Article Text

Abstract
Key questions regarding the training and physiological qualities required to produce an elite rock climber remain inadequately defined. Little research has been done on young climbers. The aim of this paper was to review literature on climbing alongside relevant literature characterising physiological adaptations in young athletes. Evidence-based recommendations were sought to inform the training of young climbers. Of 200 studies on climbing, 50 were selected as being appropriate to this review, and were interpreted alongside physiological studies highlighting specific common development growth variables in young climbers. Based on injury data, climbers younger than 16 years should not participate in international bouldering competitions and intensive finger strength training is not recommended. The majority of climbing foot injuries result from wearing too small or unnaturally shaped climbing shoes. Isometric and explosive strength improvements are strongly associated with the latter stages of sexual maturation and specific ontogenetic development, while improvement in motor abilities declines. Somatotyping that might identify common physical attributes in elite climbers of any age is incomplete. Accomplished adolescent climbers can now climb identical grades and compete against elite adult climbers aged up to and >40 years. High-intensity sports training requiring leanness in a youngster can result in altered and delayed pubertal and skeletal development, metabolic and neuroendocrine aberrations and trigger eating disorders. This should be sensitively and regularly monitored. Training should reflect efficacious exercises for a given sex and biological age.
Abbreviations
- UIAA
- International Mountaineering and Climbing Federation
Statistics from Altmetric.com
Rock climbing is both a physical and psychologically demanding aesthetic sport. Only very small parts of the hands and feet are in contact with the climbing surface whether climbing vertically upwards or more horizontally on an overhanging route as seen in fig 1.1 Elite-level rock climbing places extreme forces on the upper body extremities, specifically digital and upper-extremity strength.2–5 Relative strength is high in elite climbers as they must support and lift their body mass using a variety of finger grips, combined with complex vertical and lateral movement and position changes.2–13

Psychologically, the climber must manage the arousal of climbing a demanding and/or unknown route while puzzling out the most efficient technical moves required to minimise the intrinsic risk of falling or injury.5 13–16 Completing an unknown route first time without falling is referred to as an “onsight” ability, and is essential for competition. “Redpointing” refers to completion of a route after several attempts. Jean Piaget’s distinguished research places the developmental ability to solve abstract and formal problems between the ages of 11 to 15 years.17
Climbers typically seek out new route challenges to develop honed technical skills whether on artificial rock surfaces indoors or outdoors on specific rock types. The constant challenge of climbing unknown routes is extended to competitions where all the routes will be unknown to the competitor and cannot be rehearsed or specifically trained for. Little research has explored the psychological or neurogenic requirement of rock climbing at any age, though the former is a key element in accomplished climbers.13 15 16 18 19 The scope of this paper is restricted to the physiological aspects of climbing.
HISTORY AND AGE CATEGORIES OF COMPETITIVE CLIMBING
Rock climbing originated as a skill practice to train for short difficult sections of a long Alpine ascent. It has progressed to burgeon many new sub-disciplines such as technical difficulty climbing, speed climbing, bouldering and ice climbing.5 20
Two decades of sport climbing competitions in Europe and the former Soviet Union have secured rock climbing’s inclusion as an extra-curricular sport in many countries.20 The International Mountaineering and Climbing Federation (UIAA) arranged the first successive annual World Cup Climbing event in 1989 and participation in the 2005 International World Games Association.20 21 In 2006 the UIAA endorsed the creation of an International Federation to regulate competition climbing to meet Olympic Games requirements.20
Watts5 suggests that the most talented climbers in the last decade have been relatively young, though age was not specified. The 2006 male and female European senior climbing championship winners were aged 16 years, an age that can also found among adult World Cup finalists.22 Competitive climbing in some countries can feature unusually broad and overlapping age ranges. For example, one competition featured categories for: juniors aged 13–15 years, masters open to any age, open competition ⩾16 years and mixed veterans aged ⩾45 years.23 There is no known peak performance age in climbing (see table 1). This should not lead to the assumption that an adult’s training regimen is suitable for a growing young climber. The term “youngster” in this review refers to those aged 7–17 years.
