Article Text

Statistics from Altmetric.com
Introduction
The world governing body of football, Fédération International de Football Association (FIFA), was established in 1904 and currently has 208 member associations from around the world. There are 300 million active, registered, football players, referees, coaches, medical and paramedical personnel as well as administrators, and hundreds of thousands of organised matches are played every weekend around the globe. The popularity of the game is increasing, with the FIFA World Cup as the biggest single sporting event drawing the attention of millions of fans. Cumulatively, 30 billion TV spectators watched the 64 matches of the last FIFA World Cup South Africa 2010. Football players at all levels of play try to mimic the way the top teams present at the highest competitions.
FIFA's Medical Assessment and Research Centre (F-MARC) was established in Zurich in 1994 to provide scientific evidence to protect the players' health, to reduce or prevent football injuries, and to promote football as a health-enhancing leisure activity—at that time a unique initiative of a sport's governing body.
Osteoarthritis and football
The current body of literature regarding osteoarthritis and football is far from complete. About 30 years ago, Klünder et al1 reported that osteoarthritis of the hip was significantly more frequent in retired football players than in controls. Similarly, Lindberg et al2 found osteoarthritis of the hip in 5.6% of former football players compared with 2.8% in controls. If only elite football players were regarded, the prevalence was 14%. Shepard et al3 found that ex-professional football players have an increased prevalence of osteoarthritis of the hip (13%) compared with age-matched controls (1.5%). In a survey on long-term health impacts of playing professional football in the UK,4 about half of the respondents reported to have an osteoarthritis diagnosis in at least one anatomical site, with the knee being the most commonly affected side. Drawer and Fuller5 found a 32% prevalence of osteoarthritis in at least one of the lower limb joints, and the knee more often affected than the hip or ankle. Roos et al6 reported a prevalence of gonarthrosis of 16% in elite football players, 4.2% in non-elite players and 1.6% in controls. Knee injury is a major risk factor for the development of gonarthrosis.6,–,9 Drawer and Fuller5 reported that 47% of former professional football players retired due to an acute or chronic injury primarily of the knee but also of the ankle, hip and lower back. Therefore, the injury prevention is of great importance. F-MARC identified the following entry point for preventive measures:
▶ optimal preparation of players for training and matches;
▶ adaptation of the Laws of the Game to reduce the incidence with the highest propensity of causing injuries;
▶ early diagnosis of minor cartilage injuries;
▶ state-of-the-art treatment of cartilage injuries.
Exercise-based programmes to reduce football injuries
After a detailed risk factor analysis and initial studies on the prevention of football injuries, F-MARC in cooperation with a group of experts developed a preventive programme for amateur and recreational players10 11: ‘The 11’. This programme consisting of 10 simple exercises and the promotion of Fair Play (http://www.FIFA.com/medical). In Switzerland and New Zealand, ‘The 11’ was implemented in cooperation with the national health insurance company and the national football association as a country-wide campaign. In Switzerland, the implementation and the effects of the campaign were evaluated by an independent research group.12 Over 2 years, a total of 5549 coaches for amateur players were instructed to perform ‘The 11’ in their training sessions. Teams who regularly performed the prevention programme, ‘The 11,’ had an 11.5% lower incidence of match injuries and a 25.3% lower incidence of training injuries than other teams.12 The results showed impressively that football injuries could be reduced, even on a nationwide level (figure 1).

Percentage of change in the incidence of match (grey columns) and training (black columns) injuries in the players who did and those who did not perform ‘The 11’ prevention programme (data from Junge et al12).
Based on the experience with ‘The 11’ and other preventive programmes, such as ‘Prevention Enhance Performance’,13 a comprehensive warm-up programme ‘The 11+’ was developed. In collaboration with the Oslo Sports Trauma Research Centre (Norway), ‘The 11+’ was evaluated for its efficacy in preventing football injuries in a cluster randomised controlled trial.14 In the intervention group who performed ‘The 11+’ programme throughout one season, the injury rate was 30–50% lower than in the control group who continued their usual warm-up (figure 2).14

Incidence of match and training injuries per 1000 exposure hours in the players who did (grey columns) and those who did not (black columns) perform ‘The 11+’ prevention programme (data from Soligard et al14).
