Article Text

Statistics from Altmetric.com
Limiting certain aspects of inflammation may be a useful new treatment for sport related muscle injury
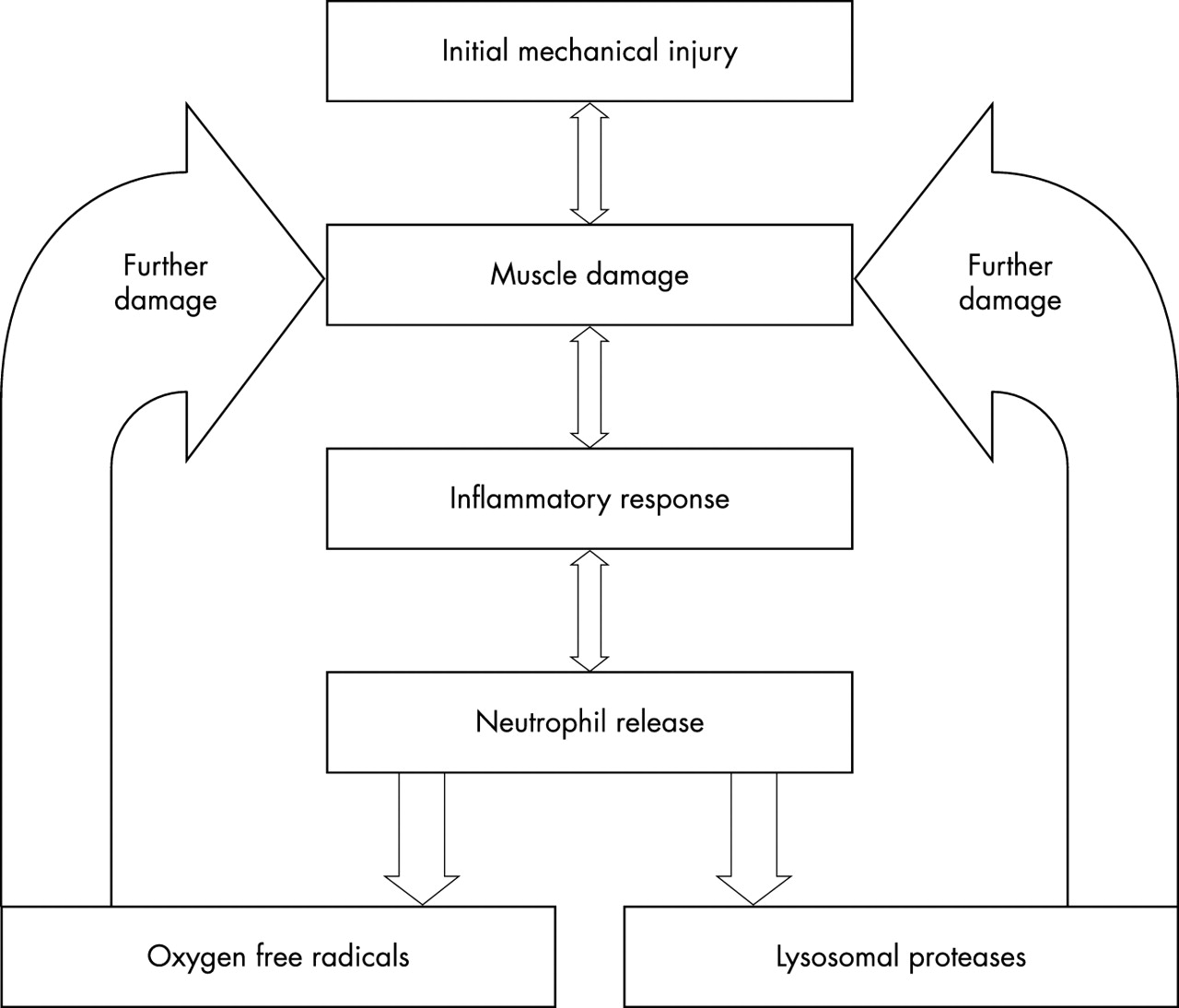
Muscle injury can occur through diverse mechanisms such as mechanical injury, muscular dystrophies, infectious diseases, and biochemical toxicities. Several types of skeletal muscle injury fall into the broad category of sport and exercise induced muscle injury. When exercise involves eccentric muscular contractions, it is associated with overloading of the contractile elements and connective tissues—that is, the force requirement of the muscle exceeds the habitual requirements—and can result in injury to skeletal muscle. It has traditionally been felt that the events following the initial injury, including inflammation, are necessary for optimal repair. The inflammatory response to eccentric exercise as well as stretch injury consist of neutrophilia, neutrophil activation, and the accumulation of neutrophils within the injured muscle as early as one to two hours. In this early inflammatory stage, cellular debris is removed by the infiltrating neutrophils and is followed by a regenerative response during which satellite cells proliferate to replace the previously damaged and phagocytosed muscle.1–4 In addition to phagocytosis, neutrophil invasion and activation can lead to the release of oxygen free radicals and proteases which potentially cause injury.5 Neutrophils contain more than 40 hydrolytic enzymes and toxic molecules in their granules and can generate various oxidants such as superoxide anion, hydrogen peroxide, and hypochlorous acid. The NADPH oxidase complex located on activated neutrophils and macrophages can initiate a “respiratory burst” which leads to production of superoxide anion, which can quickly be converted into hydrogen peroxide. In addition, myeloperoxidase, an enzyme present in neutrophils and macrophages, can generate hypochlorous acid, a highly reactive oxidising agent. Although the exact time course of the appearance of inflammatory cells and secondary muscle damage is debated, recent studies of single stretch injury have highlighted that peak damage occurs at the same time as maximum neutrophil invasion of the injured tissue,6,7 prompting the idea that neutrophils may somehow participate in causing injury (fig 1).