LIMITATIONS OF EXISTING CLIMBING DATA
The inherent nature of the sport presents a challenge in standardising testing protocols for specificity and sensitivity to climbing ability.4 6 7 12 13 19 20 24–30 It combines dynamic gymnastic-like movements with static isometric position holds, explosive strength, stamina and intense isometric gripping function.
Table 1 summarises some of the difficulties posed when comparing studies. Climbing involves attempting new routes on different artificial or rock surfaces that are subjectively graded 5 15 19 20 25 and this grading system can vary among countries;19 20 the intensity of climbing exercise is influenced by a climber’s training, ability and experience;4 10 11 15 19 28 31 32 improved equipment and techniques continue to facilitate more technically difficult climbing that creates new higher grade abilities;5 33 and climbers are not necessarily brought to volitional fatigue.25 34–37 Performance terminating “climbing fatigue” is generally localised to the muscles responsible for gripping function.4 11 19 24 25 29 30
A trained adult climber’s heart has a similar cardiac response and morphological adaptation to that of a weight lifter as opposed to an aerobically led sport.38 It is characterised by a submaximal cardiac output,5 19 25 38 39 high heart rate4 6 12 28 29 34 38 40 and marked increase in peripheral resistance.19 29 38 41 This high isometric content of climbing prevents physiological data obtained from climbing exercise, for example blood lactate levels, from being directly compared with published isotonic exercise reference tables.4 11 12 34 36 Isometric exercise testing protocols are poorly related to dynamic athletic performance.4 12 35 42 Direct physiological data comparisons between climbing studies with a unique experimental design cannot be made.1–5 10 12 13 24 25 37 41 43–46
Sport-specific testing protocols with sensitivity and repeatability to common physiological variables in high-ability climbers are still being developed.4 6 7 9 10–13 24 26 27 For example, the use of handgrip dynamometry to measure handgrip strength is increasingly not used as a measured performance variable as it lacks specificity to climbing.1–3 5 26 27 30 40 41
SKELETAL, TENDON AND LIGAMENT GROWTH
Growth is a complex biochemical and biological process whereby predetermined genetic expression is maximally achieved only when favourable conditions operate throughout the entire period of growth.45 47–56 Developmental maturation of different tissues and bones occurs at different biological ages and is influenced by changes in endocrine function, especially during adolescence.45 49–52 57 Load-bearing exercise, for example in climbing or gymnastics, is positively associated with increased bone mineral content and mass compared with normative data.31 48 58 59 Inadequate body fat in a youngster can detrimentally influence bone growth and development and will be explored later.
Full skeletal maturation to adult proportions and biological function are not achieved until approximately age 19–20 years in women and 22–23 years in men. Skeletal maturation ends with epiphyseal closing once three distinct stages in linear growth have been achieved.45 47 48 60 The first stage lasting 2–3 years is characterised by a reduced pre-pubertal growth speed; stage two is an accelerated growth spurt; and in the final growth-ceasing stage >20% of adult final stature is achieved. This final stage normally occurs between the ages of 13–17 years: bone formation exceeds bone reabsorption processes and skeletal mass will increase approximately twofold, with the most critical period being between 14 and 15 years old.22 47 48 52 61 Pubescence is known to be a time whern there is an increased incidence of physeal fractures that often coincides with peak height velocity.61
A cross-sectional study of 5 461 girls aged 11 to 17 (mean age 13.9) years found 2.7% had a history of stress fracture, often underreported and untreated.62 Those subjects who participated in >16 h of exercise per week had 1.88 greater odds of developing stress fractures; leanness was also implicated with these fractures.62 High-impact sports, for example running or gymnastics presented the greatest risk factor.62
Mounting clinical evidence suggests that sports training of sufficient duration and intensity can precipitate pathological changes to the growth plate that may result in growth disturbance.61 63 Bone growth can be halted through shearing, avulsion and compression forces to produce deformity.61 63 64 Unlike adults, the physis on the epiphyseal plates in growing youngsters is two to five times weaker than the surrounding connective fibrous tissue.61 63 A force producing a ligamentous tear in an adult is likely to incur more damage in a youngster.61 63
Some research points to a 75–90% probability of developing an upper limb injury or overuse syndrome in climbing.65 Upper limb injuries, especially to fingers, are ubiquitous in adult climbing compared with injuries of the foot or lower limbs.31 66–84 The A-2 pulley rupture is a very common sport-specific injury on the volar aspect of the proximal phalanx.71 73 79
Where reported, high-ability climbers generally experienced more injuries, as routes with a higher grade place increased mechanical stresses and weight-bearing loads to the fingers. For example, an elite climber may be required to support their body using one or two fingers on difficult routes. Small handholds requiring the “crimp” position exert the greatest compressive force to finger joint cartilage, compared with the “open hand” position that is more protective.33 85 Using radiographic evaluation, Rohrbough et al. found a significantly higher (p = 0.010 to 0.036) osteoarthritis scores in five specific finger joint areas of experienced climbers (n = 65, age = 37.5 years, climb experience = 19.8 years, grade = 5.12c) compared with non-climbing age-matched controls.85 The overall osteoarthritis prevalence between both groups was not significant.85
Such evidence suggests there may be many unreported injuries in young climber’s fingers, especially those who can climb identical grades to those achieved by elite adult climbers.
