Article Text

Abstract
Objective To assess whether a platelet-rich plasma (PRP) injection leads to an enhanced tendon structure and neovascularisation, measured with ultrasonographic techniques, in chronic midportion Achilles tendinopathy.
Design Double-blind, randomised, placebo-controlled clinical trial.
Setting Sports medical department of The Hague medical centre.
Patients 54 patients with chronic midportion Achilles tendinopathy were included.
Interventions Patients were randomised to eccentric exercise therapy with either a PRP injection (PRP group) or a saline injection (placebo group).
Main outcome measurements Tendon structure was evaluated by ultrasonographic tissue characterisation, a novel technique which quantifies tendon structure into four echo-types: echo-types I+II represent organised tendon bundles, whereas echo-types III+IV represent a disorganised tendon structure. Colour Doppler ultrasonography was used to measure the degree of neovascularisation. Follow-up was at 6, 12 and 24 weeks.
Results A significant improvement in echo-types I+II was found after 24 weeks within both the PRP group (n=27) and the placebo group (n=27), but there was no significant between-group difference (95% CI −1.6 to 7.8, p=0.169). After 6 weeks, the neovascularisation score increased within the PRP group (p=0.001) and the placebo group (p=0.002), but there was no significant between-group difference in change in neovascularisation score at any point in time.
Conclusion Injecting PRP for the treatment of chronic midportion Achilles tendinopathy does not contribute to an increased tendon structure or alter the degree of neovascularisation, compared with placebo.
Funding Biomet Biologics LLC, Warsaw, Indiana.
Statistics from Altmetric.com
Introduction
Chronic midportion Achilles tendinopathy is a degenerative disorder that commonly affects middle-aged individuals.1 2 Conventional ultrasonography is frequently used to image tendon disorders.3 Ultrasonography is an operator-dependent technique, and transducer handling and machine settings can influence the image obtained. Consequently, the interobserver reliability of ultrasonographic assessment of tendon structure is not known, and changes in time may be difficult to compare.3 In veterinary medicine, a method for computerised ultrasonographic tissue characterisation (UTC; UTC imaging, Stein, The Netherlands) has been developed, in which ultrastructural organisation of tendon tissue could be matched with histomorphology of equine tendons as a reference test.4 Recently, this novel technique was found to be a reliable method, which was able to distinguish symptomatic from asymptomatic human Achilles tendons by quantifying the three-dimensional stability of the echopattern over contiguous images.3
Colour Doppler ultrasonography (CDU) is an established method to measure the vascularity within and around tendons. Hypervascularity is commonly seen in symptomatic Achilles tendons and is also called neovascularisation.5 The degree of neovascularisation can be measured with an excellent interobserver reliability using a five-point scale (modified Öhberg score).6 In previous studies, it was reported that neovascularisation was present in all symptomatic tendons, which decreased concurrently with a reduction in symptoms after conservative therapy.7 8 An increase in neovascularisation was observed within the first 3 weeks after applying sclerosing injections, which were successful when the neovascularisation later disappeared after this initial period.9 Although there is still discussion about the role of neovascularisation, these findings suggest a beneficial effect of increased neovascularisation within the very first period of treatment and an opposing effect when neovascularisation is still present in the longer term.
Injections with platelet-rich plasma (PRP), defined as an increased concentration of platelets with the ability to release several growth factors after degranulation, may improve tissue repair processes and therefore enhance tendon structure.10 A recent laboratory study indicated that PRP application may lead to accelerated remodelling of the damaged tendon collagen tissue with an increased vascularisation.11 These effects have never been measured in clinical studies on patients with tendinopathy.
Therefore, we evaluated whether a PRP injection in addition to an eccentric exercise programme leads to an improved tendon structure and an increased degree of neovascularisation, using ultrasonographic techniques.
Materials and methods
Patients
This study was part of a randomised, double-blind, placebo-controlled trial, which was performed at a sports medical outpatient department in The Netherlands and has been reported in the JAMA.12
Inclusion criteria were the presence of clinically diagnosed chronic midportion Achilles tendinopathy and an age of 18–70 years. Symptoms had to have been present for at least 2 months.
