Article Text

Abstract
A systematic review of the literature on the frequency and characteristics of sports related growth plate injuries affecting children and youth in organised sport was carried out. Both acute and chronic physeal injuries related to participation in sports have been reported to occur, although injury incidence data are somewhat limited. Of particular concern is the growing number of stress related physeal injuries, including those affecting the lower extremities. Although most physeal injuries appeared to resolve with treatment and rest, there is also evidence of growth disturbance and deformity. Possible injury risk factors and countermeasures are discussed, and suggestions for directing future research provided.
- growth plate
- epiphyseal
- physis
- injuries
- children
Statistics from Altmetric.com
Participation in children’s and youth sports is widespread in Western culture. Many of these youngsters initiate year round training and specialisation in their sports at a very early age. Preteens training at regional training centres or with high school and club teams in sports such as gymnastics may train 20 or more hours a week. In addition, many youngsters travel with select soccer or hockey teams to other towns and communities to compete on a regular basis. Increased involvement and difficulty of skills practiced at an early age and continued through the years of growth, with the level of intensity required to be competitive, raises concern about risk and severity of injury to young athletes.
In particular, the concern is that the tolerance limits of the physis may be exceeded by the mechanical stresses of sports such as football and hockey or by the repetitive physical loading required in sports such as baseball, gymnastics, and distance running.1,2 Disturbance of physeal growth as a result of injury can result in length discrepancy, angular deformity, or altered joint mechanics and may cause significant long term disability. This article describes the present status of knowledge on the frequency and characteristics of physeal injuries affecting children and youth involved in organised sport. In doing so, possible risk factors are elucidated that may assist in developing specific recommendations for injury prevention and for directing future research.
METHODS
A literature review was undertaken using Medline and SPORTDiscus. The search was restricted to English language articles. Medical subject headings and text words included: growth plate, physis, epiphyseal, physeal, athletic injuries, sports, injury, and injuries. Each title was searched manually for any focus on growth plate injuries involving the long or tubular bones of young athletes. Titles focusing on sport related apophyseal injuries were excluded given the focus of the present review on injuries that may adversely affect growth. The reference lists of selected articles were searched using the same criteria.
Most reports retrieved were case reports or case series investigations where the characteristics of a series of people who were injured are detailed. These investigations allow a comprehensive account of the characteristics and relative frequency of sport related physeal injuries. However, they do not allow calculation of incidence rates or the identification of risk factors unless denominator data are available. The literature on the epidemiology of paediatric sports injuries was next searched in order to obtain, as far as possible, an insight into the prevalence and incidence of growth plate injuries in children’s and youth sports.
ANATOMY AND PHYSIOLOGY OF THE PHYSIS
The growing parts of the bone include the physis and the epiphysis. Two types of epiphyses are found in the extremities: traction and pressure. Traction epiphyses (or apophyses) are located at the site of attachment of major muscle tendons to bone and are subjected primarily to tensile forces. The apophysis of the tibial tubercle provides an example (fig 1). The apophyses contribute to bone shape but not to longitudinal growth.3 As a result, acute or chronic injuries affecting traction growth plates are not generally associated with disruption of longitudinal bone growth. Overuse apophyseal conditions, such as Osgood-Schlatter disease, Sever’s disease, and medial epicondylopathy in the throwing arm, are common in young athletes and may be the source of significant discomfort and time lost from training.

An illustration of the location of the physes and epiphyses of the distal femur and proximal tibia, and the tibial tubercle apophysis. Illustration by Kevin Short. From Caine.1 Reprinted with permission from S Karger AG, Basel.
Pressure epiphyses are situated at the end of long bones and are subjected to compressive forces. The epiphyses of the distal femur and proximal tibia are examples of pressure epiphyses (fig 1). The growth plate or physis is located between the epiphysis and metaphysis and is the essential mechanism of endochondral ossification.4 In contrast with traction growth plates, injury to pressure epiphyses and their associated growth plates may result in growth disturbance. Physeal injuries of the latter type sustained in organised sport are the focus of this article.
Briefly, as explained by Ogden,4 in the zone of “growth”, germinal cells are attached to the epiphysis and obtain their vascular supply from the epiphyseal artery. Longitudinal growth is accomplished by the proliferation of these cells. The zone of growth is the area of greatest concern with any fracture involving the growth plate, as damage to cells in this zone may have long term consequences for normal growth patterns.
