Altitude illness
BMJ 2003; 326 doi: https://doi.org/10.1136/bmj.326.7395.915 (Published 26 April 2003) Cite this as: BMJ 2003;326:915
- P W Barry, consultant paediatric intensivist (pwb1{at}le.ac.uk)a,
- A J Pollard, senior lecturer in paediatric infectious diseasesb
- a Department of Child Health, University of Leicester, Leicester LE2 7LX
- b Department of Paediatrics, University of Oxford, John Radcliffe Hospital, Oxford OX3 9DU
- Correspondence to: P W Barry
- Accepted 10 March 2003
As more people travel to high altitudes for economic or recreational purposes, altitude medicine has become increasingly important. Doctors may be asked to give advice to people planning an excursion to high altitudes or to help with patients while they themselves are travelling. Altitude illness should be anticipated in travellers to altitudes higher than 2500 metres, although for most it will be mild, and self limiting, and will not require the intervention of a doctor. Rarely altitude illness may progress to more severe forms, which can be life threatening. The best method of preventing altitude illness is to ascend slowly, allowing time for acclimatisation. The mainstay of treatment is descent, and drugs and other treatments should be used mainly to aid this.
Summary points
Altitude related illness is rare at altitudes below 2500 metres but is common in travellers to 3500 metres or more
The occurrence is increased by a rapid gain in altitude and reduced by a slow ascent, allowing time for acclimatisation
For most travellers, altitude related illness is an unpleasant but self limiting and benign syndrome, consisting chiefly of headache, anorexia, and nausea
More severe forms of illness including cerebral or pulmonary oedema may occur and may be fatal, particularly if not recognised
The treatment of altitude related illness is to stop further ascent and, if symptoms are severe or getting worse, to descend
Oxygen, drugs, and other treatments for altitude illness should be viewed as adjuncts to aid descent
Methods
We gathered the information in this review from several sources, including our own experience and reading of the relevant literature, supported by a search of the Cochrane database, a search of Medline by using the terms “altitude sickness” or “altitude,” and by consulting a specialist database of altitude related articles.1 We used two recently published texts (especially in regard to diagnosis), 2 3 and information from a recent course on high altitude medicine and physiology organised by ourselves and held at the National Mountain Centre, Plas Y Brenin, Wales. The research evidence in altitude medicine is scanty and hampered by differences between studies in ascent rates, environmental conditions, and definitions of illness. We therefore used observational studies and clinical experience to formulate recommendations.
Altitude illness
Three main syndromes of altitude illness may affect travellers: acute mountain sickness, high altitude cerebral oedema, and high altitude pulmonary oedema. The risk of dying from altitude related illnesses is low, at least for tourists. For trekkers to Nepal the death rate from all causes was 0.014% and from altitude illness 0.0036%.4 Soldiers posted to altitude had an altitude related death rate of 0.16%.5 In British climbers attempting peaks over 7000 metres, altitude related illnesses contributed to death in 17%.6
Risk factors for developing altitude illness include the rate of ascent, the actual altitude reached, the altitude at which the traveller sleeps, and individual susceptibility.w1 Box 1 shows definitions of altitude and associated physiological changes. Physical fitness is not protective,7 and exertion at altitude increases a traveller's risk of becoming unwell.w2 Genetic make up may also influence performance at altitude.8 Most pre-existing illnesses, such as chronic obstructive airways disease or diabetes, are not in themselves risk factors for developing altitude illness.
Box 1: Definitions of altitude and associated physiological changes
Intermediate altitude (1500-2500 metres)
Physiological changes detectable. Arterial oxygen saturation >90%. Altitude illness possible but rare
High altitude (2500-3500 metres)
Altitude illness common with rapid ascent
Very high altitude (3500-5800 metres)
Altitude illness common. Arterial oxygen saturation <90%. Marked hypoxaemia during exercise
Extreme altitude (>5800 metres)
Marked hypoxaemia at rest. Progressive deterioration, despite maximal acclimatisation. Permanent survival cannot be maintained
Acute mountain sickness
Figure 1 shows the reported incidence of acute mountain sickness at different locations.
