Article Text

Statistics from Altmetric.com
- CFI, collateral flow index
- CFR, coronary flow reserve
- CVP, central venous pressure
- LAD, left anterior descending
- Pao, aortic pressure
- Poccl, occlusive pressure
Cardiovascular disease, in particular coronary artery disease (CAD), is the leading cause of death in industrialised countries. Current therapeutic approaches to obstructive CAD include pharmacologic reduction in myocardial oxygen demand or mechanical restoration of blood flow to regions with insufficient blood supply. Alternatively, recent investigations have focused on the growth of vascular communications between different coronary artery regions. In principle, vessel growth occurs by the formation of a primary plexus of vessels by angioblasts (vasculogenesis), by sprouting of endothelial cells leading to a new capillary network (angiogenesis), or by the transformation of pre-existing collateral arteriolar pathways into conducting vessels (arteriogenesis).1 In occlusive CAD, angiogenesis takes place in the presence of myocardial ischaemia while the remodelling process of arteriogenesis is related to enhanced shear forces at the vessel wall in response to increased flow through pre-existing collateral connections.2 Theoretically, this renders physical exercise an ideal therapeutic option for inducing arteriogenesis, since cardiac output, and thus coronary flow, is elevated along the arterial branches of the coronary circulation.3 In humans without stenotic coronary arteries, it has recently been shown that there can be functional anastomoses between different vascular territories.4 However, proof of the arteriogenic potential of physical exercise is lacking.
The purpose of this cardiac invasive follow up study, in an entirely healthy male volunteer, was to investigate whether a programme of physical endurance exercise could increase directly obtained coronary collateral flow.
METHODS
The subject of this study was a 46 year old healthy male cardiologist (CS) with no cardiovascular risk factors. The subject has been an amateur long distance runner for 25 years. He volunteered to be included in an invasive study on the effect of a long term physical endurance exercise programme on collateral flow among patients with coronary artery disease. That study was approved by the local ethics committee. So far, there was no history of any serious illness in the study subject. The cardiac non-invasive and invasive examinations described below were performed during three phases: low physical fitness (baseline of two hours of aerobic endurance training per week, continuously); intermediate fitness (four hours training per week for four months); and high physical fitness (8–9 hours training per week for four months). There was a baseline examination in May 1999, one during preparation for a marathon run (Berlin Marathon 2000; 42.2 km, flat topography), and one shortly after the finish of an alpine ultramarathon run (Swiss Alpine Marathon, Davos 2002; 78.5 km, with a 2300 m difference in altitude). The three examinations each comprised: Doppler echocardiography; bicycle spiroergometry with measurement of heart rate, blood pressure, peak exercise capacity (in watts (W)) and maximum oxygen uptake (ml/min/kg); and coronary angiography with measurement of hyperaemic coronary flow reserve (CFR). Collateral flow index (CFI), which is the collateral flow obtained during vascular balloon occlusion relative to normal antegrade flow during vessel patency, was assessed during intermediate and high physical fitness.5 Biplane coronary angiography was performed via the right femoral artery. Aortic pressure (Pao) was recorded using a 6 French guiding catheter for percutaneous transluminal coronary angioplasty. Central venous pressure (CVP) was directly measured only once (5 mm Hg). CFR was obtained using a 0.014 inch, 20 MHz Doppler tipped angioplasty guidewire. Following intracoronary injection of 200 μg of glyceryl trinitrate, CFR was determined by measuring maximum flow velocity in the mid left anterior descending coronary artery (LAD) after bolus injection of 18 μg of intracoronary adenosine, and dividing it by the baseline flow velocity without adenosine. CFI to the entirely normal LAD relative to normal antegrade blood flow was determined by simultaneous measurements of mean Pao and mean distal coronary occlusive pressure (Poccl) obtained via a 0.014 inch sensor tipped pressure guidewire (PressureWave, Jomed, Switzerland)), at the end of a one minute balloon occlusion: CFI = (Poccl−CVP) / (Pao−CVP) (fig 1).

