference number 07/Q0404/9 and 10/H0724/38 and complies with the requirements of the Human Tissue Act, 2004.
Patient demographics and detection of risk factors
Data on age, sex, circumstances of death, antecedent cardiac symptoms, past medical history and toxicology were obtained for each patient from the referring pathologist or coroner when available.
Characteristics of MI
The location of each infarct in the ventricular myocardium was determined. The age of each infarct was estimated on well-established histological criteria that can be observed during the evolution of an MI. In the first 17–24 h MI is impossible to recognise both macroscopically and microscopically. Features of an acute MI in the first 24–48 h include contraction band necrosis, myocyte swelling, loss of myocyte nuclear detail and a neutrophilic infiltrate. Days 3–7 are characterised by an infiltrate of lymphocytes and macrophages around necrotic myocytes. Granulation tissue with myocyte loss, pigmented macrophages and myofibroblasts are seen on days 7–42. The presence of fibrosis indicates an infarct more than 6 weeks before death.13
Results
Case selection
Histology confirmed the presence of acute MI in 16 patients, and an old fibrosed MI in three patients. The coronary arteries in all 19 cases were entirely normal with smooth contours, no luminal irregularities and no atheroma. The intramyocardial arteries were normal.
Patient characteristics
Gender was similarly distributed (men n=10; women n=9) and the mean age was 33.8±12.2 years (range 14–58). There was no significant difference in the age distribution between male and female patients. The distribution of age at death is shown in figure 1.

Age and gender distribution of patients who died suddenly with a myocardial infarction and normal coronaries.
Circumstances of death
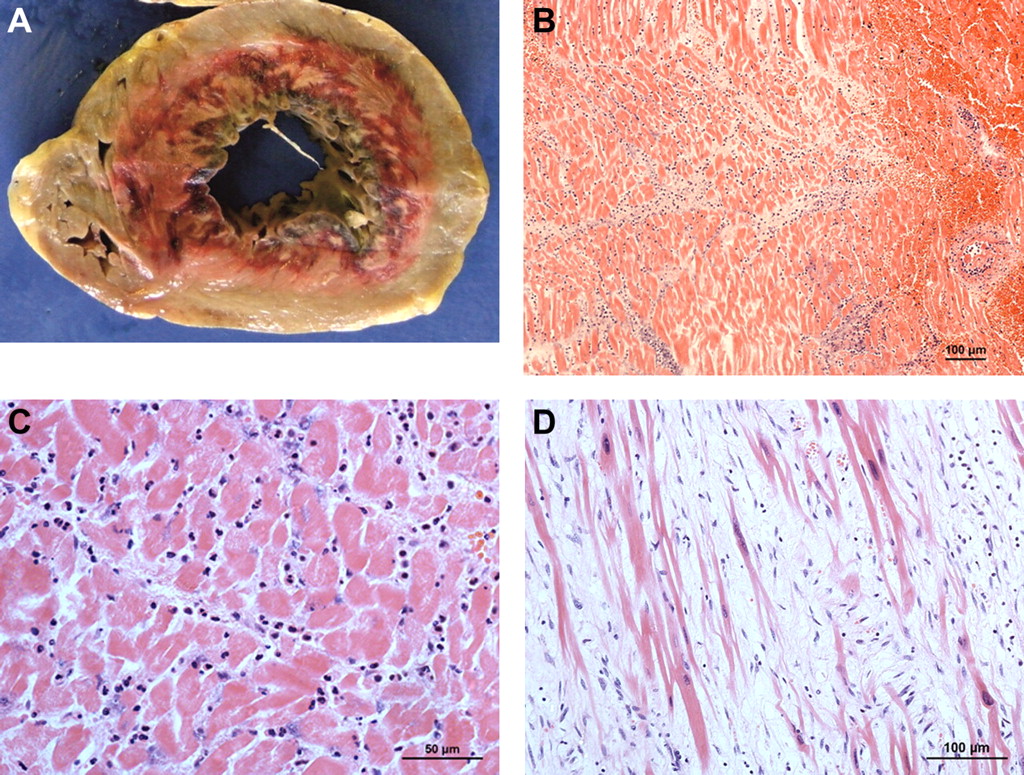
All 19 patients died suddenly. Twelve (63%) patients were found dead at home, mostly dying at rest (n=7). Two patients (cases 3 and 11) died within 12 h of strenuous exertion in sport. Images of the infarct post-exertion for case 11 are shown in figure 2; a macroscopic cross-section of the left ventricle (A) and a microscopic image of haemorrhagic reperfusion of the same infarct (B). The remaining cases died in the community (n=3), following hip replacement (n=1) or died in unknown circumstances (n=3) (table 1).