Diagnosis —Acute mountain sickness consists of a constellation of symptoms in the context of a recent gain in altitude. These include headache; anorexia, nausea or vomiting; fatigue or weakness; dizziness or lightheadedness; and difficulty sleeping. These non-specific symptoms may be attributed to other conditions, especially by people who are anxious to stick to a preplanned schedule. Symptoms typically occur six to 12 hours after arrival at a new altitude (but may occur sooner) and resolve over one to three days, providing no further ascent is made. Acute mountain sickness is unusual at altitudes below 2500 metres. Peripheral oedema may be seen, but there are no physical signs that are diagnostic of acute mountain sickness, and the presence of neurological signs should imply the possibility of high altitude cerebral oedema or an alternative cause. Symptoms of acute mountain sickness can be quantified by using the Lake Louise scoring system,9 but this epidemiological research tool should probably not be used to direct the management of an individual case.
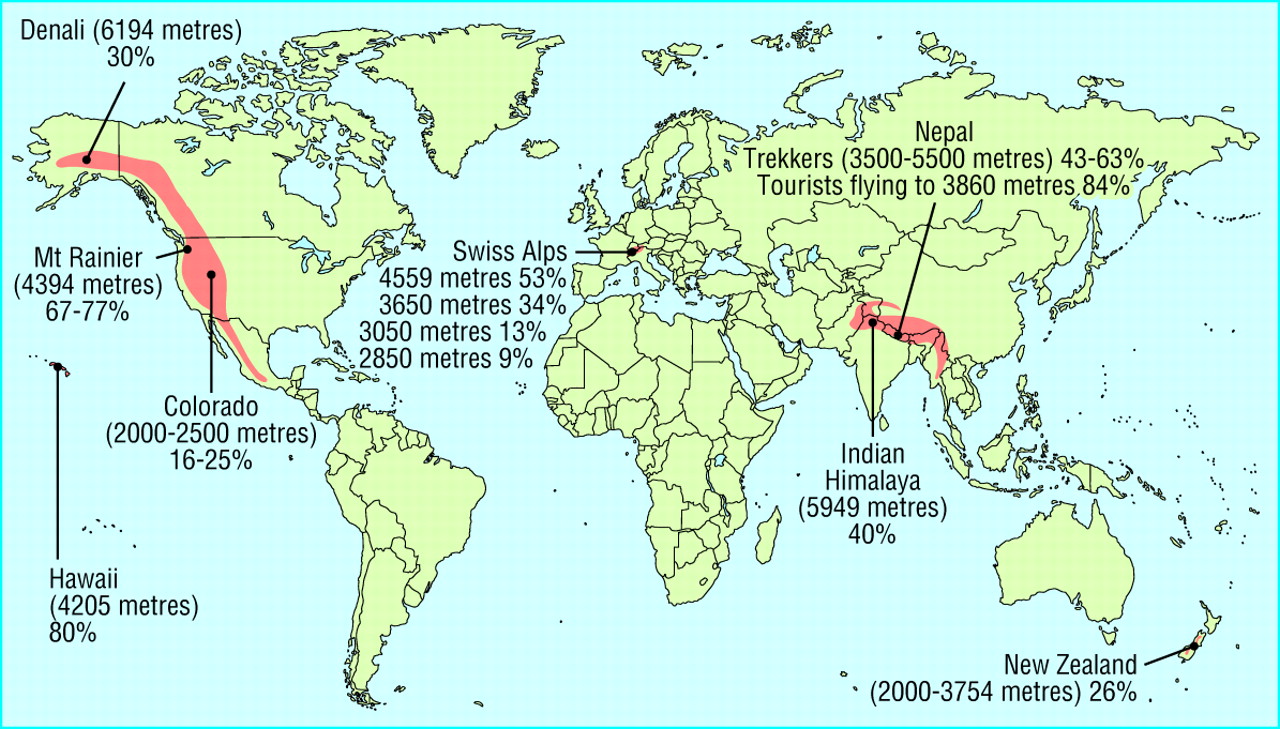
Global incidence of acute mountain sickness
{kind=link}
Pathophysiology
The pathophysiological processes that cause acute mountain sickness are unknown. However, symptoms of acute mountain sickness may be the result of cerebral swelling, either through vasodilatation induced by hypoxia or through cerebral oedema.3 Impaired cerebral autoregulation, the release of vasogenic mediators, and alteration of the blood-brain barrier by hypoxia may also be important.10 Similar mechanisms are thought to cause cerebral oedema at high altitude, which may represent a more severe form of acute mountain sickness.w1 Differences in individual susceptibility to acute mountain sickness are striking and inadequately explained. A reduced ventilatory drive in response to hypoxia may be important,3 as may an individual's relative volume of cerebrospinal fluid to brain tissue—people with relatively more cerebrospinal fluid are able to displace it to compensate for cerebral oedema.10
Treatment
Resting at the same altitude often relieves the symptoms of acute mountain sickness, and most patients will improve without treatment at the same altitude in 24–48 hours. 2 3 Simple analgesics and antiemetics may reduce headache and nausea in mild acute mountain sickness.w3 w4
A carbonic anhydrase inhibitor, acetazolamide, is effective in reducing the symptoms of acute mountain sickness, although the optimum dosage is unknown: 250 mg every eight hours is widely used and has been shown to be effective. Dexamethasone (8 mg initially, then 4 mg every 6 hours) may also be used to relieve symptoms.