{kind=link}
Proposed mechanism of the relation between the inflammatory response to mechanical injury and further muscle damage. The initial mechanically induced damage produces myofibre tearing and inflammatory cell infiltration. Neutrophils may promote further damage through the release of oxygen free radicals and lysosomal proteases and elastases.
We will examine the relation between muscle injury and change in neutrophil concentration after both eccentric exercise and acute stretch injury. We will present evidence to suggest that invading leucocytes—that is, neutrophils and macrophages—exacerbate the initial mechanical damage. Although the clinical implications are not clear at this time, it is conceivable that limiting certain aspects of inflammation will present new treatment strategies for sport related muscle trauma. Perspectives for rational approaches to handle the development of muscle injury during neutrophil inflammation are considered.
MUSCLE INFLAMMATION AND CHANGE IN NEUTROPHIL CONCENTRATION AFTER REPEATED ECCENTRIC EXERCISE
There is a ubiquitous host response to various types of skeletal muscle injury.8,9 Neutrophils are the first subpopulation of leucocytes to appear at the injury site.10 They are produced in the bone marrow and circulate in the bloodstream, representing 50–60% of the total circulating leucocytes. Neutrophils constitute the first line of defence against infectious agents or non-self substances that penetrate the body’s physical barriers.
Studies on whether neutrophils participate only in phagocytosis or also promote muscle injury after modified musculoskeletal loading use different injury methods and rely on various variables to assess such injuries. Nevertheless, inflammatory cell infiltration after repeated eccentric contractions has been well established in both human and animal models.2,11,12 Stretch of activated skeletal muscles—that is, eccentric or lengthening contraction induced muscle injury—involves a variety of histopathological changes, including swelling of muscle cells, loss of the intermediate filament proteins desmin and dystrophin, and inflammatory cell infiltration.13 Repeated eccentric contractions of skeletal muscle can lead to an immediate loss of isometric force production that is the result of excitation/contraction uncoupling and damage to force producing or transmitting structures.14 This initial strength loss is followed by the so called “secondary damage” phenomenon,9 which many now consider to result from, among several possibilities, inflammatory cell mediated processes.
Clinical studies have supported the notion that there is an associated neutrophilia and secondary damage associated with repeated eccentric contractions. Saxton et al15 showed that the total leucocyte count was increased within four hours of repeated eccentric contraction and bench stepping exercise, but had returned to pre-exercise levels 24 hours later. This increase in total leucocyte count was attributed to changes in the numbers of circulating neutrophils. Previously Pizza et al16 measured blood neutrophil concentrations in humans during early recovery (<24 hours) from two bouts of eccentric exercise. The exercise bouts were separated by four weeks. Neutrophil concentrations were significantly higher three, six, and nine hours after exercise for the first bout than the second bout. The isometric strength deficit was significantly greater for bout 1 than bout 2 six, nine, and 24 hours after exercise. These data suggest that the neutrophilia associated with novel eccentric arm exercise precedes secondary changes in isometric strength and, furthermore, point to the possibility that invading neutrophils are linked to the secondary damage process which has been observed both clinically and in animal studies.
MUSCLE INFLAMMATION AND CHANGE IN NEUTROPHIL CONCENTRATION AFTER STRETCH INJURY
In animal models of single stretch injury, there appears to be a decline in muscle function that persists for 24 hours after injury.17 Recently, it has been shown using monoclonal antibodies that peak neutrophil invasion of stretch injured muscle occurs over the time course.7 This observation is true regardless of the amount of initial mechanical damage.7 Moreover, this study noted for the first time an absence of monoclonal antibody specific macrophages, suggesting that, in certain animal models, macrophages may not be involved in muscle regeneration and repair.7 In another study from the same laboratory, peak levels of oxygen free radicals were measured within the muscle 24 hours after injury.6 Similarly, muscle fibre tearing increases locally at the site of injury over the first 24 hours.6 Collectively, these studies suggest that a relation exists between neutrophil infiltration and degree of damage to stretch injured skeletal muscle. Moreover, these observations suggest that a valid target for attenuating muscle fibre damage may be to block neutrophil derived oxygen free radical production.