The next functional area is the zone of cartilage “maturation”. Increased extracellular matrix is formed in this zone, primarily between columns. The extracellular matrix exhibits cell mediated biomechanical changes, then calcifies. The cells align in vertical columns as they hypertrophy and are eventually replaced by osteoblasts. Fractures most commonly occur at the junction of calcified and uncalcified hypertrophic cells because it is structurally the weakest portion of the growth plate.4
In the zone of cartilage “transformation”, the cartilaginous matrix is penetrated by metaphyseal vessels, which break down the transverse cartilaginous septa, allowing invasion of mature cell columns. The cartilage and the bone are remodelled, removed, and replaced by a more mature, secondary spongiosa, eventually containing no remnants of the cartilaginous precursor.4
SUSCEPTIBILITY TO INJURY
Physeal injuries may produce irreversible damage to the growing cells, resulting in growth disturbance. Growth plate cartilage is less resistant to stress than adult articular cartilage.5,6 It is also less resistant than adjacent bone to shear and tension forces. Therefore, when disruptive forces are applied to an extremity, failure may occur through the physis. In addition, the physis may be 2–5 times weaker than the surrounding fibrous tissue.7 For these reasons, injury mechanisms that in an adult may result in a complete tear of a ligament or in a joint dislocation may produce a separation of the growth plate in a child.
The susceptibility of the growth plate to injury appears to be especially pronounced during periods of rapid growth.4,5,8,9,10,11,12,13,14,15,16,17 Research on the development of physeal cartilage in animals shows a decrease in physeal strength during pubescence.8 The data on humans are consistent with these findings.9–11 An increase in the rate of growth is accompanied by structural changes that result in a thicker and more fragile plate.9,12 In addition, bone mineralisation may lag behind bone linear growth during the pubescent growth spurt, rendering the bone temporarily more porous and more subject to injury.13 Studies of the incidence of physeal injuries in humans indicate an increased occurrence of fractures during pubescence,12–16 with the peak fracture rate probably occurring at the time of peak height velocity.13
It has been proposed that the growth spurt may also increase susceptibility to growth plate injury by causing an increase in muscle-tendon tightness about the joints and an accompanying loss of flexibility.18 However, this concept is controversial.19 Longitudinal growth occurs initially in the long bones of the extremities, and the muscle-tendon units elongate in response to this change. This may create a temporary disparity between muscle-tendon and bone lengths. If an excessive muscular stress is applied, a muscle-tendon imbalance is produced that may predispose to injury.20 Because the joint, and in particular the growth cartilage, is the weak link in this assembly, it is believed that the risk of injury may be increased at this site during the growth spurt.18 However, Feldman et al19 have questioned whether a reduction in flexibility occurs during the adolescent growth spurt.
ACUTE PHYSEAL INJURY
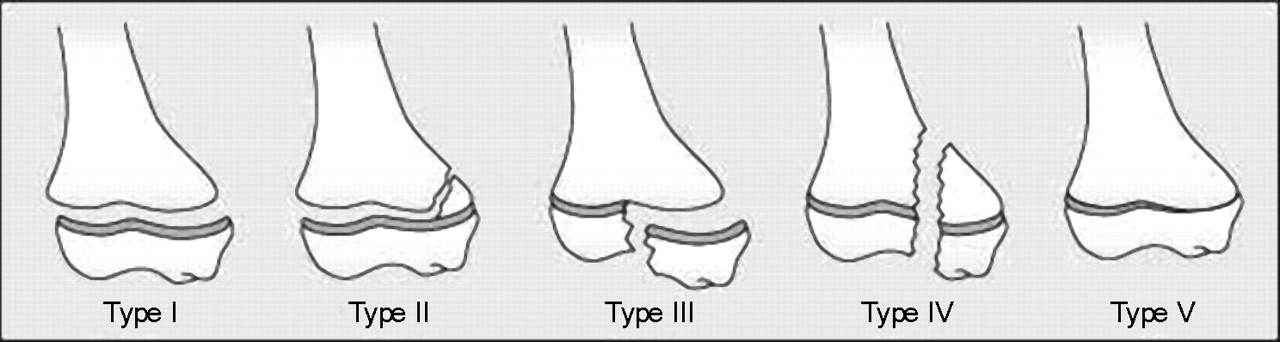
Although more elaborate classification systems for describing acute physeal injuries are available,4 the system most widely used was developed by Salter and Harris.21 Figure 2 shows the different types of injury in this classification. Type I injuries show a complete separation of the epiphysis from the metaphysis without any bone fracture. The germinal cells of the growth plate remain with the epiphysis, and the calcified layer remains with the metaphysis. In type II, the most common physeal injuries, the line of separation extends along the growth plate, then out through a portion of the metaphysis, producing a triangular shaped metaphyseal fragment sometimes referred to as the Thurston Holland sign. Type III, which is intra-articular, extends from the joint surface to the weak zone of the growth plate and then extends along the plate to its periphery. In type IV, often involving the distal humerus, a fracture extends from the joint surface through the epiphysis, across the full thickness of the growth plate and through a portion of the metaphysis, thereby producing a complete split. In type V, a relatively uncommon injury, there is a compression of the growth plate, thereby extinguishing further growth.