The main principles of treating acute mountain sickness are to stop further ascent, to descend if symptoms do not improve over 24 hours or deteriorate, and to descend urgently if signs of high altitude pulmonary oedema or high altitude cerebral oedema occur.
Prevention
A body exposed to hypobaric hypoxia makes a series of adjustments, known as acclimatisation, that serve to increase the delivery of oxygen.11 Acclimatisation is best achieved by a slow ascent, allowing the body to adjust before going higherw5 and minimising the risks of succumbing to altitude related illness. This has led to recommendations for maximum rates of ascent (box 2). Slower ascent may be necessary for some individuals, but others may be able to ascend much faster without symptoms. A flexible itinerary is important, to allow days of rest without further ascent if needed.
Box 2: Acclimatisation and rates of ascent
Above 3000 metres increase your sleeping altitude by only 300–600 metres per day
Above 3000 metres take a rest day for every 1000 metres of elevation gained
Different people will acclimatise at different rates
If possible, don't fly or drive directly to high altitude
If you do go directly to high altitude by car or plane, do not overexert yourself or move higher for the first 24 hours
“Climb high and sleep low”
If symptoms are not improving, delay further ascent
If symptoms deteriorate, descend as soon as possible
A large part of acclimatisation takes place over the first one to three days at a given altitude, but the rate varies between different people. Full acclimatisation takes considerably longer. No reliable predictors for good acclimatisation exist, except that people tend to be consistent in how well they acclimatise on different trips.
Drug treatment may also be used for prophylaxis against acute mountain sickness.12 Acetazolamide has been recommended for people who are susceptible to acute mountain sickness or when ascent rates are unavoidably greater than those recommended.w6 Several randomised trials have shown a notable reduction in symptoms of acute mountain sickness with the prophylactic use of acetazolamide 250–500 mg twice a day. A recent meta-analysis concluded that acetazolamide 750 mg per day is efficacious in preventing acute mountain sickness but that lower doses are not.12 However, this analysis has been criticised for its choice of outcome variable and for analysing trials with different ascent rates together.w7 Lower doses of acetazolamide (125 mg twice a day) have been recommended to reduce symptoms while minimising side effects,w8 but the minimum effective dose remains unknown. If acetazolamide is used, treatment should be started at least one day before ascent and continued until adequate acclimatisation is judged to have occurred. Side effects, which include paraesthesia and mild diuresis, are common but usually well tolerated. Acetazolamide is a sulphonamide, and allergic reactions can occur.
