Article Text

Abstract
Objective To evaluate a potential reduction in injury related healthcare costs when using the ‘11+ Kids’ injury prevention programme compared with a usual warmup in children’s football.
Methods This cost effectiveness analysis was based on data collected in a cluster randomised controlled trial over one season from football teams (under-9 to under-13 age groups) in Switzerland. The intervention group (INT) replaced their usual warmup with ‘11+ Kids’, while the control group (CON) warmed up as usual. Injuries, healthcare resource use and football exposure (in hours) were collected prospectively. We calculated the mean injury related costs in Swiss Francs (CHF) per 1000 hours of football. We calculated the cost effectiveness (the direct net healthcare costs divided by the net health effects of the ‘11+ Kids’ intervention) based on the actual data in our study (trial based) and for a countrywide implementation scenario (model based).
Results Costs per 1000 hours of exposure were CHF228.34 (95% CI 137.45, 335.77) in the INT group and CHF469.00 (95% CI 273.30, 691.11) in the CON group. The cost difference per 1000 hours of exposure was CHF−240.66 (95%CI −406.89, −74.32). A countrywide implementation would reduce healthcare costs in Switzerland by CHF1.48 million per year. 1002 players with a mean age of 10.9 (SD 1.2) years participated. During 76 373 hours of football, 99 injuries occurred.
Conclusion The ‘11+ Kids’ programme reduced the healthcare costs by 51% and was dominant (ie, the INT group had lower costs and a lower injury risk) compared with a usual warmup. This provides a compelling case for widespread implementation.
- children
- football
- soccer
- injury prevention
- FIFA 11+ Kids
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
A physically active lifestyle and active participation in sport at a young age can promote lifelong healthy active behaviour.1–3 Football (soccer) is one of the most popular sports worldwide, and a suitable physical activity setting for children.4 Although there are many health benefits of sport participation, sport is the main cause of injury in children and adolescents.5–9 Injuries in young athletes can reduce current and future involvement in physical activity and lead to substantial healthcare and societal costs.10 11 This economic burden associated with injury involves medical, financial and human resources at many levels.11–13
The football specific warmup and injury prevention programme, ‘11+’, prevents injuries in recreational youth football.14–17 There is, however, a dearth of data on sport injury prevention in children.18 Based on our epidemiological data,19 20 we developed and evaluated an injury prevention programme for children’s football (‘11+ Kids’).21 In a randomised controlled trial, this warmup programme reduced the overall injury risk in children’s football by 48% and the risk for severe injuries by 74%.22 Here we report the cost effectiveness study that ran alongside that randomised controlled trial.22
Our cost effectiveness analysis compared direct healthcare costs of the ‘11+ Kids’ intervention group with costs in a control group who undertook their usual warmup.22 The intervention was investigated from a societal perspective, considering all relevant costs and effects, regardless of who pays or who benefits from the effects.
Methods
Sample, design and data acquisition
We followed the CHEERS statement for the reporting of this cost effectiveness analysis.23 Study participants were boys and girls, aged 7–12 years, participating in the 2014/2015 football season (August to June). Boys and girls train and compete together in these age categories. Healthcare resource use was collected prospectively in the Swiss study arm of a cluster randomised controlled trial. This trial was conducted to test the efficacy of the ‘11+ Kids’ injury prevention programme compared with a regular warmup programme in children’s football. The study involved four countries (Switzerland, The Netherlands, Germany and the Czech Republic). The primary outcome was the potential reduction of all football related injuries. The study (ClinicalTrials.gov identifier: NCT02222025) complied with the Declaration of Helsinki and was approved by the local ethics committee (Ethikkommission Nordwest- und Zentralschweiz, EKNZ, approval No 2014–232). All children and their parents received written information about the project prior to the start of the study. Participation was voluntary and all parents of injured children gave their active consent. Study specific details of the randomised controlled trial are described in the original paper.22
Intervention
The intervention group (INT) used the ‘11+ Kids’ programme, replacing their usual warmup at the beginning of each training session throughout the season. The ‘11+ Kids’ is a 15 min warmup programme designed to prevent injuries in children’s football, consisting of seven different exercises each with five levels of difficulty.22 The exercises focus on dynamic stability, power, core strength and falling techniques. ‘11+ Kids’ has been proven to be efficacious in preventing injuries.22 Participants in the control group (CON) performed their usual warmup routine.
