Article Text

Abstract
Football is the most popular sport on earth. When a young, fit popular player suddenly collapses and dies during play, the tragic event is frequently screened and publicised worldwide. The reported incidence of sudden cardiac arrest (SCA) varies from 1:65 000 to 1:200 000 athletes. A broad spectrum of cardiac and non-cardiac causes have been implicated, and regular precompetition medical assessments are recommended as a preventive measure. Immediate cardiopulmonary resuscitation and early defibrillation is the treatment for SCA. High success rates can be achieved if this is initiated promptly, preferably within seconds of the arrest. Trained medical responders must be allowed to respond, ideally with a defibrillator (manual or automated) in hand, to a player who suddenly and unexpectedly collapses and remains unresponsive on the field. Immediate defibrillation of a pulseless ventricular tachycardia or ventricular fibrillation, within 1 to 2 min of onset, has a successful cardioversion rate exceeding 90%. Medical responders should be well trained and rehearsed in the recognition of SCA, including distractors such as seizures, myoclonic jerks and agonal (gasping) breathing. Prompt initiation of chest compressions on the field, together with early defibrillation, will result in many athletes' lives being saved by immediate implementation of these simple recommendations.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://bjsm.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
Football (soccer), is the most popular sport on earth, with 260 million registered players1 representing 208 national football associations and a media viewership of billions. A number of football players reach the level of iconic stardom and are perceived by many young followers as role models to live up to. Therefore, when a young, fit, healthy, popular football player succumbs on the field of play to a sudden cardiac arrest (SCA), particularly when viewed on live television, it becomes a tragic event with catastrophic effects to the family,2 3 followers and to the football family worldwide.4 Such a tragic event is beyond most people's imagination or expectation, for it involves elite athletes who are at the pinnacle of health and success. The collapse and sudden cardiac death (SCD) of Miklós Fehrér, Marc-Vivien Foe, Daniel Jarque, Antonion Puerta and Phil O Donnel5 are vivid examples of this tragic event.
Definitions
SCA can be defined as the sudden, unexpected cessation of cardiac output, usually of cardiac origin but not necessarily so, in a previously healthy appearing individual. SCD is defined as the sudden, unexpected natural death occurring within 1 h of the onset of symptoms in a person who appears to be healthy or afflicted with a medical condition that is not considered fatal.6 7 An athlete, and hence a football player, is a person participating in an organised team sport that requires systematic training and regular competition against others, and that places a high premium on athletic excellence and achievement.8 9
Incidence
The true incidence of SCA among footballers is not known,10 but can be predicted from available data in team-based athletes which reports an incidence of 1 in 65 000 athletes to 1 in 200 000 athletes,11,–,13 which in USA appears to equate to one SCA every 3 days14 and is 2.5 times higher than in non-athletes.15 A prospective population-based study of SCD in young competitive athletes in the Vento Region of Italy indicated an incidence of SCD of 2.3 per 100 000 athletes per year from all causes, and 2.1 per 100 000 athletes per year from cardiovascular diseases.16
A further problem is the realisation that the reported figures are probably underestimated due to the absence of either postmortem results and/or mandatory reporting of SCA in sports in many countries including the USA. Whatever the true incidence may be internationally, there is no doubt that SCD is the leading cause of death in exercising young athletes11 17 and all efforts must be undertaken to prevent its occurrence by screening procedures such as the precompetition medical assessment,18 19 or when necessary, through efficient and effective emergency treatment.20
Causes of SCA
A broad spectrum of cardiac and non-cardiac causes, both congenital and acquired, have been implicated in causing SCA in athletes. Similar to other estimated data concerning SCA in athletes, the exact numbers cannot be accurately quantified. However, from what is available from the USA and Italy, it appears that structural cardiac disease accounts for 60–95% of the causes of SCA,21,–,23 and mainly includes hypertrophic cardiomyopathy, arrythmogenic right ventricular dysplasia and congenital coronary artery anomalies in the under-35-year-old group, and coronary artery disease in the over-35-year-old group, all of which induce ventricular fibrillation (VF) as the main presenting rhythm in SCA.24 In the under-16-year-old age group, commotio cordis (cardiac contusion) is thought to be responsible for up to 20% of SCAs. It is very uncommon after 21 years of age.25 26 Commotio cordis is the induction of VF during the vulnerable repolarisation period of the myocardium due to a blunt, non-penetrating, usually high velocity, blow to the chest either from a small solid object,27 including a football28 or from contact with another player. Other cardiac causes of SCA include myocarditis, ruptured aortic aneurysm, aortic valve stenosis, mitral valve prolapse, dilated cardiomyopathy, drug-induced cardiac arrhythmias and the ion-channelopathies29 which include the long and short QT syndrome (caused by sodium or potassium ion channel genetic mutations), Brugada syndrome (defective sodium channel gene) and familial catecholaminergic polymorphic ventricular tachycardia30 (abnormal ryanodine receptor regulating calcium release). Non-cardiac causes of SCA include asthma, heat stroke, cerebral artery rupture and exertional rhabdomyolysis secondary to sickle cell trait.