Box 3: Treatment of altitude illness
Mild acute mountain sickness
Rest days, relaxation; consider descent
Aspirin, paracetemol, ibuprofen
Antiemetics may be useful
Acetazolamide may be considered
Severe acute mountain sickness and high altitude cerebral oedema
Descent, evacuation, oxygen
Dexamethasone
Pressure bag to facilitate descent
High altitude pulmonary oedema
Descent, evacuation, oxygen
Nifedipine
Pressure bag to facilitate descent
Altitude illness, type unknown
Descent, evacuation, oxygen
Dexamethasone
Nifedipine
Pressure bag to facilitate descent
Dexamethasone (4 mg every 6 hours) reduces the incidence and severity of acute mountain sickness at altitudes above 4000 metres.12 Lower doses or the same dose given every 12 hours are less effective.12 Prophylaxis may be started a few hours before ascent. Dexamethasone is not the first choice for the prophylaxis of acute mountain sickness because of its side effects. It may, however, be useful in people who have to ascend rapidly or who are predisposed to acute mountain sickness and are intolerant of or allergic to acetazolamide.
Box 4: Pre-existing medical conditions and altitude illness
Cardiac disease
The risk of ischaemic heart disease in previously well trekkers is not increased
Angina of effort at sea level is likely to worsen at altitude, and ascent to moderate altitude may precipitate angina in patients with previously stable coronary artery disease
Well controlled hypertension is not a contraindication to travel to altitude
Tests such as an electrocardiogram have no benefit in predicting potential problems at altitude
Echocardiography while the patient is breathing a hypoxic gas mixture will identify someone whose hypoxic pulmonary vascular response is brisk, but this test is not discriminatory for the development of altitude illness
Asthma
Asthma is generally unaffected by travel to altitude
There is no evidence that people with asthma are at greater risk of altitude illness than people without asthma
Some peak flow meters may be inaccurate at altitude
Chronic obstructive airways disease
Symptoms at sea level will be worse at altitude, and performance will deteriorate. Infectious exacerbations are a greater risk, so appropriate antibiotics should be carried and treatment started early
Patients with interstitial lung disease, such as cystic fibrosis, are at high risk of deterioration on travelling to altitude
Diabetes mellitus
Exposure to altitude in itself does not worsen diabetes
Symptoms of hypoglycaemia may be confused with high altitude cerebral oedema
Diabetic patients should have ready access to glucose supplements, and their companions should be aware of the symptoms and management of hypoglycaemia
Some blood glucose monitors may be inaccurate at altitude
Epilepsy
Altitude in itself does not increase the risks of seizures in patients with well controlled epilepsy
The consequences of an epileptic seizure may be more severe in a remote mountain area
Many other substances have been considered for preventing acute mountain sickness, supported by anecdote or, in a few cases, small randomised trials.12 Ginkgo biloba and aspirin are more effective than placebo in preventing symptoms of acute mountain sickness.w9 Evidence for the use of spironolactone is conflicting, and there is no convincing evidence for using nifedipine, furosemide (frusemide), or codeine in preventing acute mountain sickness.12
High altitude cerebral oedema
Diagnosis
High altitude cerebral oedema is usually preceded by acute mountain sickness and may lead to coma and death. Prodromal symptoms of early mental impairment or a change in behaviour may be ignored by patients and their companions. Headache, nausea and vomiting, hallucination, disorientation, and confusion are often seen; seizures are less common. Clinical signs include ataxia, a common early feature that may be disabling and is often the last sign to disappear during recovery; a progressive deterioration in concious level, proceeding to coma and death; and papilloedema and retinal haemorrhages. Focal neurological signs may occur, but in the absence of other signs and symptoms of cerebral oedema these should prompt consideration of other diagnoses.
Severe illness due to high altitude cerebral oedema may develop over a few hours, especially if the prodromal signs are ignored or misinterpreted, and may be accompanied by high altitude pulmonary oedema. Like acute mountain sickness, the incidence of high altitude cerebral oedema depends on the speed of ascent and the altitude reached, and is less than 0.001% for people travelling to 2500 metres and approximately 1% for lowlanders travelling to 4000–5000 metres.

High altitude pulmonary oedema and associated contributing factors. Adapted from Hornbein and Schoene.6
{kind=link}
Treatment
Anyone with symptoms of high altitude cerebral oedema should descend immediately. Delay may be fatal. Dexamethasone (8 mg initially, then 4 mg every 6 hours orally or parenterally) will usually relieve some symptoms, making evacuation easier. Similarly oxygen, if available, should be used as an aid to evacuation. Hyperbaric chambers improve oxygenation and relieve symptoms, making unaided descent easier.w10 w11 Even with descent, recovery may be delayed, and good supportive care is essential.