Outcome measures
Injury
During the football season, football related injuries that resulted in at least one of the following were recorded and followed-up by the research coordinators for up to 3 months following the end of the season19: (a) inability to complete the current match or training session and/or (b) absence from subsequent training sessions or matches and/or (c) injury requiring medical attention. Injury type, location and mechanism as well as time loss (ie, absence from sport participation) were documented via an internet based injury registration platform. Coaches entered injuries on a weekly basis. Directly after an injury was entered in the online system, study coordinators contacted coaches, parents and injured children to get more details on the injuries using a standardised questionnaire. Injuries were followed-up on a weekly basis at least until the child was back in training. In the case of an injury, parents forwarded the medical diagnosis and cost relevant information to the study coordinators.
Healthcare resource use and costs
Costs considered included direct healthcare costs and intervention costs. Intervention costs included actual expenses for the printed manuals and the organisation of instruction courses for the coaches, and potential opportunity costs of coaches due to their attendance at the ‘11+ Kids’ instruction course (table 1, for further information see online supplementary material 1).24 We used the sum of these costs and the number of players to calculate the total intervention costs per player (ie, player season).
Supplemental material
Intervention costs in the study and estimated costs for a countrywide implementation of ‘11+ Kids’
The healthcare resource use of injured players (ie, information on the number of visits to healthcare professionals, medical examinations, treatments and equipment used by injured players) was derived by contacting the parents of injured children via telephone. We applied the cost analysis from a healthcare perspective (direct costs). Standardised medical fees according to the national medical association (‘Tarmed’, V.1.08) enabled a precise estimation of the medical treatment costs of injuries.25 This approach has been applied previously and allowed for valuing the healthcare resources used (eg, visits to physicians, X-rays, casts).24 Out of pocket healthcare costs borne by the parents of injured players (eg, physical therapy, braces and visit to a chiropractor) were estimated based on the prices of various providers of such services and products. All costs are reported in Swiss Francs (CHF, 2015).
Projected costs and health effects for a nationwide implementation scenario of ‘11+ Kids’ in Switzerland (model based scenario)
In a further analysis, we estimated the costs of a nationwide implementation of ‘11+ Kids’ in Switzerland (table 1). These costs include expenses for printing and shipping the ‘11+ Kids’ manual, organisation of instruction courses to reach football coaches (including time expenditure for travel), loss of productivity during attendance of the course as well as the development and hosting of a website to provide the digital version of the manual over a time horizon of 5 seasons (see online supplementary material 1). We estimated a 50% turnover of coaches (ie, new coaches replacing coaches who retire/resign) over the course of 5 seasons. Therefore, we multiplied the costs for the manuals and the courses by an inflation factor of 1.5. The resulting overall costs for the printed manuals, education courses and the website were CHF568 533 over a 5 season period. Based on the actual number of players in children’s football in Switzerland (58 622 in the 2014/2015 season), this relates to CHF9.70 per player over a 5 season period and CHF1.94 per player season.
Statistical analysis
We calculated the mean cost per player (ie, player season) as the total cost in each group divided by the total number of players in each group, as well as the mean cost per injured player as the total cost in each group divided by the total number of injured players in each group. Further, we calculated the cost of injuries per 1000 hours of football exposure in each group. To obtain the corresponding 95% CI, we used non-parametric bootstrapping with 1000 samples to account for the skewed cost distributions.24
We calculated injury incidence density for both groups with corresponding 95% CI. Further, we analysed the time to event data using a mixed effects Cox model. The model accounted for clustering effects on team level and allowed analysis of multiple injuries to individual players while accounting for potential correlations on the intra-person level. We used age and age adjusted body height as covariates, as described previously.20 22
Cost effectiveness analysis
We calculated the differences in mean cost per player (ie, player season), mean cost per injured player and cost per 1000 hours of football exposure between the INT and CON groups. Differences in costs between the groups are presented as absolute cost differences (95% CI).