Injuries to pubertal climbers’ hands
Hochholzer and Schöffl presented 24 case studies on pubertal climbers (age 14.5±0.9 years, 23 male, one female) with history of finger pain.22 Subjects experienced epiphyseal fractures on the proximal interphalangeal joint of the third or fourth finger. The former is typically a climber’s strongest finger. No single trauma was associated with any of the fractures. Repeated micro-traumas causing fatigue fractures to affected area were suspected. Medical histories revealed a trend whereby adolescent males undertook intensive finger strength training to compensate for their increased weight gain following a growth spurt. Climbers who delayed reporting joint pain, ignored medical advice and continued to train intensively, especially on the “Campusboard”, experienced permanent deformity of the affected finger with some loss of range of motion, as seen in ⇓figs 2 and 3.


The long-term effects of high impact and stress on the finger joints of young climbers cannot be predicted, as there are too few longitudinal studies to understand whether such changes may lead onto the early onset of osteoarthritis.22 31 86 87 This type of permanent damage could adversely affect a climber’s quality of life and future competitive career.
BOULDERING COMPETITIONS
“Bouldering” is ropeless climbing over a short distance that generally involves more intense and sustained anaerobic power moves.
To minimise the risk of digital damage and injury from uncontrolled falls at international bouldering competitions, the UIAA medical commission recently proposed, and the International Council of Competition Climbing accepted, that there should be a minimum age of 16 years for participation;88 that competitors should be able to safely fall 3 m onto a DIN 7914 standard (corresponding to 22 kg/m3) ground mattress a minimum of 30 cm thick; and that route-setters do not place handholds at the top of route that require great jumps to achieve.89 Many competition bouldering climbing teams include fall training and ankle stabilisation training, and use “spotters” to limit injuries from inevitable bouldering falls.21

KNOWN PHYSIOLOGICAL ADAPTIVE CHANGES TO CLIMBING
Climbers’ hands
Adaptive changes that characterise a veteran adult climber’s hands have been extensively documented to reveal a doubling in tendon width size, thickened finger phalanges and a tendency to have thicker fingers.22 33 72 A similar cortical hypertrophy of the bone in the finger phalanges in young rock climbers was found by Schöffl et al.72 86 87 This hypertrophy was positively correlated to climbing years, training hours and climbing level.72 86 87
Climbers’ feet
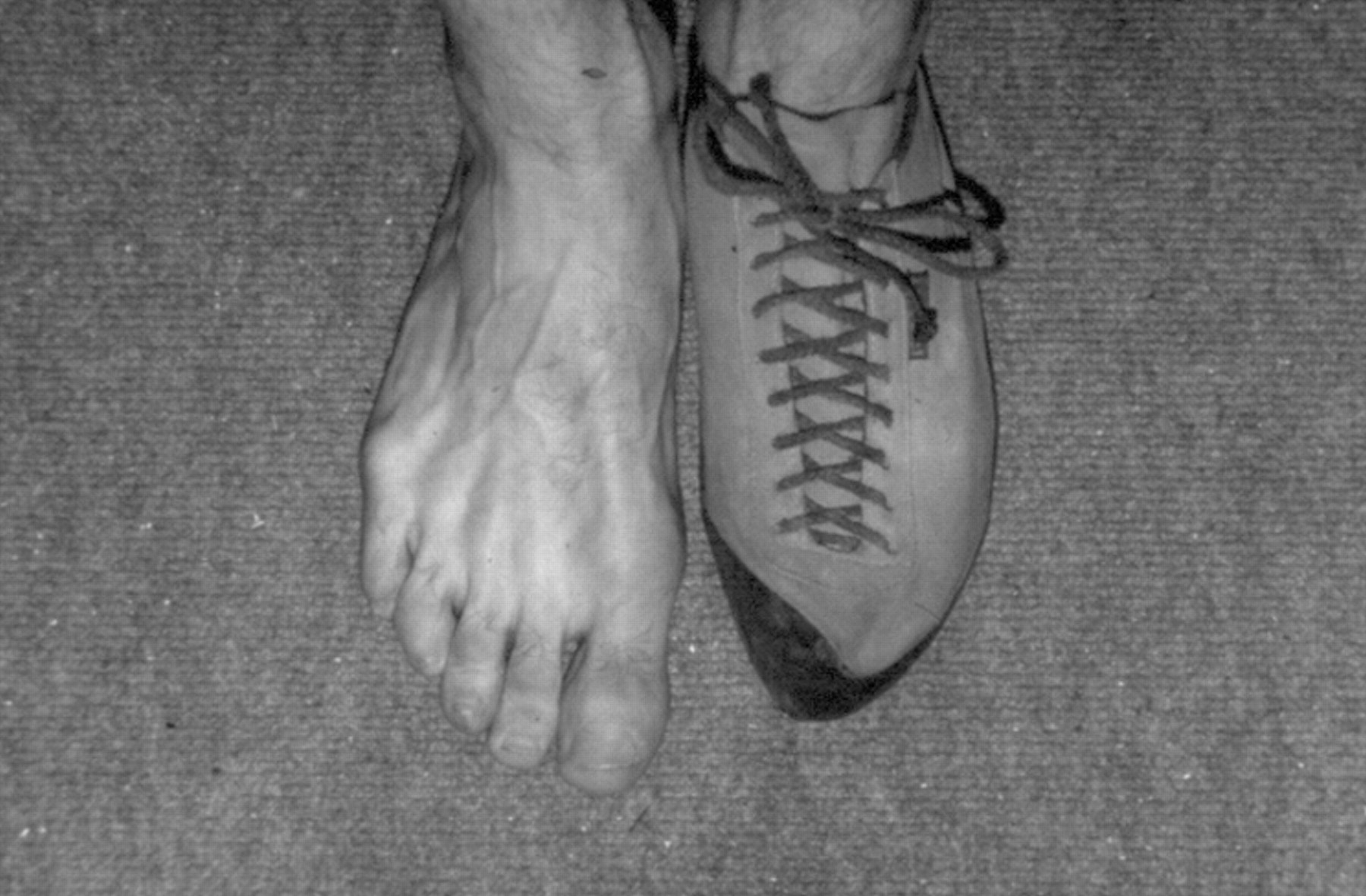
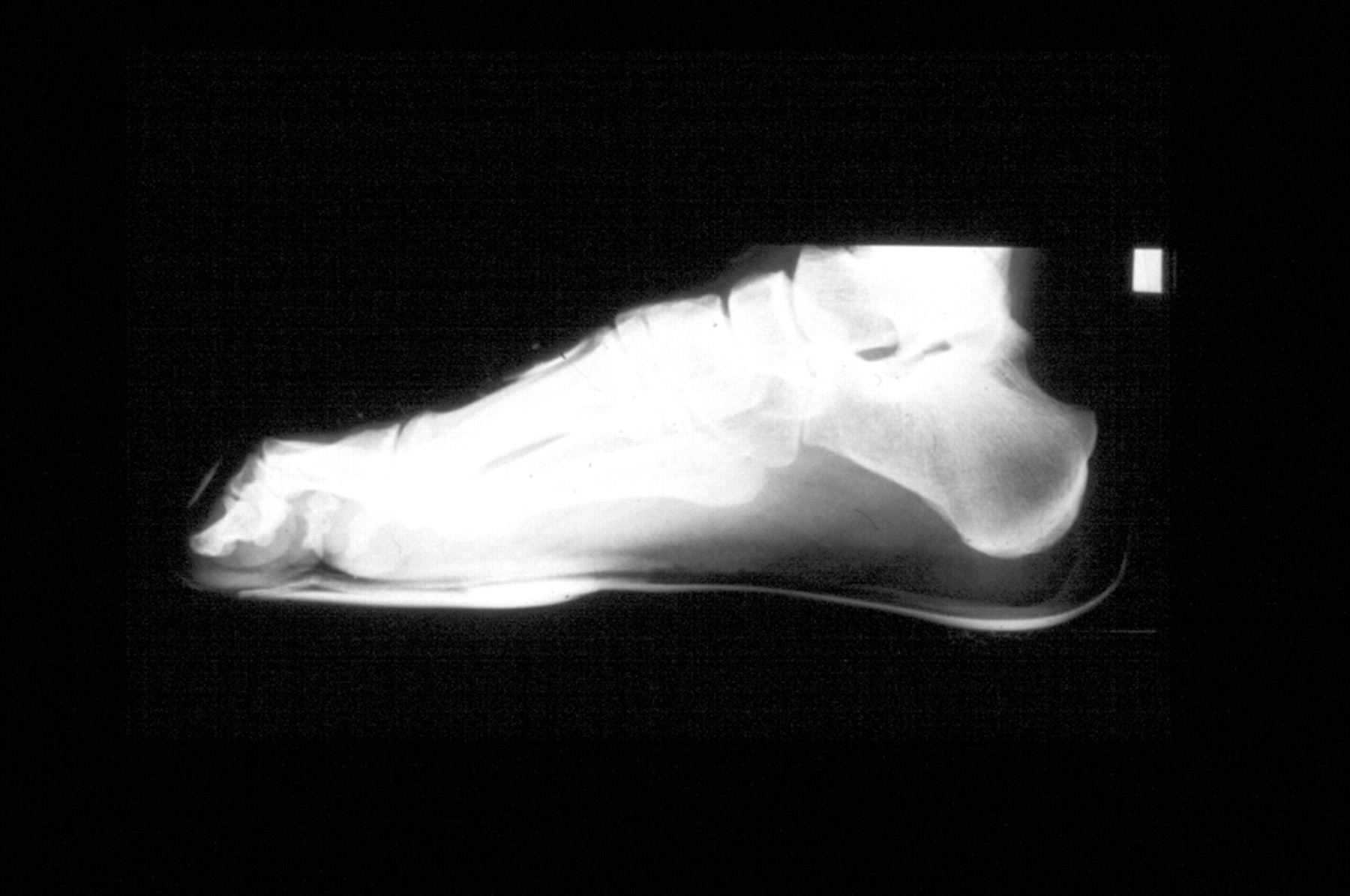
Climbing shoes should facilitate the ability to stand using friction with straight toes and on edges with bent toes with precision and proper contact.16 33 75 77 78 The majority of climbing foot injuries result from wearing climbing shoes that are unnaturally shaped or too small.76–78 High-ability climbers experience more foot deformities and injuries compared with climbers of lower ability due to the common practice of wearing climbing shoes sized smaller than normal street wear shoes (see ⇓⇑⇓figs 4 to 7).75 77 78 Only one paper77 on young climbers reported shoe sizes for both normal and climbing footwear: the mean was found to be 2.3±0.73 Continental sizes smaller in 19 junior competition subjects (Volker Rainer Schöffl, personal communication, 2007).⇓⇓


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Foot length and width increase in a linear fashion from the age of 3 to 12 years in girls and to 15 years in boys, after which growth plateaues.90 Foot length and width were also significantly correlated to body height in these 2 829 children aged 3 to 18 years with a coefficient of 0.96 to 0.98 for both sexes.90 Wearing excessively restrictive climbing shoes is not recommended to help achieve full growth potential and minimise the incidence of localised bouts of acute or chronic pain, injury or permanent deformity.75–78 91 92 Removing climbing shoes between climbs may also help limit such damage.