High altitude pulmonary oedema
Diagnosis
Symptoms of high altitude pulmonary oedema occur most commonly two to three days after arrival at altitude and consist of dyspnoea with exercise, progressing to dyspnoea at rest, a dry cough, weakness, and poor exercise tolerance.w12 As the disease worsens, severe dyspnoea and frank pulmonary oedema are obvious, with coma and death following. Early clinical signs include tachycardia and tachypnoea, mild pyrexia, basal crepitations, and dependent oedema. Patients with high altitude pulmonary oedema tend to have lower oxygen saturations than unaffected people at the same altitude, but the degree of desaturation by itself is not a reliable sign of high altitude pulmonary oedema.w13
High altitude pulmonary oedema rarely occurs below 2500 metres. Its incidence is 0.0001% at 2700 metres, increasing to 2% at 4000 metres. Speed of ascent, exercise during or immediately after ascent, male sex, youth, and individual susceptibility are all risk factors.
Pathophysiology
The pathophysiological cause of high altitude pulmonary oedema is still unknown, although several mechanisms have been proposed.3 Due to patchy pulmonary hypertension, stress failure occurs in capillaries of overperfused areas, leading to pulmonary oedema.w14 It is not clear whether the inflammatory mediators detected in the oedema fluidw12 reflect an underlying inflammatory cause or are a consequence of another process.
Recent work with people susceptible to high altitude pulmonary oedema indicates that deficiencies in clearance of alveolar fluid may also contribute to high altitude pulmonary oedema.13 Figure 2 shows the inherent characteristics and encountered stresses associated with high altitude pulmonary oedema.
Box 5: Children, pregnant women, and elderly people at altitude
Children
Altitude illness seems to have the same incidence in children as in adults, but the diagnosis may be delayed in children too young to describe their symptoms
Any child who becomes unwell at altitude should be assumed to be having altitude illness unless a clear alternative diagnosis is obvious
The principles of treatment are the same as in adults
Lowland infants taken to altitude are at risk of developing pulmonary hypertension and subacute mountain sickness (also called high altitude heart disease)
It remains unclear whether ascent to altitude increases the risk of sudden infant death syndrome
Pregnant women
There are very few data on the risks of travelling to altitude when pregnant
Studies from altitude residents indicate few differences in fetal oxygenation at altitudes below 3000 metres
Data from small studies and the experience of the airline industry indicate that exposure to normal aircraft cabin pressure or altitudes <2500 metres in later pregnancy (up to 37 weeks) is safe, provided that no other complications of pregnancy have occurred
There are very few data about pregnant lowlanders travelling to altitudes above 2500 metres
Conditions that reduce maternal oxygenation, such as altitude illness, carboxyhaemoglobin (exposure to cigarettes and fires), or other conditions impairing oxygen carriage, should be avoided or treated aggressively
Elderly people
The risk of altitude illness does not seem to increase with increasing age
Provided a traveller is fit, age in itself is not a barrier to travel
Exercise capacity and performance may be reduced and may also be affected by other medical conditions
Elderly patients should limit their activity during the first few days at altitude to allow acclimatisation to take place
Treatment
Descent is the mainstay of treatment. Descent of even a few hundred metres may be beneficial. 2 3 Supplemental oxygen should be given if available. Nifedipine is effective in preventing and treating high altitude pulmonary oedema in susceptible individuals (10 mg orally initially, then 20 mg slow release preparation ever 12 hoursw15 w16). A portable hyperbaric chamber has been developed that simulates descent. This consists of an airtight bag, which is pressurised by means of a manual pump. Continuous pumping is needed. The chamber may be claustrophobic, and lying down in it may worsen orthopnoea. Despite these problems the chamber remains popular and is carried by many larger expeditions.