Prognosis for types I and II fractures is good if the germinal cells remain with the epiphysis, and circulation is unchanged. However, these injury types are not as innocuous as originally believed, and can be associated with risk of growth impairment.4,16,22–28 Figure 3 provides a radiographic depiction of a Salter-Harris type II injury in a young male gymnast. Type III injuries have a good prognosis if the blood supply in the separated portion of the epiphysis is still intact and if the fracture is not displaced. Surgery is sometimes necessary to restore the joint surface to normal. In type IV injuries, surgery is needed to restore the joint surface to normal and to perfectly align the growth plate. Type IV injuries have a poor prognosis unless the growth plate is completely and accurately realigned.

A radiographic illustration of a Salter-Harris type II supracondylar fracture of the humerus in a 9 year old male gymnast who fell badly after a vault.
Studies of more than 200 specimens of simultaneously occurring physeal fractures in children (usually from traumatic amputation) and skeletally immature zoo animals indicate that the typical physeal fracture occurs within the hypertrophic zone.4 The most common level was the junction of calcified and uncalcified hypertrophic cells. However, variation in fracture propagation may occur that relates to extent of physical maturity, the amount of force applied, rates of loading, and particularly the application of forces.4,8,29,30 In addition to the variable undulation of the fracture plane in physeal injuries, an important finding is microdisruption in the germinal zone that is separate from the main cleavage plane.4
Approximately 15% of all fractures in children involve the physis.4,31 Acute growth plate injuries such as those incurred by falling off bicycles, skateboards, playground equipment, out of trees, and so forth, are common to many childhood misadventures. In one large population based study of growth plate injuries, the largest single group of physeal fractures occurred as a result of a fall, usually while running or playing around furniture or playground equipment.14 Competitive sports—for example, hockey, football, baseball—accounted for 33.5% and recreational activities—biking, skateboarding, skiing—for 21.7% of physeal injuries in this study. In several studies, organised sports accounted for more physeal injuries than recreational activities.11,14,16,25,32,33 American football is the sport most often connected with acute physeal fractures; however, most other sports are also represented.14,16,25,27 Motor vehicle accidents, including motorcycles and all-terrain vehicles, also account for a significant number of especially severe physeal injuries.
Reports on acute physeal conditions affecting young athletes are abundant and arise primarily from case reports and case series data involving mostly male athletes (table 1).34–66 These injuries were incurred in a variety of sports, although football is the sport most often reported. Injury outcome was generally good with growth disturbance reported in only eight of 50 cases; however, the length of follow up was brief or not reported in some cases. Most of the athletes were advanced in age (13–17 years), limiting the amount of growth disturbance possible.
Case reports including data on sports related physeal fractures
Table 2 summarises case series reporting growth plate fractures.11,14,16,22,24,25,27,32,33,67–74 With the exception of two studies that reported on only sport related physeal injuries, the studies reviewed reveal a wide range in the proportion of fractures associated with organised sports (5.6–72.8%), and a wide range that were associated with growth disturbance (0–75%).