DO NEUTROPHILS CAUSE EXERCISE ASSOCIATED MUSCLE INJURY?
In the last decade, major advances have been achieved in understanding the possible mechanisms of neutrophil mediated tissue damage. Muscle injury by inflammatory cells has been examined most thoroughly in experimental models of muscle ischaemia followed by reperfusion, in which neutrophils have been clearly shown to promote muscle fibre damage during the reperfusion phase.18–20 It is clear from non-exercise models, in particular ischaemia-reperfusion studies, that increased neutrophil adhesiveness to the endothelium is a critical early step in the sequence of events leading to muscle damage.21 Furthermore, there is very strong evidence that polymorphonuclear leucocytes (particularly neutrophils) and oxygen free radicals are key mediators of ischaemia related tissue injury.18–20 After ischaemia, local leucosequestration of activated neutrophils occurs, with generation of reactive oxygen species,22 leading to the hypothesis that endothelial and subendothelial damage are caused by neutrophil derived oxidants.23 Animals rendered leucopenic develop less damage and less oxidant production during the reperfusion phase.24
On the basis of the observed time course for neutrophil infiltration and degree of injury,7 the hypothesis that neutrophils play a role in stretch injury has been investigated. Using an antibody that blocks the neutrophil’s respiratory burst, it has been shown that the degree of myofibre damage can be considerably reduced 24 hours after injury.25 Moreover, there is preservation of the intermediate filaments desmin and dystrophin, suggesting that oxygen free radicals may operate directly on these proteins. Although the consequences of these observations are unknown for human muscle injury, they parallel similar in vitro experiments showing that neutrophils can injure skeletal myotubes and may indicate that neutrophils exacerbate injury16 and or/delay regeneration.26 These findings may be species specific, however, as rat ankle dorsiflexor muscles submitted to in situ lengthening contractions do not show evidence of accumulation of neutrophils after activity.27 Furthermore, others have shown that passive stretch and isometric contractions can elevate neutrophil concentrations without causing overt signs of injury.10
CLINICAL IMPLICATIONS
From the above discussions, it appears that blocking neutrophil recruitment may limit the amount of damage that occurs in various models of muscle injury. Although we do not understand the precise mechanism, it appears that neutrophils may cause damage by release of oxygen free radicals.25 Furthermore, we now have evidence (unpublished results) that neutrophil derived free radicals target the proteins desmin and dystrophin, which are intermediate filament proteins important in regulation of muscle contraction.
To manipulate the host inflammatory response and attenuate the potentially negative consequences of inflammation, investigators have used animal models to examine the effects of non-steroidal anti-inflammatory drugs on muscle injury. Early studies suggested that they may reduce the decline in the muscle’s tensile strength after injury.28 In a similar study, rabbits treated with piroxicam showed an earlier recovery of muscle contractile force; however, no significant differences were observed at any other time period between treated and untreated animals.29 According to Mishra et al,30 flurbiprofen administration to rabbits produced more complete functional recovery three and seven days after repeated bouts of eccentric contractions. However, the same animals showed a deficit in torque and force generation at 28 days. In addition, flurbiprofen administration resulted in preservation of the intermediate filament protein desmin. Early in the recovery period, there was a dramatic increase in the regenerative response, which persisted until seven days. It was argued that flurbiprofen may have delayed the muscle’s regenerative response. Although a definitive study has not been performed, these data argue that non-steroidal anti-inflammatories, which can attenuate neutrophil activity, may lead to delayed recovery and functional losses in animal models of muscle injury.
CONCLUSIONS
Neutrophils and macrophages play a role in muscle damage after repeated eccentric exercise and acute stretch injury. However, contrary to conventional thinking, it is possible that certain aspects of neutrophil function cause damage to healing muscle or delay its regenerative capabilities. Because neutrophils can release oxygen free radicals during phagocytosis, it is possible that neutrophil derived oxidants exacerbate pre-existing muscle injury in vivo by damaging previously uninjured muscle.10 These findings suggest the possibility that innovative treatment strategies directed at specific functions of the neutrophil are theoretically possible to improve recovery from muscle injury. Pharmacological intervention may be better targeted against specific aspects of neutrophil function such as free radical production, while maintaining the steps necessary for phagocytosis and removal of cellular debris. This possibility is being investigated.
Limiting certain aspects of inflammation may be a useful new treatment for sport related muscle injury