{kind=link}
{kind=link}
Acute myocardial infarction in a 17-year-old man after exertion. (A) Macroscopic mid-ventricular short-axis view of circumferential subendocardial infarction. (B) Haemorrhage reperfusion of an acute myocardial infarction (H&E, magnification 100×). (C) Infiltrate of neutrophils around necrotic myocytes in an infarct on days 3–7 (H&E, magnification 200×). (D) Granulation tissue with myocyte loss, pigmented macrophages and myofibroblasts are seen on days 7–42 (H&E, magnification 400×). This figure is produced in colour in the online journal—please visit the website to view the colour figure.
Patient demographics, circumstances of SCD, relevant medical history, location and timing of infarction
Antecedent symptoms, medical history and risk factors
Of the 19 cases, just over a quarter (n=5) had experienced one or more antecedent cardiac symptoms, including chest pain (n=4), shortness of breath (n=1) or palpitations (n=1). Risk factors were identified in the majority of cases (n=14, 68%) with some experiencing more than one risk factor (table 1). The most common association was alcohol consumption (n=5, chronic alcoholism n=2), of whom three patients also had a history of drug use (cocaine n=1, heroin n=1, cannabis n=1). Three patients had positive toxicology results (alcohol n=1, 80 mg/dl, morphine n=1, 0.012 mg/dl, cocaine n=1, positive for cocaine metabolites, quantity not specified). Both patients with a history of heroin use were hepatitis C positive. Other associated factors included exertion (n=2), epilepsy (n=2), oral contraceptive pill use (n=2), pregnancy (n=1), bronchitis (n=1) and phaeochromocytoma (n=1) (table 1).
Infarct characteristics
Location of infarct
The majority of the cases (n=9, 47%) had transmural infarcts located in the anterolateral region of the left ventricle supplied by the left anterior descending artery. Four infarcts (21%) were located in the posterobasal region of RCA territory. Two infarcts (11%) were transmural in both the RCA and left coronary artery territories, and four infarcts were subendocardial (21%).
Age of infarct
Eleven of 19 infarcts were estimated to be 24–48 h old, two infarcts were 3–7 days old (example in figure 2C) and three infarcts were 7–42 days old (example in figure 2D), while three cases had established regional fibrosis transmurally with no evidence of acute changes (cases 5, 13, 16). Five cases of acute infarction had evidence of established regional fibrosis within the myocardium in the same territory, indicating reinfarction (cases 3, 10, 11, 14, 17).
Discussion
Our study is to our knowledge the first large autopsy series on MI with completely normal coronary arteries. A previous study of ours examining non-atherosclerotic causes of SCD found six cases of infarction with normal coronary arteries.14 Our current study demonstrates that MI with normal coronary arteries is rare but is associated with a definite risk of mortality, presenting a contrast to reports suggesting a favourable prognosis. Our series suggest that MI with normal coronary arteries can occur in the territories of any single or multiple coronary arteries, similar to previous studies,15 16 with an effect on a predominantly younger population. While vasospasm cannot be confirmed as the underlying mechanism of infarction in postmortem hearts, several of the associated factors are linked to vasospasm, as is described below. Our cases illustrate several possible associations and multifactorial mechanisms,17 and a single aetiology does not appear to exist for this condition.
Most infarcts in our study were acute. However, our study also suggests that a proportion of patients have recurrent MI with normal coronary arteries.