Case series including data on sports related physeal fractures
Most cohort studies reporting on the nature and incidence of paediatric sports injuries describe the frequency of fractures without specifying the frequency or severity of physeal fractures.75,76 There is also rarely any follow up to indicate the outcome of physeal injuries. Table 3 provides a summary of cohort studies that do provide information on the frequency of physeal fractures in several sports.77–89 Perusal of these reports reveals that 1–30% of paediatric sports injuries are acute physeal injuries. Of concern in these reports is the finding that sprains were common injuries and that not all injuries were seen by a doctor. As discussed above, an injury that would cause a sprain in an adult can be a potentially serious growth plate injury in a child.
Cohort studies including data on sports related physeal injuries
CHRONIC PHYSEAL INJURY
An accumulating number of clinical reports indicate that sport training, if of sufficient duration and intensity, may precipitate pathological changes of the growth plate and, in extreme cases, produce growth disturbance. This injury appears to occur through repetitive loading, which alters metaphyseal perfusion and in so doing interferes with the mineralisation of the hypertrophied chondrocytes, which typically occurs in the zone of provisional calcification.4 The hypertrophic zone continues to widen because of constant growth in the germinal and proliferative zones,4 as shown experimentally by Jaramillo et al.90 MRI findings of distal radial physeal injury reported in Chinese acrobats and young competitive gymnasts91,92 resemble the experimentally induced injuries described by Jaramillo et al.90
Briefly, as explained by Ogden,4 the widening of the growth plate within the hypertrophic zone is usually temporary, as the resting and dividing cellular layers of the growth plate, and the attendant epiphyseal and metaphyseal blood supplies, are essentially undisturbed. However, in some situations, this ischaemic condition may lead to osseous necrosis and deformity within the developing ossification centre and to growth irregularities in the physis. These changes may be localised and cause asymmetric growth, or they may involve the entire physis and result in an overall slowdown of the rate of growth or even complete cessation of growth. In either case, premature closure of some or all of the physis may occur.4
Baseball pitchers were perhaps the first young athletes recognised to present with stress related injury of the physis.93 Table 4 shows studies reporting stress changes or stress fracture of the proximal humeral physis in young baseball pitchers.93,94,95,96,97,98,99,100,101,102,103,104 Often associated with persistent pain in the throwing arm, stress changes of the proximal humeral growth plate, or “Little league shoulder”, represent sequelae of repetitive traction and rotational forces across the epiphysis and growth plate.99 In most cases, subjects improved with rest and were able to return to baseball, albeit in some cases to a position other than as pitcher. In one instance there was premature closure of the proximal humeral physis.102
Pathological changes involving the proximal humeral physis in baseball players
Similar cases of stress related proximal humeral physeal widening (Salter-Harris type 1 fractures) have been reported in other young athletes involved in overhead sports including: cricket,105 gymnastics,106 badminton,107 and swimming and volleyball.108 Johnson and Houchin108 suggest that this condition may be more appropriately termed “adolescent athlete’s shoulder.” Chronic physeal injuries affecting the distal humerus and proximal radius of young baseball players are also documented.109,110 Stress related physeal fractures of the middle phalanx of the finger have also recently been reported in young sport climbers.111
Table 5 summarises case data on stress related lower extremity physeal injuries involving paediatric athlete participants representing a variety of sports and activities.112–121 In these cases, diagnosis of physeal stress fracture was based on widening of the physis and irregularity of the metaphyseal line or fragmentation or separation of the metaphysis. Symptoms arose primarily from running related activities, including long distance running. Most subjects improved with rest and were able to return to their sport. However, in one case119 there was a premature closure of the right proximal tibial growth plate, and in another,121 bilateral varus deformity of the knees. In the latter case, the subject was non-compliant and continued vigorous tennis training despite physician prescription for rest.
Pathological changes involving lower extremity physes in young athletes
Notably, in one case, a stress reaction of the proximal tibial growth plate developed in response to extreme repetitive rotational and pressures forces on the epiphysis associated with the practice of rugby place kicking.120 The mechanism of injury is believed to be similar to that seen from overuse in the proximal humeral epiphysis of throwing athletes.120 In a second, similar case,121 stress injury of the distal femoral physis developed in a football place kicker (fig 4). Clinical resolution of symptoms in this case occurred in 23 days.