We estimated the incremental cost effectiveness ratio (ICER) to summarise the cost effectiveness of ‘11+ Kids’ and created cost effectiveness planes (figures 1 and 2).24 26 The ICER is the difference in cost per player between the INT and CON groups, divided by the difference in the number of injuries per player between the INT and CON groups. We calculated the ICERs for the ‘trial based’ data (figure 1) and for the ‘model based’ (countrywide implementation) scenario (figure 2).

Cost effectiveness plane presenting cost effect pairs in the ‘11+ Kids’ study (trial based data). Cost effect pairs were estimated using bootstrapping (1000 samples) for the difference in the costs and injury risk in the ‘11+ Kids’ intervention group versus the control group. Values in the southeast (dominant) quadrant indicate that the intervention group showed lower costs and lower injury incidence density. Data in the northwest quadrant (dominated) indicate that the intervention group showed higher costs and a higher injury incidence density.

{kind=link}
{kind=link}
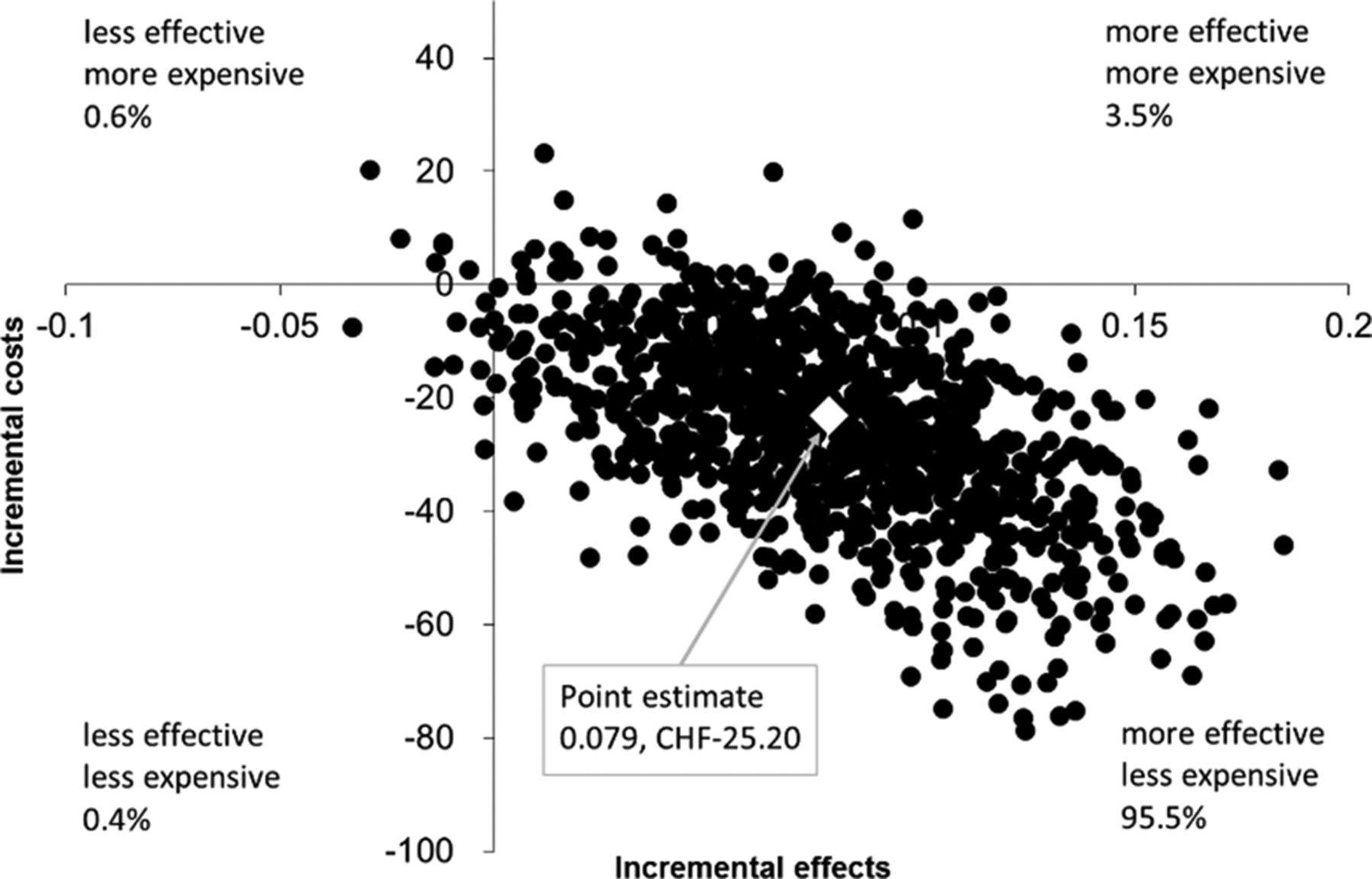
Cost effectiveness plane presenting model based data for a countrywide implementation of the ‘11+ Kids’. Cost effect pairs were estimated using bootstrapping (1000 samples) for the difference in the costs and injury risk in the ‘11+ Kids’ intervention group versus the control group. The figure shows simulated data for a countrywide implementation scenario in Switzerland over one football season. Values in the southeast (dominant) quadrant indicate that the intervention group showed lower costs and lower injury incidence density. Data in the northwest quadrant (dominated) indicate that the intervention group showed higher costs and a higher injury incidence density.