Field identification of SCA
It is common during a football match for players to collapse on the field, mainly following contact with an opponent, for either a genuine or spurious31 injury (figure 1). The majority of these incidents are resolved with little therapeutic intervention from the team physician within a few minutes. According to the International Football Association Board Rules of the Game, if a player appears injured, the referee may stop play, approach the injured player and assess whether medical assistance is required. Once the referee has determined that medical assistance is required, they will then authorise one, or at most two doctors, to enter the field.32 This applies to the sideline medical stretcher bearers as well. A consequence of this rule, when response is required to a collapsed player, is some delay in waiting for the referee to first approach the injured player, determine the urgency of the situation and if needs be, summon the medical responders onto the field.33
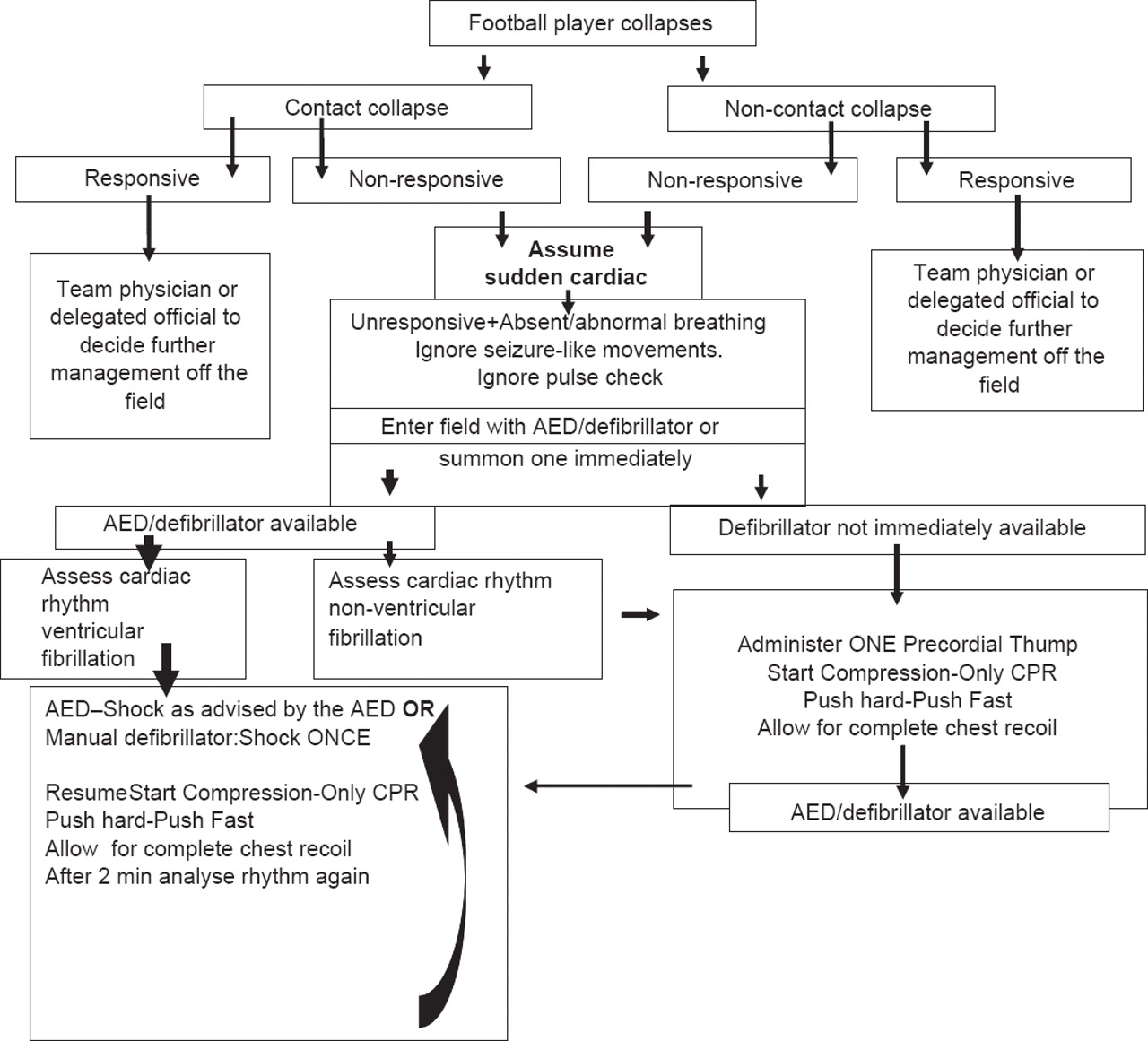
{kind=link}
On field SCA management algorithm.
If a player collapses to the ground as a consequence of bodily contact with an opposition player during competition, the referee is nearby and will visualise the incident and thus be in a position to respond to the injured player immediately. Were they to ascertain that the collapsed player is unconscious, they should summon medical assistance without delay. However, if the player collapses without having had any contact with either an opposition player or ball, particularly if it is out of sight of the referee, whose attention will be focused on the area of active play, this could substantially delay their awareness of the incident, and a much needed speedy response for life-saving assessment and treatment which is mandatory in SCA.34