Fifteen year old male football place kicker. (A) Frontal radiograph and (B) magnetic resonance image of right knee showing physeal widening of lateral aspect of distal femoral physis (arrow). (C) Frontal radiograph obtained three months after immobilisation showing near complete resolution of physeal widening. From Laor et al.121 Reprinted with permission from the American Journal of Roentgenology.
The most commonly reported physeal stress injuries have been those affecting the distal radial physes of young gymnasts.91,122–137 Most reports describe distal radius stress reaction with a radiographically widened and irregular physis, especially on the metaphyseal side. However, Read122 reported stress fractures of the epiphysis and metaphysis in the distal radii of young female gymnasts. Table 6 summarises case data on stress related physeal injuries involving the distal radius of gymnasts.
Case reports and case series of physeal injuries involving the distal radius of gymnasts
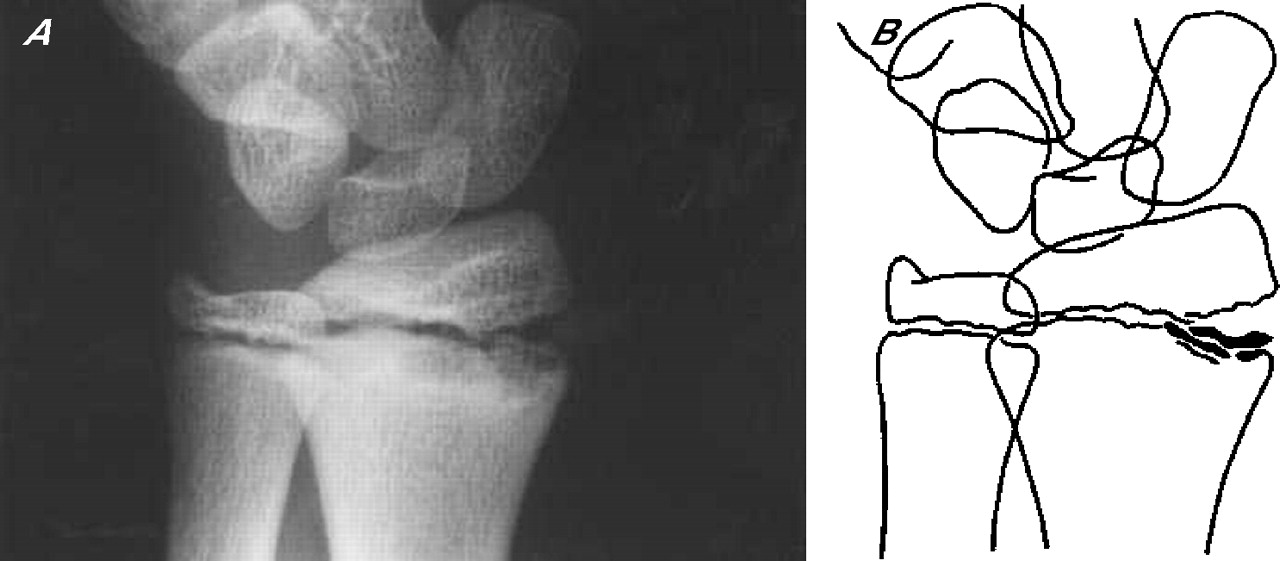
Figure 5 shows an illustration of the stress injured distal radial physis of a gymnast. In the studies reviewed (table 6), almost all patients with stress related injury affecting the distal radius recovered with rest, and did not experience premature physeal closure or abnormal growth. However, there are four subsequent reports of distal radius physeal arrest in skeletally immature female gymnasts.128,133–137 Evidence of premature growth arrest in these reports was provided by repeated roentgenographic evaluations, which revealed discrepancies in radiographic status of the growth plates in the involved and uninvolved bones and extremities. Figure 6 shows an illustration of partial closure of the right distal radial physis in a 14 year old female gymnast.134,137

Radiograph (A) and line drawing (B) of the wrist in a symptomatic young female gymnast with findings of widening of the distal radial physis, breaking of the epiphysis, and cystic changes and irregularity of the metaphyseal margin. From Roy et al.123 Reprinted with permission from The American Orthopedic Society for Sports Medicine.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fourteen year old female gymnast with chronic right wrist pain. The image on the right is of the symptomatic right wrist and shows partial closure of the right distal radial physis. The ulnar physis remains open. The image on the left is of the asymptomatic left wrist. Both physes of the left wrist remain open. From Caine et al.137 Reproduced with permission from Elsevier.