Adaptation’s of climbers’ hearts
Italian law mandates that athletes at all levels of competition have their hearts screened regularly, normally by echocardiograph. This Italian database is formidable, aptly demonstrated by Corrado et al.’s93 study on 33 735 young athletes. Delise et al.38 drew upon this database to create five classifications into which different sports could be grouped dependant on common characteristics of cardiovascular involvement. Climbing and sport climbing were categorised as:
sports with “pressure” cardiovascular involvement, characterised by submaximal cardiac output, high to maximal heart rate and moderate to marked increase in peripheral resistances38
The dimensions of the left ventricular diastolic cavity in isometric sports have high values for wall thickness relative to the cavity capacity.94
From limited metabolic data of short duration obtained on adult climbers, an adult Vo2peak is estimated to be 52–55 ml·kg−1·min−1, averaging 20–25 ml·kg−1·min−1 during an ascent.5 6 19 This reinforces the isometric rather than isotonic aerobic quality95 of climbing, and would reflect the climbing sub-discipline tested.24 34 Bar-Or, designer of the Wingate anaerobic test, found that Vo2 was unchanged in children aged 6–15 years and this corresponded to approximately 49 ml·kg−1·min−1.96 Such data suggest that children can almost match an adult climber’s Vo2peak without any additional training, and that aerobic potential is not a limiting factor to climbing performance.
Development of anaerobic potential is more limited in children and will be explored later.97 98
Back pain
There are major differences in the diagnosis of back pain in young athletes versus adults.64 The stress fracture of the pars interarticularis at the base of the spine, or spondylolysis, is often overlooked in young athletes.64 99 Symptoms include a complaint of focal low back pain, although the pain can also extend into the buttock or legs. Sports with causative mechanisms such as lumbar hyperextension and rotation found in rowing, artistic gymnastics and throwing sports record high spondylolysis prevalence rates (16.88%, 16.96% and 26.67%, respectively) compared with the general population (3.0% to 8.02%).100 Climbing also involves these causative mechanisms.
Reports suggest climbing may precipitate the development of spondylolysis, but its prevalence has not been investigated.33 Anecdotal evidence in veteran adult climbers of spondylolisthesis has been reported.33 Spondylolisthesis refers the overuse deterioration of a spinal disc that causes it to slip out of alignment.
IMPROVED ATHLETIC PERFORMANCE TIMEFRAMES IN YOUNG ATHLETES
Distinguishing the independent effects of training from those of normal growth and other confounding factors is difficult due to the shortage of longitudinal studies. Viru et al.’s101 global meta-analysis of 31 studies and 11 reviews of the annual increases and improvements in motor abilities for youngsters, summarised in table 2, was based mainly on cross-sectional data. Viru’s timeframes for strength improvements are strongly associated with the latter stages of sexual maturation and specific ontogenetic development, as in the testosterone-dependent muscular hypertrophy found in male adolescents.101 Sexual maturation is associated with the phenomenon of “outgrowing one’s strength”.101 The rate of improvement in motor abilities declines at ages closely associated with the second and third stages of sexual maturation, and may cease at approximately age 16 years in boys and 14 years in girls.101
The mean age of 14.5±0.9 years reported in Hochholzer and Schöffl’s22 case studies of 24 climbers (23 adolescent males) with finger fractures coincides with Viru’s101 timeframes for improvements for strength and speed, “outgrowing one’s strength”, as well as the critical age between 14 and 15 years old when skeletal mass increases approximately twofold and is at greater risk of injury.47 48 52 61 The influence of training and rapid growth at this age is further supported by examination of red blood cell count, packed cell volume and haemoglobin concentration in 876 intensely training athletes (age 14.01±0.06 years) compared with controls.102 All measured variables were reduced more in the athletic group versus controls, and the male athletes experienced the greatest reductions.102
DIFFERENCES IN THE YOUNGSTER’S METABOLISM
Children as young as 12 years old are “metabolic non-specialists”; they do not exhibit the specialised metabolic response to their sport as occurs in adults.96 97 103–105 Unlike adults, children metabolise fat, rather than carbohydrate, for energy when undertaking either prolonged or short, intense exercise.96–98 103 Until sexual maturation occurs, the quantities of several essential anaerobic enzymes are simply inadequate to sustain isometric contractions and support heavy loading.96–98 103 The metabolism of an adult’s tendons and ligaments demonstrates oxygen consumption is reduced by 7.5 times compared with skeletal muscles.106
Thirst and pain homeostatic feedback mechanisms are immature in children and require careful monitoring.63 64 96 104 105
SOMATOTYPE OF CLIMBERS
Watts5 suggests that the shift in the 1990s to adding severe overhangs to competition routes may have resulted in the physiological demands of the sport to favour mesomorphic ectomorphs of a shorter stature.107 The rationale offered was that the resistance forces associated with moments would be greater for taller climbers whose distal extremities were further away from their torso’s centre of gravity, and the possible increased body mass in taller climbers may result in climbing fatigue being experienced earlier,107 as demonstrated in fig 1.