Injury prevention in FIFA competitions
Starting with the FIFA World Cup 1998, F-MARC implemented a standard injury surveillance study for all FIFA competition. Thanks to the team physicians' excellent compliance, a 95% response rate and good-quality data were obtained.15 16 With the 2010 FIFA World Cup in South Africa, 43 FIFA competitions with a total of 1321 matches (or 43 609 individual player hours) have been surveyed, including four consecutive FIFA World Cups for men, three for women and three Olympic Games. On average, the incidence of injuries was 2.4 injuries per match or 76 injuries per 1000 playing hours; one injury per match resulted in time loss (figures 3, 4).
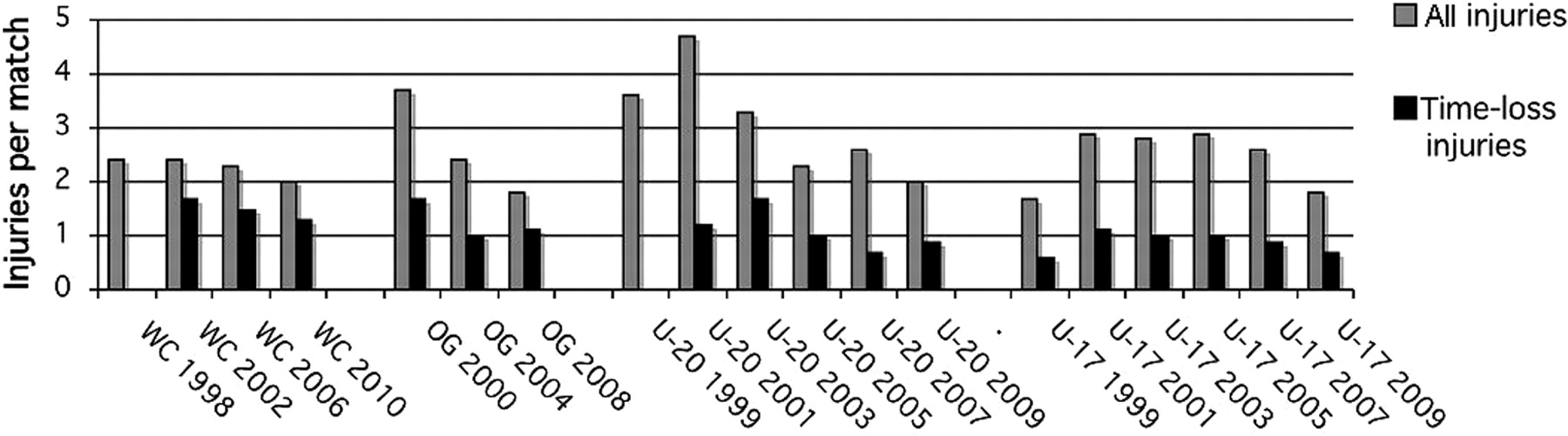
Injuries per match in competitions for male players (grey columns, all injuries; black columns, time-loss injuries). OG, Olympic Games; U-17, FIFA U-17 World Cup; U-20, FIFA U-20 World Cup; WC, FIFA World Cup.
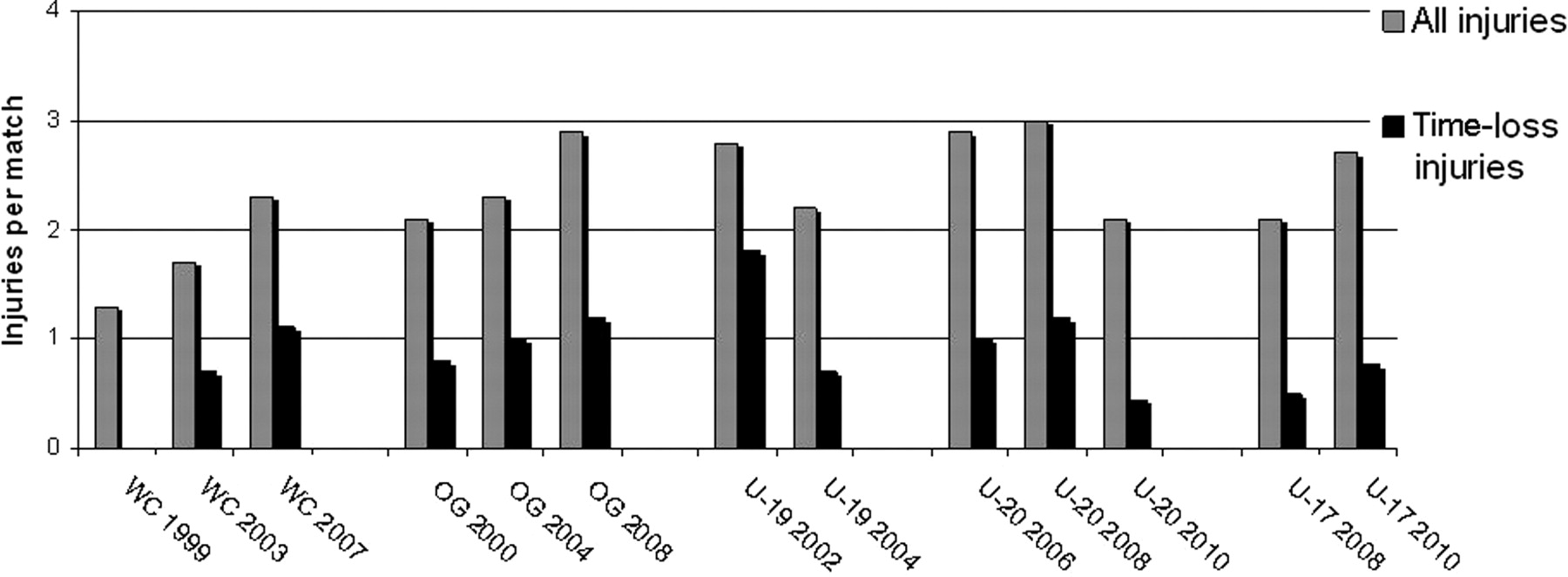
Injuries per match in FIFA competitions for female players (grey columns, all injuries; black columns, time-loss injuries) (OG, Olympic Games; U-17, FIFA U-17 Women's World Cup; U-19, FIFA U-19 Women's World Cup; U-20, FIFA U-20 Women's World Cup; WC, FIFA Women's World Cup).
In all FIFA competitions for male players, the number of injuries per match (and especially of time-loss injury) is declining (see figure 3), while in female competitions the opposite trend is observed (figure 4). The most dominant decline has been observed in the men's U-20 competitions. During the 2010 FIFA World Cup South Africa, the incidence of injuries rate was significantly lower than the average of the three previous World Cups,17 and also the incidence of time-loss injuries was lower than in any of those competitions (figure 3). Interestingly, fewer injuries during the 2010 World Cup South Africa (64%) were caused without contact with another player than in 2002 or 2006 (both 73%), and fewer contact injuries were caused by foul play based on the judgement of the team