There are also analogous reports of stress related premature physeal closure in other young people. Carson and Gasser102 reported on an 11 year old pitcher with premature closure of the proximal humeral physis (table 4). Attkiss and colleagues138 described an adolescent pianist with premature closure of the physis of the distal phalanx in the thumb, presumably caused by accumulated repetitive trauma incurred during years of piano playing. These reports are consistent with results from animal studies where prolonged intense physical loading inhibits or stops bone growth.139–144
In one case, radiographs of a young gymnast actually showed radiovolar opening of the distal radial physis and premature closure of the ulnar side of the distal radial physis.135 A similar finding involving the lateral side of the right proximal tibial growth plate in a young basketball player was described by Sato et al.119 These data are consistent with results from animal studies that show that an increased compression on one side of an epiphysis may prevent growth on that side, whereas normal growth occurs on the other side.145
Prevalence data for stress related physeal injuries are currently provided only for male and female gymnasts (table 7). Eight cross sectional studies report radiographic abnormalities consistent with distal radius physeal stress reaction in 10–85% of subjects.17,123,146–151 One cross sectional study92 reported partial closure of the left distal radial growth plate in three gymnasts (two girls and one boy).
Cross sectional studies of physeal injuries affecting gymnasts
Lishen and Jianhua152 reported on the nature and frequency of distal radius injury among 28 top level Chinese gymnasts who were followed and monitored radiographically over nine years. During this follow up, six of 18 girls and eight of 10 boys developed progressive wrist pathology. Initially, gymnasts developed chronic wrist pain associated with upper extremity weight bearing, with no radiographic abnormalities present. Next, x ray examination revealed stress changes involving the distal radial growth plate, with accompanying decreased range of motion at the wrist. Finally, radiographs revealed hindered radial growth and a relatively lengthened ulna.
The case, cross sectional, and cohort data reviewed indicate the existence of stress related injury and, occasionally, stress related physeal arrest. Along with results from animal studies, these findings suggest repetitive physical loading in excess of tolerance limits as a principle aetiological factor. Unfortunately, other potential aetiological factors such as nutrition, technique, and equipment have not been well studied.
REASONS FOR CONCERN
This review of the literature raises several important concerns related to growth plate injury among the paediatric athlete population.
-
Acute growth plate injuries do occur in sport and may account for as much as 30% of injuries, as reported in one study.78 However, the proportion of physeal injuries is probably much less, ranging from 1% to 12% of injuries depending on the sport.77,79–89 (table 3).
-
Although 71–75% of sport related growth plate fractures were associated with growth disturbance in two studies,27,68 the proportion of those with poor prognosis is probably much less, ranging from 0% to 37%.16,24,25,33,69–74 (table 2).
-
Type 1 and particularly type 2 Salter-Harris acute growth plate injuries are not as innocuous as originally described and may occasionally be associated with localised growth plate closure and osseous bridging.4,16,22–28
-
There are accumulating reports of stress related physeal injuries affecting young athletes in a variety of sports, including baseball, long distance running, basketball, football, soccer, gymnastics, rugby, tennis, and cricket. Although most of these stress related conditions resolved without growth complication during short term follow up, there are nonetheless several reports of stress related premature partial or complete physeal closure.102,119,134–136,150
-
There are two reports of varus changes subsequent to sports related stress injury to the distal femoral and/or proximal tibial physes (rugby and tennis players).120,121
-
There is a paucity of epidemiological data on the distribution and determinants of growth plate injury in organised sports.
Finally, it is of great concern that many coaches of children and youth sports, although enthusiastic and well meaning volunteers, are otherwise largely uninformed about the growth and development characteristics of children and youth and the appropriate care and prevention of athletic and particularly growth plate injuries.