Some studies suggest that the increased arm span to height ratio in elite climbers may be a selective trait at that level,13 107 although other authors suggest trainable variables are more selective of higher climbing ability.4 7 19 24 27 28
The biomechanical theory about an ideal height and arm span for climbing has not been investigated, but some racial differences are known to exist. Yun et al. measured 10 322 healthy Korean children to determine whether any correlations existed among height, leg length and arm span.108 Yun found that arm span in the shortest children never exceeded height, and that in tall boys arm span growth accelerated between puberty to age 17 years and remained increased.108 Black people have relatively long limbs, while Asian people tend to have shorter limbs.54 Ethnicity is not reported in climbing studies.
The evidence shown in table 1 is inadequate to characterise an elite climber’s somatotype at any age, but successful adolescent athletes aged 12–18 years generally exhibit common sport specific somatotyping to a successful adult athlete.46 59 It may be useful to establish elite adult climbers’ somatotyping by measuring the girth, length and breadth of the limbs, and trunk area, body mass and composition, and possibly ethnicity.
SPORTS REQUIRING LEANNESS TO BE COMPETITIVE
The widespread anecdotal view amongst climbers that reduced body fat improves performance has not been investigated,19 although elite climbers often have low levels of body fat.4 13 28 32 57 85 104–112 114–117 The determination of an athlete’s optimal body weight and composition for health and competition should be done individually as they are strongly influenced by age, sex, genetics and the requirements of the sport.46 113
The estimated minimum amount of body fat in adults that is compatible with health is 5% in men and 12% in women.46 Reference tables detailing what the minimum fat percentages should be in growing young athletes are unknown.43 44 113
Watts’107 elegant investigation of 90 competition climbers aged 13.5±3 years found that they were at or below the 50th centile for sex- and age-matched normative data and athletic controls when measured for height, weight and body fat (p<0.01). No measures of biological maturity or genetic predictions of final stature were recorded in this or any other study known to the author on young climbers. It is not known whether these shorter and leaner competitive climbers were the result of selection, training duration and intensity and/or dietary habits.
Failure to attain full genetic height potential may have several different causes.54 Pre-pubertal growth is dominated by the accelerated growth of the lower body, while post-pubertal growth is dominated by the accelerated growth of the trunk with some genetic variation.52 54–57 Site-specific bone growth deficits may occur for a wide variety of reasons, including exposure of intense training or negative energy balance that can reduce levels of insulin-like growth factor 1.45 50 52–55 57 For example, as gymnasts’ high-impact sport-specific training begins pre-pubertally, they can have marked stunting in leg-length growth52 compared with rhythmic gymnasts and swimmers whose training presents active loading but low impact exposure.50 55–57
Caine et al.55 reviewed gymnastic studies from 1966 and found that competitive gymnasts were clearly identified by their attenuated growth that was followed by catch-up growth, though not always reversed, once training was reduced or when following early retirement. Caine suggests regularly plotting growth velocity charts from pre-pubescence and referral for complete evaluation of underlying pathologies whenever height is in the lower fifth percentile or there is a downward trend of growth indices across two major percentile lines.55
Watts’ study reported that the finalists for both sexes shared similar body fat measurements of 9.6±1.9% at age 13.5±3 years.107 The possible implications of this low body fat pre- and post-pubertally will now be explored. A highly correlated positive relationship was found between total body fat mass and bone mass and size (p<0.001) in 3082 children by repeating DXA measurements at ages 9.9 and 11.8 years.118 In girls, this positive relationship was maintained to pre-pubertal Tanner stage 1 (p<0.001).118 Clarke suggests that fat mass may act to increase bone size by stimulating radial, as opposed to longitudinal, bone growth by increasing the rate of periosteal apposition.
