Article Text

Statistics from Altmetric.com
Starting and sticking to an exercise programme is challenging for most who are at risk of developing lifestyle-related chronic disease: the most physically inactive, unfit, and overweight or obese middle-aged individuals, that is, the majority of the adult population. The 2018 US Physical Activity Guidelines for Americans1 introduced a number of new elements that will undoubtedly change how we think about and promote physical activity (PA). Not to anyone’s surprise, the new guidelines abandoned the unsupported by empirical evidence idea that PA needs to be accumulated in at least 10 min continuous bouts to be health enhancing.1 This opens new exciting opportunities to capitalise on sporadic, incidental in nature, PA to improve the population’s health.
Incidental PA: what is it and why is it appealing?
Incidental PA is any activity that is part of one’s daily living that is not done with the purpose of recreation or health and requires no sacrifice of discretionary time. For example, walking or cycling to move from place to place, stair climbing and active daily chores, such as carrying heavy shopping1 and house cleaning. Inherently, incidental PA does not encounter the myriad of barriers to structured exercises, such as lack of time, costs, equipment, lack of skills or poor fitness. In itself, such a feasibility advantage may signal a turning point as fewer barriers mean that many more people can be incidentally active than recreationally active. What is far less clear is how to maximise the health impact of incidental PA and how to convince and empower people to be physically active in their daily lives. In this editorial, we address the first of these questions.
The length of each incidental PA bout can vary from a ‘short and sweet’ few seconds, such as climbing a few flights of stairs 3–4 times a day,2 to several minutes or even hours of active commuting, housework or shopping. Besides meeting recommended targets, incidental PA offers opportunities for brief episodes of vigorous intensity PA (VPA) which, compared with moderate intensity, provides superior ‘per time unit’ health benefits.1 3 For most practitioners, researchers and the public, VPA is synonymous with participation in continuous exercise lasting at least 20–30 mins3, such as running or playing racquet sports. Conversely, few would associate incidental PA with vigorous intensity.4 Both of these misconceptions have flourished for two key reasons: (a) the inability of questionnaire-based studies to capture most sporadic and incidental PA; and (b) the overemphasis on absolute MET intensity, that is, multiples of resting metabolic rate expended during activity. Absolute intensity ignores the large variations between individuals in cardiorespiratory fitness (CRF) and RMR. For example, RMR decreases considerably with age, higher adiposity and female gender5; and correspondingly, the MET intensity of any given activity is higher in older and overweight/obese individuals and women. The online supplementary table 1 lists the absolute and corrected (for age, sex and height/weight6) MET values for common forms of incidental PA. Over 30% of walking scenarios cross the VPA threshold of 6 absolute METs7 and an additional 10% of all activities listed cross the 6 MET threshold after resting metabolic rate corrections. Although crude, such examples illustrate that once variations in resting metabolic rate are taken into account, a broad array of daily tasks will be classified as VPA for many adults. It is thus encouraging that the 2018 US guidelines emphasise the importance of relative intensity and acknowledge that incidental PA can be of vigorous intensity.1
Supplementary file 1
The ‘best bang for buck for time unit’ exercise
The time-economy advantage of VPA1 further strengthens the case for making the most of the ‘best bang for the buck for time unit’ incidental PA. High-intensity interval training (HIIT) is a time-efficient approach to exercise characterised by brief bursts of VPA near (typically >80%) or above VO2max, interspersed with periods of low activity or rest.8 HIIT has the capacity to induce rapid peripheral adaptations (eg, activation of peroxisome-proliferator-activated receptor γ coactivator-1α and muscle mitochondrial biogenesis), as well as improve the structure and function of the cardiovascular system. These effects are linked with improvements in glycaemic control and other metabolic syndrome components and, most notably, CRF.8 High PA intensity is undoubtedly a key to these beneficial physiological changes, as the effects of very low-volume HIIT appear similar to those achieved with traditional continuous exercise.
Large population cohort studies9 are also in agreement that any amount of VPA confers mortality gains with little or no volume dose–response. Studies that compared the volume and intensity of incidental PA are also consistent. For example, data from Copenhagen, a city where >50% of all trips involve walking or cycling, showed that higher relative intensity of cycling, but not higher daily cycling volumes, was associated with substantial life expectancy gains and lower cardiovascular disease mortality risk.10
In other words, both experimental and epidemiological evidence point towards the superiority of occasionally reaching vigorous exertion over total exercise volume.