INJURY COUNTERMEASURES
Although epidemiological data are lacking, it is evident that both acute and chronic physeal injuries occur in children’s and youth sports and that some of these injuries may be associated with growth disturbance. A disturbing finding is the growing number of reports of stress related physeal injuries affecting young athletes, including those affecting the lower extremities. Coaches and others associated with children’s and youth sports should be educated about the potential for growth plate injury and recommended strategies for prevention. The following preventive measures may be worthy of consideration.
-
Training and skill development should be individualised to reduce risk of acute and stress related physeal injury; in particular, coaches should reduce training loads and delay skill progressions for young athletes experiencing periods of rapid growth. Careful measurement of height at three month intervals will provide coaches with data to estimate growth rate. Height measurements should be taken at the same time of day (preferably in the morning) and should not be taken after a workout.
-
Coaches should use a variety of drills or activities during practice to avoid excessively repetitive movements that may result in overuse injury. Emphasis should be on quality of workouts rather than training volume.
-
Periodic physical examination should be carried out so that stress related growth plate and other overuse injuries can be diagnosed at an early stage and modifications made to the training programme to assist in the recovery process; when indicated, radiographs of symptomatic physeal areas should be administered to rule out stress changes.
-
Although data on injury prevention are lacking, physical conditioning, including strengthening, range of motion, and proprioceptive exercises, may help to reduce both acute and chronic physeal injury.
-
Trained personnel such as certified athletic trainers should supervise injury rehabilitation and return to practice.
-
Periodisation of training may also help to reduce stress related physeal injuries and prevent overtraining. This technique involves the systematic cycling of training loads over set periods of time with well defined rest periods.
-
When acute epiphyseal fracture involves a joint, it is recommended that the child not participate in contact sports for at least four to six months to prevent reinjury.4 Long term follow up is usually necessary to monitor the child’s recuperation and growth. Evaluation includes x ray examination of matching limbs at three to six month intervals for at least two years.153
-
For collision sports, such factors as maturity, fitness levels, and achievement and skill in the sport should be considered as possible criteria for equalising competition among chronological age peers and preventing unnecessary acute physeal and other injuries.154–156 A non-invasive measure for grouping young athletes has been proposed.157
What is already known on this topic
-
Both acute and chronic physeal injuries occur in paediatric sports; most resolve with treatment and rest, but some—particularly acute injuries—may result in growth disturbance
-
American football is the sport most often connected with physeal fractures, but most other sports are also represented
What this study adds
-
There is documentation of sport related physeal acute injuries affecting young athletes involved in a wide range of sports activities
-
There is documentation of sport related physeal stress injuries affecting young athletes involved in overhead, running-related, and upper extremity weight bearing sports
-
There is concern for the potential of growth disturbance and deformity secondary to sport related acute and chronic physeal injury
Finally, the channels of communication between the coach and the athlete’s doctor must be kept open so that young athletes can be assessed at the earliest opportunity should they develop symptoms. Severe pain around a joint, whether of sudden or gradual onset, may be the symptom of significant growth plate changes, which require examination by a doctor, prompt treatment, and specific recommendations about return to activity. A child should never be allowed or expected to “work through the pain.”
CHALLENGES FOR FUTURE RESEARCH
This scientific review of the literature underscores the need for prospective cohort studies to clarify the distribution and determinants of physeal injuries affecting young athletes. Important to this research is the meticulous documentation of growth plate injuries on injury report forms that include appropriate designations for both physeal and apophyseal injuries.
Prospective cohort studies should include analytical as well as descriptive components, so that possible risk factors and viable preventive measures can also be determined. Studies need to account for the multivariate nature of sports injuries by including as many relevant risk factors as possible.158 A risk factor of particular interest is whether periods of rapid growth relate to an increased risk of injury and, accordingly, whether training programmes designed to reduce the training loads during these periods may also result in a reduced risk of injury. Studies that test the effectiveness of pre-participation musculoskeletal screening are also recommended.
It is only through concerted collaborative efforts that optimal results can be achieved. The research team should include the coach, athletic trainer, doctor, and epidemiologist, who interact in a very dynamic manner. In addition, it is important to emphasise that every effort should be made by the research team to establish an open and trusting dialogue with young athletes and their parents. It is only after this is achieved that an adequate database can be established.
REFERENCES
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Footnotes
-
Published Online First 6 July 2006
-
Competing interests: none declared