The cost effectiveness planes show four quadrants. Values in the southeast (dominant) quadrant indicate that the INT group showed lower costs and a lower injury incidence density. In contrast, the northwest quadrant (dominated) indicates that the intervention leads to higher costs and a higher injury incidence density. The southwest quadrant indicates that the intervention is less effective but less expensive and the northeast quadrant indicates that the intervention is more effective but more expensive.
If the intervention was ‘dominant’, an ICER was not calculated. We applied the cost evaluation with a time horizon of one football season and from a societal perspective, considering all relevant costs and effects, regardless of who pays or who benefits from the effects.
Results
Initially, 846 clubs in Switzerland were invited to participate. A total of 55 clubs (with 78 teams) agreed to take part in the study and were randomised according to the age groups of the teams and the size of the club. In total, 62 teams with 1002 players completed the study (for study flow of participants, see online supplementary material 2). Anthropometric characteristics were similar in the INT and CON groups. During the study period, 99 injuries (INT=42 injuries, CON=57 injuries) occurred, of which 53 were medically treated (table 2). For more details on injury characteristics (number, percentage and injury incidence density by injury location, type and mechanism for the INT and CON groups) and intervention effects on injury risk, see online supplementary material 2. Two of these 53 injuries were sustained by girls (both in the INT group). Table 3 shows the healthcare resource use of injured players and respective medical costs in both groups.
Player characteristics, exposure, injury, cost data and cost differences between the ‘11+ Kids’ intervention and control groups
Healthcare resource use of injured players and respective medical costs in the ‘11+ Kids’ intervention and control groups
Trial based cost effectiveness analysis
We took the actual costs of the ‘11+ Kids’ intervention in the study setting into account. These costs include expenditures for the manuals, organisation of education courses for the coaches as well as costs of coaches attending the ‘11+ Kids’ instruction course. Total intervention costs were CHF4.02 per player (ie, player season) in our study (table 1, and see additional information in online supplementary material 1).
Figure 1 depicts the cost effectiveness plane of the INT group in comparison with the CON group. The ICER for the INT group in comparison with the CON group was dominant (95% CI dominant, dominant), based on a difference in the mean cost per player (ie, player season) of CHF−23.12 and a difference in the mean efficacy of 7.9% (ie, 14.7% of players injured in the CON group versus 6.8% in the INT group). Of all bootstrapped ICERs, 94.6% were located in the southeast (dominant) quadrant (figure 1), indicating that there were considerably lower costs and fewer injuries compared with the CON group.
Incremental cost effectiveness ratio for a countrywide implementation scenario in Switzerland
For a countrywide implementation scenario (model based), the ICER was dominant (95% CI dominant, dominant), based on a difference in the mean cost per player of CHF−25.20 and assuming the same difference in efficacy of 7.9%. For this scenario, 95.5% of the bootstrapped ICERs of the INT group were located in the southeast quadrant, demonstrating dominance of the INT group above the CON group (figure 2).