From an emergency planning perspective, it would be highly advisable to revise the current Laws of the Game, to include ‘an exception’ that states that whenever a football player collapses on the field of play without there having being any contact with another player, the ball or physical object, this situation must be regarded as a SCA (until proven otherwise), with immediate response from the sideline (with a defibrillator) by the medical personnel on duty (team physician, physiotherapist, medical stretcher bearers and/or coach) without prior authorisation from the referee on the field, but with notification of the fourth official at the sideline.
Another major impediment to rapid recognition of SCA in athletes on the field of play, once they have collapsed, is the apparent signs of life that are evident in the first minutes after collapse. In over 50% of SCA in athletes, brief seizure-like activity or involuntary myoclonic jerk-like activity is present immediately after collapse.35 Thus, seizure activity may be the first obvious sign as to the cause of collapse to the responding referee or surrounding players nearby. Myoclonic movements after SCA are postulated to be due to oxygen deprivation to the brain as a result of the non-perfusing cardiac arrhythmia. To the unsuspecting responder, these seizure-like activities may appear as an epileptic seizure36 with consequent delay in critical initial management steps for SCA including cardiopulmonary resuscitation (CPR) and external defibrillation. To avoid these life-threatening delays in diagnosis and management after SCA, any athlete who collapses on the field of play and is unresponsive must be regarded as being in life-threatening cardiac arrest until it is proved otherwise.37 Accordingly, seizure-like activity must be regarded and taught as a sign of SCA and not as a standard tonic–clonic seizure per se, and training of CPR and automated external defibrillator (AED) use for potential first responders in sports environments is strongly recommended.