Translating ‘best bang for buck for time unit’ exercise evidence into a simple message
Despite the potential of HIIT, translation from short-term supervised interventions into population-level PA promotion is challenging, as both starting and sticking to HIIT programmes are difficult or even unattainable for the most physically inactive and least fit individuals. With time economy as the primary concern, potent solutions to physical inactivity will be realised by interpreting key HIIT principles into incidental PA patterns. For example, consider a pattern of 3–5 short (0.5–2 min) sporadic bouts of high relative intensity PA spread across a whole day. Such a sporadic incidental PA pattern scores high on the biological plausibility scale as the totality of the HIIT literature manifests remarkably consistent health and fitness benefits irrespective of the number of repetitions, duration (eg, from 6 s to 4 min) and intensity of the various protocols.8 The regularity of the high-intensity PA stimulus that underpins the health potency of HIIT may be driving the improvements in fitness that occur through regular but short (≈20 s) stair climbing sessions among young adults.2
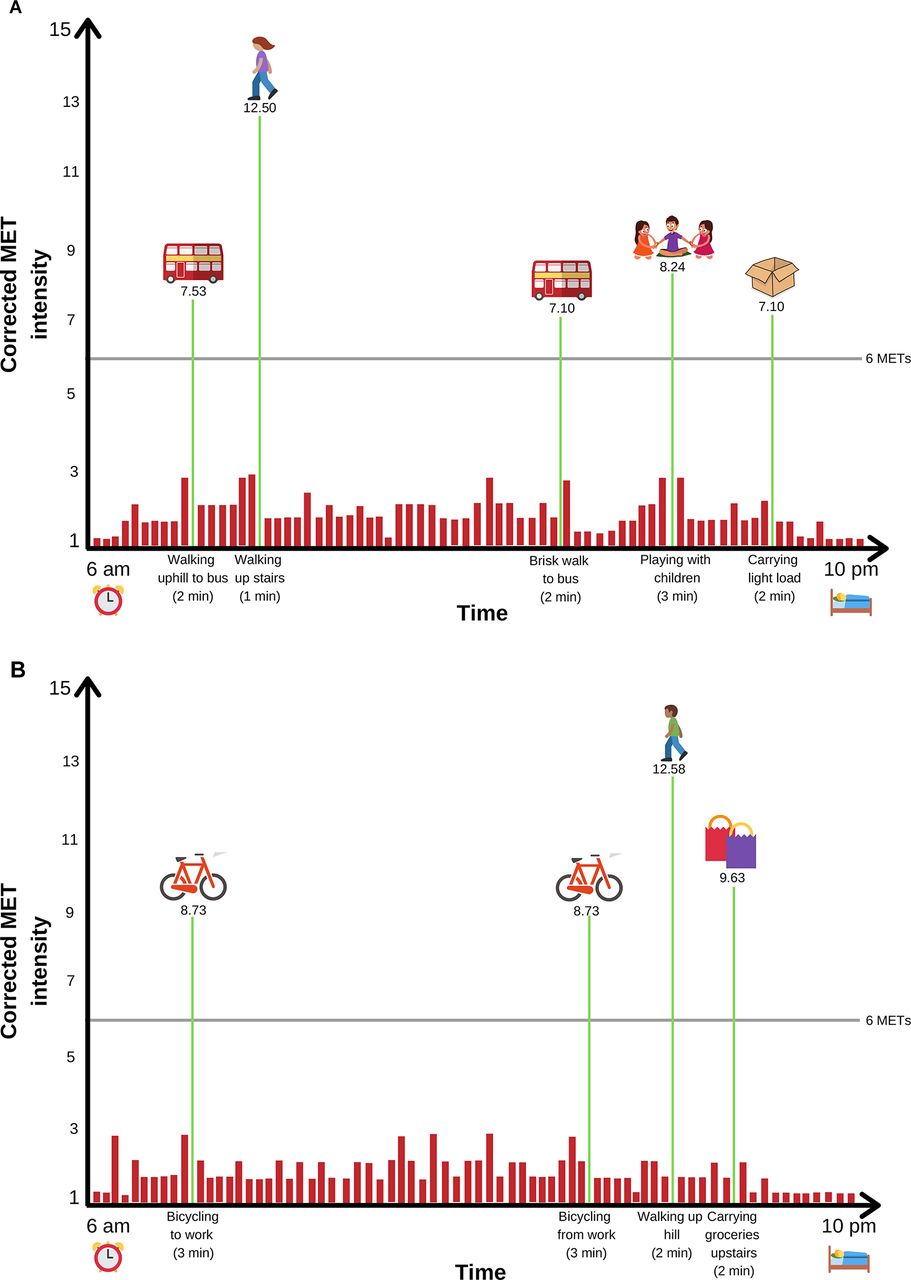
Such sporadic incidental PA patterns are achievable for most adults. Drawing data from the corrected MET values of the online supplementary table 1, figure 1 illustrates two hypothetical examples of high relative intensity incidental PA patterns totalling 10 min per day for two physically inactive middle-aged individuals. Assuming that this virtually zero time commitment PA pattern is relatively consistent (eg, 5–6 days per week), the contribution of such sporadic HII PA towards meeting the PA guidelines1 would be significant (≥2/3 of the total requirement), making it a particularly attractive option for inactive, obese and other individuals in greatest need of lifestyle intervention.
{kind=link}
Hypothetical examples of a sporadic incidental vigorous PA pattern for two otherwise physically inactive individuals. (A) Corrected* MET intensities are based on a 60-year-old woman, 72 kg and 162 cm tall (BMI 27). Activities shown include walking, 2.9–3.5 mph, uphill, 1%–5% grade (Compendium code 17210); stair climbing, fast pace (17134); walking, 4.0 mph, level, firm surface, very brisk pace (17220); walking/running, playing with child(ren), vigorous effort, only active periods (05180); moving, lifting light loads (05121). (B) Corrected* MET intensities are based on a 55-year-old man, 85.9 kg and 175.6 cm tall (BMI 27). Shown activities include bicycling to/from work, self-selected pace (01011); walking, 5.0 mph, 3% grade (17235); carrying groceries upstairs (05056). *MET intensities corrected based on Harris-Benedict RMR.6 Corrected MET=Compendium of PA7 assigned MET value x (3.5/Harris-Benedict predicted RMR).6 MET, metabolic equivalent; PA, physical activity; RMR, resting metabolic rate.
Conclusion
The 2018 US PA guidelines opened new horizons for PA and exercise medicine practice by recognising that any bouts of PA count for health.1 Building a daily routine that incorporates brief sporadic bouts of high relative intensity incidental PA has numerous practical and health advantages. The next step is to empirically examine the health effects of such PA on key outcomes in large longitudinal cohorts using wearable monitors and to develop environmental and clinical programmes promoting high-quality incidental PA during daily living. On top of ‘move as often as possible and sit less’,1 public health and clinical practice could emphasise simple messages analogous to ‘huff and puff regularly’.
Footnotes
Contributors ES: drafted the manuscript. All authors contributed to re-drafting and revisions of the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.