Estimated injuries and costs avoided with implementing ‘11+ Kids’ in Switzerland
Table 1 displays the data on which we based our estimation of costs for implementing the programme in Switzerland (further information in online supplementary material 1). Based on the difference in the mean cost per player (CHF−25.20) between the INT group and the CON group and the number of players in Switzerland, CHF1.48 million in healthcare costs could be avoided with the ‘11+ Kids’ injury prevention strategy in just one season.
Discussion
Main study findings
The new injury prevention programme ‘11+ Kids’ has been shown to reduce football injuries in children in a multicentre cluster randomised controlled trial compared with a standard warmup.22 Based on data from Switzerland, we analysed direct medical costs of injuries. This exercise based injury prevention programme is efficacious in reducing the number of football injuries by 50%. In addition to the number of injuries, healthcare costs per player season were 59% lower (CHF−23.12, 95% CI −39.09 to –7.14) and costs per 1000 hours of football exposure were 51% lower (CHF−240.66, 95% CI −406.89 to –74.32) compared with the team’s usual warmup. Further, the cost effectiveness analysis showed a 94.6% likelihood (trial based data) and a 95.5% likelihood (model based implementation scenario) for the intervention programme being dominant (ie, more effective and less costly) over the usual warmup routine.
Comparison with previous studies
A previous study investigating the cost effectiveness of a neuromuscular training programme in youth football (13–18 years) found both a reduction in injuries (−38%) and costs (−43%). These findings highlight the importance of widely implementing exercise based injury prevention strategies in youth football.27 No study has previously investigated the economic impact of exercise based injury prevention in children’s football. Our findings (in players <13 years of age) show similar beneficial injury and cost reduction effects as the above mentioned study in older players. A randomised controlled trial in adult male amateur football players, however, did not show an overall reduction in injury, but did show a reduction in direct healthcare costs related to injury (−27%). The authors concluded that the cost savings might be related to the preventive effect of knee injuries in the INT group.28
In The Netherlands, annual cost savings of €35.9 million (CHF38.4 million, EUR-CHF 1.07, 2015; USD39.8 million, EUR-USD 1.11, 2015; GBP26.0 million, GBP-EUR 1.38, 2015) have been estimated, given a widespread application of a programme to reduce the recurrence of lateral ankle sprains, compared with usual care.29 A further study from this group concluded that bracing is the dominant secondary preventive intervention over both neuromuscular training and the combination of neuromuscular training and bracing.24 In contrast with other intervention programmes, the proposed ‘11+ Kids’ does not require special training equipment, like balance boards, which is a major advantage regarding cost effectiveness.27
Strengths and limitations
The proportion of girls was representative of the population of football playing children in Switzerland. However, the absolute number was too low to draw conclusions about girls specifically. In older players, similar preventive effects of the ‘11+’ have been described for young female and male football players.30 31 Hence comparable effects could be expected for girls and boys in children’s football.
Costs related to side line treatment of injuries (eg, first aid, tape) were not recorded. However, it could be assumed that the total costs of these treatments were low and did not substantially influence the results. If there was an influence, it could be speculated that it would be in favour of the INT group, as the risk for mild and moderate injuries was also reduced.22
We did not investigate indirect costs related to injury (eg, loss in productivity of parents when nursing the injured child). In a study on Dutch schoolchildren aged 10–12 years, indirect costs accounted for 40% of the total injury related costs.11 Therefore, it can be assumed that the reduction in injury costs observed in our study substantially underestimates the total financial savings.
In common with previous high quality studies, injury data were reported by coaches. Only if an injury was reported by the coach, parents and players were contacted to gather detailed information.30–32 To maximise the quality of reporting, all coaches of the INT and CON groups were thoroughly instructed on the injury definitions and were regularly contacted by our study assistants to ensure timely and complete data entry. To minimise potential recall bias, coaches received an automated reminder via email within a week if they did not enter data into the online system. After 2 weeks without data entry, our study assistants contacted the coaches personally (via telephone and/or email).
Data recording in the INT teams started after the ‘11+ Kids’ instruction session. Therefore, the exposure time was lower in the INT group than in the CON group. We performed a sensitivity analysis by cutting the respective time period (exposure time and injury events) in the CON group at the beginning of the season. The results were similar compared with the regular analysis. Consequently, the observed intervention effect was very likely not biased.