Another major obstacle to rapid recognition of SCA on the football field is the presence of abnormal or agonal breathing38 in SCA patients during the first few minutes of arrest while the brain has sufficient oxygen supplies. Standard CPR training since 200539 has emphasised that the apparent lack of normal breathing patterns is to be regarded as a sign of cardiac arrest and if present in an unresponsive person, equates to a diagnosis of cardiac arrest, with immediate activation of an emergency action plan and emergency medical services. In addition, the inability to adequately assess the presence or absence of a pulse has led to its detection being removed from layperson CPR training and is likewise de-emphasised in healthcare professionals.
Sportspersons and other potential first responders, must make every effort to respond expeditiously to the side of a collapsed footballer, particularly if no contact has occurred. If unresponsiveness is established, SCA should be regarded as being present, despite apparent signs of life, with activation of the emergency action plan which includes immediate CPR and defibrillator retrieval. It must be left up to experienced responding healthcare professionals to determine otherwise.
On-field emergency management
The management of SCA has been described in many puvblications, most incorporating the 2005 International Liaison Committee on Resuscitation (ILCOR) guidelines. SCA is dominantly a cardiac arrythmogenic event with VF the dominant arrhythmia40 in 90% of cases. The treatment of this lethal condition is immediate external defibrillation, preceded, if defibrillation is not immediately available, by CPR. The single greatest factor affecting survival from SCA is the time interval from cardiac arrest to defibrillation.41 42 Each minute of delay in initiating defibrillation after SCA leads to a 10% decrease in shock success.43 The internationally recommended target from the ILCOR39 from collapse-to-current (shock) is a3–5 min. To achieve a rapid response practically involves prompt collapse recognition, rescuer activation, retrieval of the defibrillator, arrival at the patient's side, attachment of the defibrillator and arrhythmia recognition and defibrillator charge and delivery of the first shock. In 2005, the American College of Cardiology 36th Bethesda Conference recommended that every school hosting sports activities must have access to a defibrillator within 5 min of a patient's collapse.44 In 2007, an USA Inter-Association Task Force on Emergency Preparedness and Management of Sudden Cardiac Arrest in High School and College Athletic Programs recommended access to AEDs with a target goal of less than 3–5 min from collapse to current.45 Practically, these recommendations imply that for defibrillation to occur reliably within 3–5 min of activation, an on site defibrillator (AED) is required.4 Luiz et al46 described 13 witnessed cardiac arrests in spectators over a 6–7-year period in the Fritz–Walter Football Stadium that provided CPR within 2 min and defibrillation with 4 min resulting in a successful resuscitation rate (survival without neurological deficit) of 62%. Conversely, an initial study by Drezner37 analysed a series of nine SCA cases among college athletes, of whom seven were in VF who received initial defibrillation shocks within 3.1 min, yet only one of the nine sadly survived. Diagnostic studies in the lone survivor indicated no structural heart disease. It may therefore appear that that the 3–5 min ‘timing goal’ may be insufficient for SCA with VF occurring on the field of play,47 48 particularly those players who have underlying structural myocardial disease or commotio cordis as the underlying cause of VF. In an animal model of commotio cordis49 in which external defibrillation was undertaken within 1–2 min of VF, successful resuscitation occurred in 100% and 92% of animals, respectively. In the same experiment, only 46% of defibrillation shocks were successful after 4 min of VF, and after 6 min successful resuscitation decreased to 25% (p<0.0001). The success of early defibrillation in young athletes with SCA has been demonstrated in a recent report by Drezner et al showing a 64% survival rate in high school athletes with SCA treated promptly by an on site defibrillator.35 Consequently, it must be recommended that in order to expeditiously3 defibrillate a player with SCA on the football field, one should strive for a 1–2 min collapse-to-shock time goal, and it should be mandated that a defibrillator always be available at the sideline, either near the forth official at the midline, or with one of the medical stretcher teams, who should all be adequately trained in SCA recognition and on-field medical management as a matter of course.