physician (2010: 23%; 2006: 61%; 2002: 51%).17 A possible reason might be the strict application of the ‘Laws of the Game’, following the recommendation of the International Football Association Board to reduce or eliminate the incidence of events with the highest propensity of causing injuries, in particular tackling from behind, two-footed tackles and elbow-to-head kicks.18 As those incidents are punished by red card, they almost disappeared from the field. Education of the coaches and players is crucial in this respect.
In international competitions for top-level female players, especially in the FIFA World Cup, Olympic Games and the FIFA U-17 World Cup, an increase in the injury rate is observed (see figure 4), most probably because female football at the highest level becomes faster and more physical.
Early diagnosis of cartilage injuries
Cartilage injury in the athletic population has been diagnosed in 40% of professional athletes (n=931) in comparison with 16% in the general population.19 Untreated cartilage defects in the initial stage might have a limited impact on the sporting activities; however, the mild or moderate symptoms (pain) might be reduced by consumption of painkillers or non-steroidal anti-inflammatory drugs (NSAIDs). The use of medication during eight FIFA World Cups has been analysed and revealed a high intake of painkillers and especially of NSAIDs.20 21 During the 2002 and 2006 World Cups, 4450 medical prescriptions were reported, and the most common was NSAID (n=2092) (see figure 5). More than half of the players took these at least once during the tournament, and 10% took them prior to every match. In the other FIFA competitions, on average 0.6 medical prescriptions were taken per player per match, and NSAIDs were the most common type of medication. Players in the FIFA Women's World Cups had the highest percentage of using NSAID per match (30.7%); however, in the FIFA U-17 World Cups, 17.3% of players were using NSAIDS and 21.4% of the players in the FIFA U-20 World Cups (figure 6).