{kind=link}
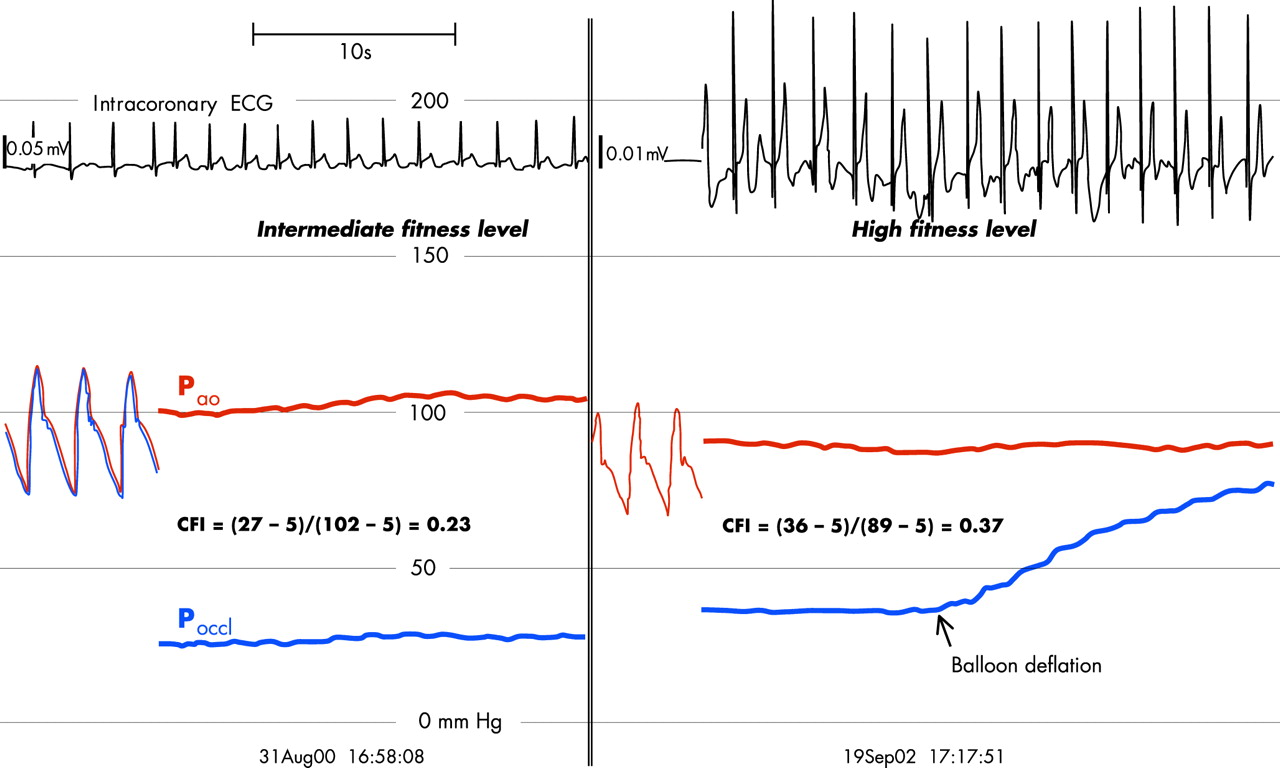
Collateral flow at intermediate fitness (left panel) and at high fitness level (right panel). Intracoronary ECG lead recordings are shown in the upper part of the panels. On the left side of both panels, phasic aortic pressure tracings are shown; on the right side mean aortic (upper curve, Pao = 102 and 89 mm Hg, respectively) and mean coronary occlusive (lower curve, Poccl = 27 and 36 mm Hg, respectively) pressure tracings at the end of a one minute coronary artery balloon occlusion at 1 atm inflation pressure. The calculation of CFI is shown for both examinations during intermediate and high fitness level (CVP = 5 mm Hg; measured non-simultaneously).
RESULTS
The study results are depicted in table 1 and fig 1. Coronary angiography was normal. CFI increased by more than 60%, 0.23 at intermediate to 0.37 at high fitness level (fig 1). During the one minute LAD occlusion, the study subject felt chest pain at intermediate but not at high fitness level.
Results of study
DISCUSSION
For the first time in a human being with entirely normal coronary arteries we have shown evidence of enhanced coronary collateral flow in response to an endurance exercise programme. This augmentation of flow across preformed coronary communications goes along with an improvement in the maximally obtainable coronary flow velocity (that is, the CFR), which suggests that elevated vascular shear forces may have been related to the increased collateral flow. It can be taken for granted that exercise induced myocardial ischaemia and thus angiogenesis (versus arteriogenesis) have not been involved in the development of improved collateral flow; this is because it was obtained in a healthy individual with normal cardiac and coronary anatomy and function who had never suffered anginal chest pain before experiencing this kind of discomfort during the first one minute balloon occlusion. Therefore, remodelling of pre-existing collateral vessels (arteriogenesis) proves possible even in the face of normal coronary circulation. This provides an important incentive for clinical studies using exercise as an arteriogenic intervention in patients with CAD.