If, for whatever logistical reason, there is at least one defibrillator available in a football stadium, whether housed in a medical centre or on-duty ambulance, it should be transferred to the side of the field during the football match, with its whereabouts known to all, including team physicians, team physiotherapists, venue medical officers, doping control medical officers, coaches and related medical personnel. The often observed practice of positioning a defibrillator in a medical centre inside the stadium for use in a collapsed spectator or inside a ‘player’ medical centre, without regard to positioning one at the field side requires serious review and revision. The current guidelines for medical services at Fédération Internationale de Football Association (FIFA) competitions by the FIFA require a defibrillator at the sideline. Emergency preparedness for SCA in spectators, especially at large football arenas, must also be considered.50
It must be appreciated that although an AED is considered basic life support and the external defibrillator of choice in developed countries, this may not be realistic in many countries where AEDs are not readily or absolutely available. In these situations, use of manual defibrillators, either monophasic, or if available, biphasic will be just as relevant and applicable, and may be a better choice, if the relevant training and experience is present. It is important in these situations that medical personnel have adequate knowledge of the specific defibrillator that they may be called upon to use, specifically the energy setting. It is recommended that the joule (J) setting for all monophasic defibrillators be set at 360 J initially, biphasic rectilinear defibrillators at 120 J and biphasic truncated exponential defibrillators at 150–200 J. In the event that the type of defibrillator and hence energy setting is not known to the operator, the suggested initial default setting is 200 J.51
Immediate precordial thump
Much transatlantic speculation and anecdotal banter continues to effect the performance, if at all, of a precordial thump in a witnessed cardiac arrest prior to initiation of CPR when a defibrillator is not immediately available.52,–,54 Maron3 describe a case of a 14-year-old with SCA after a forceful collision with a teammate who was initially administered ‘a forceful chest thump’ by a physician bystander followed by standard CPR. The patient regained a spontaneous pulse after 90 s postincident. More recently, Madias et al55 found precordial thump in an experimental model to be effective for ventricular asystole but not for VF while the Resuscitation Council (UK) still has the precordial thump in its guidelines.56 In view of the absence of hard scientific data for or against the administration of a precordial thump in witnessed SCA and the slim chance that it may contribute towards a successful outcome, it is still to be recommended in those situations of SCA where a defibrillator is not immediately available, which unfortunately, internationally, may occur frequently in the football playing world.
External chest compression
The initiation of CPR to a victim of SCA must be undertaken as speedily, safely, effectively and efficiently as practically possible, particularly if there is any delay in the immediate provision of a defibrillator. If the SCA has occurred after forceful contact of two players, it is possible that the victim of SCA may have fallen to the ground while unconscious, thus being unable to protect their spinal column from damage during impact with the ground. In such a case it must be assumed that an unstable cervical spine with potential injury is present and unnecessary uncontrolled movements during resuscitation should be avoided without compromising the resuscitation. If the victim begins to regurgitate (vomit) stomach contents during CPR, turning the player should be accomplished with due control and care.57 58 Since December 2005, when the last revised set of recommendations for CPR and Emergency Cardiac Care from the ILCOR were published, the provision of standard CPR has encompassed the following guidelines:
▶ recommendation of a universal external chest compression-to-manual ventilation ratio of 30:2 for single rescuers for victims of SCA including adults, children and infants;
▶ provision of effective, efficient rhythmic external chest compressions at a rate of 100 compressions per minute with complete chest recoil after each compression—‘push hard, push fast’;
▶ minimising interruptions in chest compression in order to maximise blood flow;
▶ external chest compressions must resume immediately after every defibrillation shock and continue for a minimum of 2 min before the rhythm analysis is repeated;
▶ CPR providers should consider changing roles with other providers after 2 min of external chest compression, to prevent fatigue induced inefficiencies in external chest compression;
▶ manual breathing via mouth-to-mouth with or without a barrier device or mask-to-mouth must be accomplished as effectively and efficiently as possible, ensuring that the chest rises with each breath, but without delaying external chest compressions.