The statistical approach does not allow controlling for potential confounders. However, in the corresponding publication on the efficacy of ‘11+ Kids’, we controlled the analysis for team and intra-person clustering, age, age independent body height and match training ratio.22 It was, however, not possible to control the analyses for previous injury as the level of detail of these retrospectively collected data was too heterogeneous. The observed point estimate of the intervention effect got stronger (ie, in favour of the INT group) by controlling for the above mentioned confounders. Therefore, the reported cost reductions could be considered conservative.
Societal costs may be additionally reduced through less dropouts from sport, leading to higher physical activity levels in the long term. Children remain active and are more likely to become active adults with a lower risk of lifestyle related diseases.1 3 33 34 However, our data provide only a snapshot of the potential short and long term effects of implementing such a sports injury prevention programme.
Future perspective
A major argument for coaches to use exercise based injury prevention is the positive effect on athletes’ performance.21 35 36 It is important to convince coaches and players to regularly use the programme, as compliance with the programme is directly linked to the reduction in injury risk.22 35 37 38 It has been shown that injuries had a significant negative influence on team performance in male professional football.39 This underlines the importance of injury prevention to increase a team’s chances to win matches.
Injuries are among the most important reasons for dropping out from sport.40 Dropout from sport is directly associated with lower physical activity levels. The resulting reduction in physical activity negatively affects health and well being.2 41 Injury prevention not only supports the individual to stay injury free but it is also positively associated with physical activity in the long term.3 As such, it can be stated that the relevance of injury prevention at an early age is widely underestimated.
An efficacious preventive programme needs to be adopted and used in the real world setting to achieve health benefits in the population.42 When developing ‘11+ Kids’, we worked closely with researchers, clinicians, practitioners and members of the target community.43 Therefore, the programme has a good chance of fulfilling the requirements of being adopted by the wider community. Including the ‘11+ Kids’ in coaches’ education could enable a countrywide reach. Countrywide campaigns have started in New Zealand (see http://fit4football.co.nz/the-11plus/11plus-kids) and the Czech Republic. It is planned that other countries will follow soon.
Conclusion
The warmup and injury prevention programme for children’s football ‘11+ Kids’ substantially reduced injury related costs and was cost effective compared with a usual warmup routine, in terms of realistic implementation costs. These findings provide strong evidence for the implementation of this programme.
What are the new findings?
The ‘11+ Kids’ programme reduced the injury related healthcare costs by 51% in players aged 7–12 years.
The cost effectiveness analysis showed a 94.6% likelihood (trial based data) and a 95.5% likelihood (model based implementation scenario) for ‘11+ Kids’ being dominant (ie, more effective and less costly) over usual warmup.
How might it impact on clinical practice in the near future?
The clear reduction in injury related costs provides strong evidence for a widespread implementation of the ‘11+ Kids’.
A countrywide application of ‘11+ Kids’ in Switzerland could prevent approximately 2500 medically treated injuries and save CHF1.48 million in direct healthcare costs per year.
Countrywide implementation campaigns have started already in New Zealand and the Czech Republic
Acknowledgments
We thank the study assistants Nadine Rolser, Silvan Stürchler, Florian Giesin, Fridolin Petersen, Florian Lohberger and Marco Bassanello for their support during data collection. We thank all participating football clubs, coaches, players and parents.
References
Footnotes
Contributors RR, EV and OF designed the study protocol. AJ and JD contributed to the design of the study. RR organised the study (ie, recruitment, data collection, quality control). EL contributed to study organisation. RR conducted the overall data management and organised the data preparation. EL contributed to the data preparation. RR analysed the data. RR and NR wrote the manuscript. RR, OF, EV and NR revised the manuscript. All authors contributed to reviewing and revising the manuscript, and agreed on the final draft.
Funding This study was supported by Fédération Internationale de Football Association and the University of Basel (grant: Top-Up Stipend).
Competing interests AJ was a member of the FIFA Medical Assessment and Research Centre (F-MARC). JD was chairman of F-MARC and consulting member of the FIFA Medical Committee until Autumn 2016.
Patient consent Not required.
Ethics approval The study was approved by Ethikkommission Nordwest- und Zentralschweiz, EKNZ (approval No 2014-232).
Provenance and peer review Not commissioned; externally peer reviewed.