In adolescence, the combined or independent factors of maintaining of a negative energy intake and low body fat can alter and delay pubertal development, contribute to metabolic and neuroendocrine aberrations, affect stature, detrimentally affect bone growth and integrity in the short and long-term, increase the risk of injuries including stress fractures, and trigger eating disorders.45 46 49–52 54–57 62 112 118 Disordered or restrictive eating patterns are reported in elite adult climbers.20 109 110 113 Regardless of training volume, aesthetic sports requiring leanness for competition typically have a high incidence of delayed menarche, menstrual dysfunction and eating disorders in both sexes.46 50 57 112 Disordered eating, amenorrhea and osteoporosis are the three interrelated components that make up the “female athlete triad”. Kahn et al. present a strong case for including osteopenia in the triad definition.116 Where one triad component exists, the other interrelated components must also be investigated as the consequences and can be time-dependent, and possibly irreversible.46 52 116
Other research suggests that the deleterious catabolic and hormonal effects on health and performance of maintaining a negative energy balance and low body fat, especially after an intensive workout, are greater than those posed by the workout itself.46 57 111 117 Lipid and apolipoprotein profiles in young female athletes aged 10 to 15 years may be due to differences in physical activity rather than dietary intake.115 Therefore both the timing and appropriateness of the dietary intake are both important factors for health and performance.
CONCLUSIONS
Based on evidence presented in this review, the following considerations are suggested when designing training programmes for dedicated young climbers:
Climbers aged <16 years should not undertake intensive finger strength training and cannot not participate in international bouldering competitions.
A force producing a ligamentous tear in an adult is likely to incur more damage in a growing youngster as the physis on their epiphyseal plates is two to five times weaker than the surrounding connective fibrous tissue.
The final pubescent growth spurt is associated with an increased risk of injuries and physeal fractures.
Up to about 12 years old, children have a limited capacity to develop an adaptive metabolic response to specific training, but possess an accelerated ability for motor development.
This suggests the emphasis of training should be on climbing an increased volume and diversity of climbing routes to improve fluency and mechanical efficiency of climbing techniques, as opposed to increasing intensity.
Wearing excessively restrictive climbing shoes is not recommended in growing feet to help prevent foot injuries and deformities. Regular record-keeping of street wear and climbing shoe size may be a useful strategy up to a minimum age of 15 years.
Growth velocity charts and measures of body fat should be sensitively and regularly plotted. If possible, menarche age and cycle details should also be collected. Referral for complete evaluation of underlying pathologies should be undertaken whenever height is in the lower fifth percentile or there is a downward trend of growth indices across two major percentile lines. This may also reveal whether a climber’s growth curve is characteristic of an early maturer, as in a swimmer, or that of a late maturer, as in a gymnast.
Climbers should be educated in the importance of an appropriate diet and timing of this intake on health and performance.
The incidence of spondylolysis has not been documented and warrants investigation.
The age at which a climber should specialise in climbing is unknown.
Knowledgeable and qualified personnel should carefully monitor training. Where training intensity is increased, it should reflect safe and efficacious exercises for a given sex and biological age, independent of the competition calendar.
More research on young climbers is needed.
What is already known on this topic
Data on young climbers are rare. Studies revealing the physiological response to various climbing sub-disciplines in adults are limited. Adult studies generally feature males, identification of sport-specific injury and injury patterns, basic anthropometrical data and development of unique sport-specific testing protocols differentiating trainable variables in elite climbers.
What this study adds
This study initiates an evidence-based foundation to help inform the development of a long-term athletic training programme for dedicated young climbers. It incorporates known physiological developmental issues common to all young athletes alongside known physiological variables in climbing. An elite adult climber’s training regimen is inappropriate for an elite young climber, even if they climb or compete on identical routes.
Acknowledgments
The author thanks Steve Gorton for the photograph of a young competition climber.
Abbreviations
- UIAA
- International Mountaineering and Climbing Federation
REFERENCES
Footnotes
Funding: None.
Competing interests: None.
Linked Articles
- Review
- Review
- Miscellaneous