Approaching an unconscious patient
In the field, a doctor may be called to the aid of a severely ill, comatose patient. The diagnosis of altitude illness can be supported by an appropriate history where available. The patient will almost certainly have some chest signs, and it can be difficult to know if the underlying illness is high altitude pulmonary or cerebral oedema, but this matters little, as the pragmatic management is the same: oxygen, dexamethasone 8 mg intravenously or intramuscularly, nifedipine slow release 20 mg, and hyperbaric treatment if available—and, most importantly, descent as soon as possible. Descent of even a few hundred metres may be life saving, and relays of porters, yaks, or ponies are all more likely to be available than a helicopter, which may take many hours to arrive. Box 3 lists types of treatment for altitude related illness.
Predicting altitude illness
Can doctors predict who is likely to develop altitude illness? An individual's past experience is in general a good guide, although there have been well documented exceptions. Otherwise, tests undertaken at sea level are disappointingly poor at predicting altitude illness. Level of fitness, simple measures of lung function, and vascular or pulmonary responses to hypoxia are all inconsistent in predicting individual susceptibility to altitude illness, 2 3 and small innovative studies have not as yet been confirmed in larger trials.14
Additional educational resources
Societies
Medical Expeditions (www.medex.org.uk/) is a research charity dedicated to investigating the mechanisms of altitude related illness. The organisation runs courses in high altitude medicine and physiology and from 2003 will be organising a diploma in mountain medicine
The International Society for Mountain Medicine (www.ismmed.org/) aims to encourage research and the dissemination of practical information about mountain medicine around the world
The International Mountaineering and Climbing Federation (UIAA; www.uiaa.ch/) is the umbrella society for climbing organisations
The Wilderness Medical Society (www.wms.org/) aims to improve scientific knowledge in matters related to wilderness environments and human activities in these environments
Journals and journal articles
High Altitude Medicine and Biology
Wilderness and Environmental Medicine
Bibliography of High Altitude Medicine and Physiology (http://annie.cv.nrao.edu/habibqbe.htm) lists 8600 references on high altitude medicine and physiology
Pollard AJ, Murdoch DR. The high altitude medicine handbook. Abingdon: Radcliffe Medical Press, 1998
Ward MP, Milledge JS, West JB. High altitude medicine and physiology2 is the definitive UK text for altitude medicine
Hornbein TF, Schoene RB. High altitude—an exploration of human adaptation3 contains a collection of detailed essays on the pathophysiology of altitude related disease
West JB. High life—a history of high altitude physiology and medicine. New York: Oxford University Press, 1998
Niermeyer, S. The pregnant altitude visitor. Adv Exp Med Biol 1999;474:65-77
Peacock AJ. Oxygen at high altitude. BMJ 1998;317:1063-6. (See also references 3, 11, and 16.)
Information for patients
Emedicine on line (www.emedicine.com/emerg/ENVIRONMENTAL.htm) is an online emergency medicine textbook with chapters on altitude illness
CIWEC Clinic Travel Medicine Center (http://ciwec-clinic.com/) provides information from Kathmandu on altitude illness and traveller's diarrhoea
The Himalayan Rescue Association (HRA; www.himalayanrescue.com/) is a voluntary organisation that aims to reduce casualties in the Nepal Himalayas
The High Altitude Medicine Guide (www.high-altitude-medicine.com/) provides current medical information for doctors and non-doctors on the prevention, recognition, and treatment of altitude illness
Pre-existing medical conditions and altitude illness
How should a practitioner advise a patient with a pre-existing chronic disease who wishes to travel to altitude? The research evidence to guide such advice is scanty, but in general is encouraging (box 4). Travellers should remember that access to medical care is difficult in many regions at high altitude. Adequate supplies of drugs should be carried, and itineraries should be selected that can offer escape routes if problems arise.
Special considerations arise in respect of children, pregnant women, or elderly people (box 5). Recommendations come largely from consensus documents or expert opinion. 2 3 15 16
Acknowledgments
We thank Jim Milledge and David Murdoch for their helpful comments on the paper and Brownie Schoene and David Murdoch for permission to reproduce figures.
Footnotes
-
Competing interests PWB has received reimbursement from Medical Expeditions, a UK charity that supports altitude research, for organising educational activities in the field of altitude medicine and physiology. He is also a member of MEDEX, a limited company that supports the activities of Medical Expeditions.
 Extra references and definitions appear on bmj.com
Extra references and definitions appear on bmj.com