Although there should be no shortage of persons available on and around a football field that can initiate effective and efficient CPR at international level competitions, this might not always be the case at practices or lower level competitions and in countries with less developed emergency medical services. Additionally, standard compression-ventilation CPR is regarded as a complex set of skills59 to initially muster and once acquired is prone to memory decline issues with time. The development and acceptance of external chest compression-only CPR (hands-only CPR, without ventilation) may be the answer to ensuring that immediate CPR will be effectively, efficiently and immediately undertaken on the football field during a SCA because of a number of practical and pedagogic advantages:60,–,65
▶ the only skill that is required is the performance of manual external compression (MEC) of the chest;
▶ active manual ventilation can be omitted for up to 10 min, as the football player is fully oxygenated before the onset of SCA;
▶ MEC is easily taught to any bystander and can be effectively administered with minimal supervision;
▶ minimal interruption with continuous external chest compression results in higher coronary perfusion pressures and greater blood flow;
▶ there are fewer objections to MEC from infectious or aesthetic concerns compared with standard CPR with mouth-to-mouth ventilation;
▶ the success rates with external chest compression-only CPR is at least similar to standard CPR.
It is recommended that chest compression-only CPR be considered as the most effective means of training large cadres of players, coaches and other likely responders in the football environment and that it be promoted as the initial method of CPR in the presence of a SCA, in conjunction with defibrillation.66 67 In South Africa, the Resuscitation Council of Southern Africa has endorsed the need to simplify the training of CPR, promoting a basic course named Simply CPR,68 where CPR represents:
▶ Call—for help if the victim is unresponsive;
▶ Push—on the chest if the victim is not breathing normally;
▶ Recharge—the heart with an external defibrillator or AED.
Planning, education and training
SCA will continue to occur on the football field, with and without preparticipation cardiac screening, even though efforts to broadly implement the latter is an important preventive measure. What cannot be totally prevented must therefore be managed when it does present. The medical management of SCA on the football field can only be effectively, efficiently and expeditiously managed if it is planned for beforehand with a known and distributed emergency action plan. This involves education and training of likely responders, availability of emergency equipment and regular updates and rehearsals. Simply CPR has been shown to adequately train classes of bystanders in 30 min by emphasising its three fundamental steps of call, push and recharge. It is of vital importance to instil in the football players, the physical trainers, coaches and football management personnel the basic understanding of a medical emergency action plan in the event of a life-threatening event during training or competition, and the invaluable part that each can contribute to a successful outcome. In the event of SCA in the football environment, multiple rescuers should be available to assist in CPR and defibrillator use. This means that multiple tasks can be undertaken simultaneously, especially if regular training is undertaken prior to the event. Failing that, it takes one trained person to adequately supervise a number of players or officials.
Conclusion
SCA is a catastrophic occurrence when it occurs because it may lead to the death of a young, fit, healthy popular football player. Preparticipation screening can do much to prevent such events, but it has limitations which ensure that SCA will continue to occur on the football field as well as in other sporting facilities. Nothing short of an established emergency action plan which is rehearsed and includes adequate numbers of motivated trained responders utilising appropriate life saving equipment69 and located in strategic positions during active training and competition, will afford the chance of a successful resuscitation of SCA.
What is already known on this topic
▶ Sudden cardiac arrest (SCA) is an infrequent event on the football field.
▶ Precompetition Medical Assessment is the recommended examination that may identify players at risk and thus prevent SCA.
▶ SCA on the football field is usually fatal if not managed expeditiously and efficiently using a defibrillator and effective cardiopulmonary resuscitation.
▶ An Emergency Action Plan is necessary to ensure a speedy response to a collapsed football player.
What this study adds
▶ The necessity to place a defibrillator on the sideline of the football field during a match.
▶ Hands-only cardiopulmonary resuscitation (CPR) is recommended as the initial on-field CPR technique for first responders, until defibrillation can be undertaken.
▶ Defibrillation, from potential hypertrophic cardiomyopathy, may require defibrillation sooner than the usual 3–5 min to be successful.
▶ A player who collapses without contact must be considered a cardiac arrest until proved otherwise.
▶ All members of a football team should be trained in at least hands-only CPR.
Acknowledgments
Grateful thanks are given to K Grimm and S Motaung for their assistance in preparation of the manuscript.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.