Associated factors
Alcohol and drug use
Alcohol misuse is widespread in the UK.18 Epidemiological studies show higher rates of alcohol abuse in men younger than 40 years, with a first MI and higher rates of sudden death in heavy alcohol consumers.19 Ethanol generally induces vasodilation but can produce concentration-dependent coronary vasospasm in animal studies,20 subsequently confirmed in humans.21 With the increasing trend towards binge drinking this entity may become more prevalent. The role of cocaine in causing cardiovascular complications, including myocardial ischaemia and infarction, is well documented.22 Aslibekyan et al23 showed that 18–45 year olds had a significantly elevated prevalence of MI in association with cocaine use. Alcohol and cocaine can have synergistic or additive adverse effects on coronary artery blood flow.24 Marijuana is a rare trigger of acute MI, ventricular tachycardia and fibrillation by the induction of coronary artery spasm being reported in the background of other associations such as cigarette smoking, obesity and coronary artery disease.25 Two cases consumed alcohol and one case consumed cannabis within 12 h of death. As these infarcts were greater than 24 h in duration, this may indicate that a fatal arrhythmia may have been triggered by these substances in a heart already infarcting. A case report by Yu et al26 described MI after heroin injection with a normal coronary angiogram. It is possible that morphine usage in a detoxification programme in one further patient may have caused cardiac ischaemia by the same mechanism as heroin. However, this patient was also on an antipsychotic medication known to induce coronary vasospasm. In a cohort of schizophrenia, users of typical antipsychotic agents had a fivefold risk of MI compared with control subjects.27
Hypercoagulable state
Acute MI during pregnancy and puerperium is well documented, with the highest incidence occurring in the third trimester, as in case 2. Normal coronary arteries have been reported in 29% of cases.28 Coronary artery spasm associated with a probable hypercoagulable state is the most likely mechanism. Our patient also had a family history of hereditary haemorrhagic telangiectasia. Acute MI with normal coronary arteries in this disorder has been reported.29 It is well established that contraceptive medications thath include oestrogen increase the risk of vascular thrombosis.
Exertion
MI following strenuous exercise also featured in this study. Post-exercise ST elevation MI has been described.11 Physical exertion may precipitate epicardial coronary spasm related to an increased catecholamine output leading to arterial vasoconstriction and platelet aggregation.30 31
Adrenal tumours
Phaeochromocytoma identified in one patient in our series is a rare neuroendocrine tumour that can secrete high levels of catecholamines and has been linked to apical ballooning (or takotsubo syndrome) and may cause coronary vasospasm with infarction.32
Epilepsy
In a recent study, patients with epilepsy were at an increased risk of an acute MI, which may explain the sudden death of our patients with this condition. Epileptic seizures may induce cardiac ischaemia and increase the risk of subsequent acute MI in the absence of structural disease.33
Inflammation
Inflammation has been implicated in the pathogenesis of MI. C-reactive protein, an acute phase protein has been shown to be an independent predictor of future coronary events in apparently healthy individuals.34 Acute myocarditis and an inflammatory response to specific infectious agents, such as Epstein–Barr virus and Chlamydia pneumoniae have been proposed as a mechanism for acute coronary syndrome.35 36
Study limitations
Our autopsy series is a retrospective study and subject to the limitations of such studies, including reliance on information obtained from the referring pathologist and the coroner regarding epidemiological data and past medical history. A definite causative link between the risk factors and MI cannot be demonstrated and the presence of vasospasm can only be assumed in this study. It must also be stated that infarction as a result of spasm occurring within 24 h of the spasm may not be detected at autopsy.
Conclusion
Our autopsy series demonstrates a small but definite risk of mortality associated with MI and normal coronary arteries. Our study highlights that this entity can be fatal and its prognosis may be less favourable than currently considered. This autopsy series also demonstrates that the causation of MI with normal coronary arteries is complex and multifactorial. It suggests an association of this entity with a history of alcohol and/or drug use. However, studies such as ours rely on clinical information provided by referring pathologists. Only with complete clinical histories and investigations, including toxicology results, can we obtain better epidemiological data and identify the multifactorial causes more accurately.
Take-home messages
MI with normal coronary arteries is associated with a definite risk of mortality.
This study highlights its risk factors, particularly alcohol and/or drug use. With both being on the increase, this entity may be encountered more frequently in the future.
Interactive multiple choice questions
This JCP review article has an accompanying set of multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://jcp.bmj.com/education. Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into JCP with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Acknowledgments
The authors wish to acknowledge the charitable organisation, Cardiac Risk in the Young (CRY), for funding SVN.
References
Footnotes
Funding SVN is funded by a research fellowship grant from Cardiac Risk in the Young (CRY).
Competing interests None.
Ethics approval Ethics approval was granted by Brompton, Harefield and National Heart and Lung Institute REC: 07/Q0404/9 and 10/H0724/38.
Provenance and peer review Not commissioned; externally peer reviewed.