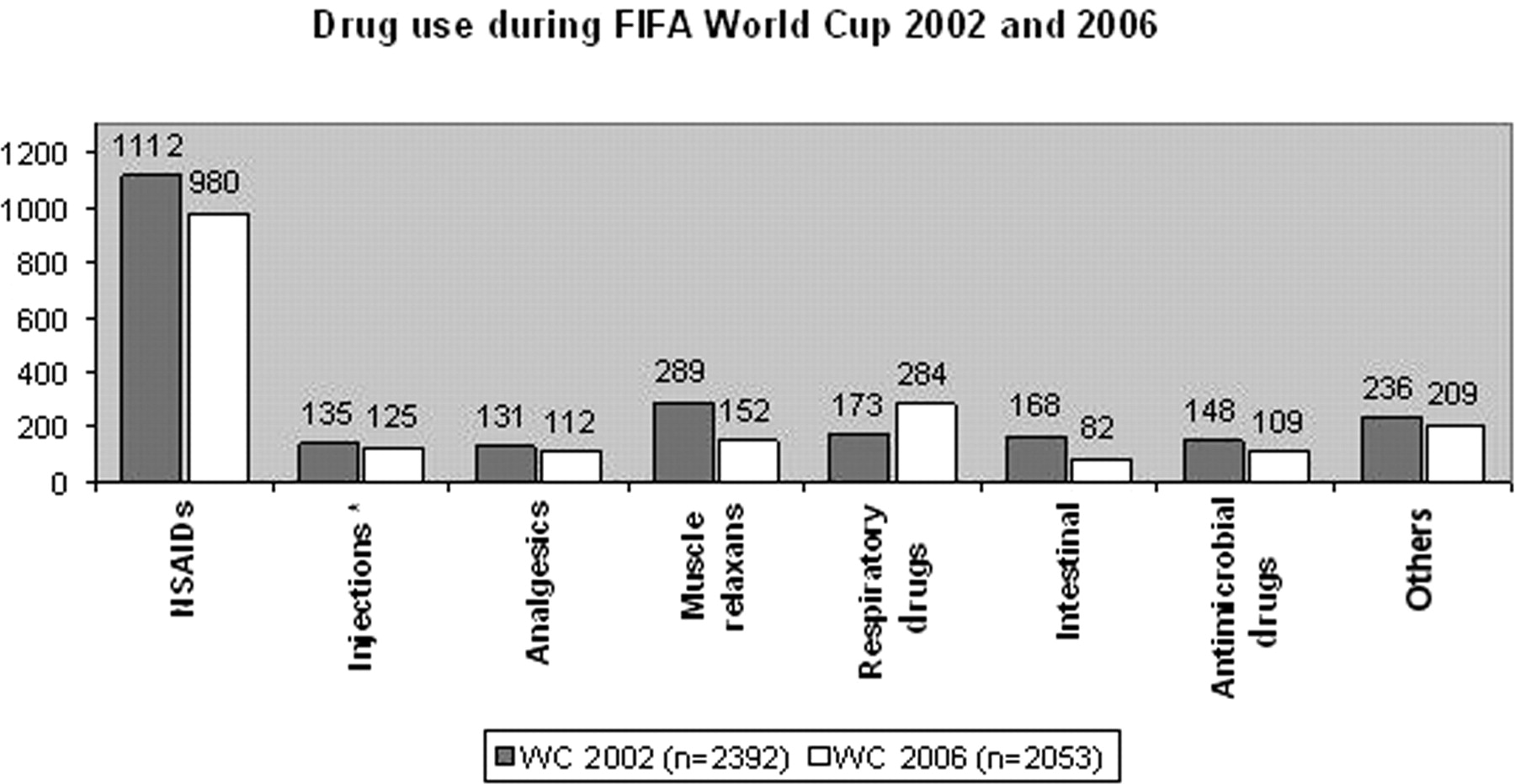
Medication use during the 2002 and 2006 FIFA World Cups (figure from Tscholl et al20).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of players using medication prior a match during FIFA World Cups (data from Tscholl et al21).
These findings highlight the existing problem of excessive medication use in international top-level female and male football players. The results are alarming, and further steps should to be taken to understand the reasoning behind the sports physicians' practice and also to plan educational programmes to avoid the abuse of prescription medication. Currently, it can only be hypothesised that the players are taking the medication to reduce the symptoms of small lesions in the joints and to allow them to play pain-free at a high professional level. Research into the early onset of osteoarthritis in sports and in particular the most popular sport, football, should include an early diagnosis of small cartilage lesions in the joints which might be treated and reduce the later onset of osteoarthritis.
Acknowledgments
JS Blatter, FIFA President, is thanked for supporting the research activities as an integrated part of development of the game and as social and cultural involvement. A Junge and C Fuller are thanked for their intellectual input and continuous research activities within F-MARC over the past 12 years.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.