Exclusion criteria were clinical suspicion of other musculoskeletal (insertional disorders and tendon rupture) injuries, inflammatory internal disorders, use of fluoroquinolones, previous performance of a complete heavy load eccentric exercise programme1 or inability to perform it, or a previous injection with PRP.12
Procedures
The details of the RCT (which reported clinical outcome using the Victorian Institute of Sports Assessment-Achilles (VISA-A) questionnaire) have been reported elswhere.12 Patients could contact the researcher (RJdV), who arranged an appointment at the outpatient sports medicine department. One experienced sports medicine physician (JLT) examined the eligibility of the patients. Both ultrasonographic measures (UTC and CDU) were performed after inclusion. Prescription of the exercise therapy and the injection procedure were done after scanning.
For every included patient, one PRP injection and one saline injection were prepared. The PRP injection was prepared using the ‘Recover Platelet Separation Kit’ (type ‘Gravitational Platelet Separation’ III), in accordance with the system instructions.10 12 A total amount of 4 ml was prepared for infiltration.
All the patients received instructions for the rehabilitation programme. During the first 48 h after the injection, the patients could fully weight-bear and were advised to walk only short distances indoors. After 1 week, the exercise programme was started. The patients were instructed to start with stretching exercises for 1 week, and after 2 weeks, a 12-week heavy-load eccentric calf-muscle exercise programme was started, as described by Alfredson et al.1 The patients were instructed to perform 180 repetitions daily, despite the presence of pain. All patients were instructed to avoid weight-bearing sporting activities for the first 4 weeks of the study. After 4 weeks, a gradual return to sports activities was encouraged.13
Stratification was performed, based on the activity level of the patients using the Ankle Activity Score (AAS),14 and block randomisation was done to equalise the number of patients in both groups over time.12 Patients were randomised to the PRP group (PRP injection with eccentric exercises) or the placebo group (saline injection with eccentric exercises).
The treating sports-medicine physician (JLT), the researcher who collected the data and performed the analysis (RJdV) and the patients were all blinded to group allocation. The injection was given by a sports-medicine physician blinded to group allocation. A local anaesthetic was injected (2 ml of 0.5% marcain) in the skin and subcutaneous tissue. Hypoechoic areas within the thickened part of the tendon were identified in transverse and longitudinal plane using an ultrasonographic machine (MyLab30; Esaote Piemedical, Maastricht, The Netherlands). The fluid was injected using a 22G needle under ultrasonographic guidance via three puncture locations. Through each puncture location, five small depots were left at several sites in the degenerative areas of the tendon. The first injection was placed at the site of most degenerative areas, and the other two injections were positioned proximal and distal from the first injection. If there was no hypoechoic region or irregular fibre structure in the thickest part of the tendon, we chose to inject the substance to the most painful site medially or laterally.
Outcome measurements
Ultrasonographic tissue characterisation
The outcome measurements were determined with the ultrasonographic techniques and were evaluated by a single researcher (RJdV) at baseline and after 6, 12 and 24 weeks postinjection. The detailed working mechanisms of ultrasonographic tissue characterisation (UTC; UTC imaging) have been previously described in the literature.3 4 The patients were asked to lay prone on the examination table with the affected leg positioned in a holding device, which ensured a standardised dorsiflexion (15°) of the ankle. The UTC procedure and measurements were performed with a high-resolution 10 MHz linear-array transducer (Smartprobe 10L5, Terason 2000; Teratech, Burlington, MA, USA). The transducer was secured in a frame which was clamped in the holding device to prevent motion of the transducer. This transducer was moved automatically with a constant speed, using a driving mechanism, along and perpendicular to the Achilles tendon's long axis over a distance of 9.6 cm. This custom-designed tracking and data-collection device assisted the collection of digital transverse images at regular distances of 0.2 mm. These images were stored on a computer and subsequently used to reconstruct a three-dimensional data block. The processing of contiguous transverse images by means of custom-designed algorithms facilitated the discrimination of four echo-types: echo-types I and II are generated from a single ultrasound reflection that belong to typically one interface structure and therefore represent more or less organised tendon bundles. Echo-types III and IV are generated by multiple reflections that interfere as a consequence of multiple interfaces that represent smaller, disorganised and more amorphous or fibrillar structures that have been described in tendinotic tissue. The method has been extensively described and validated in equine tendons,4 and to a lesser extent it has also been tested in tendinopathy patients versus a control group.3 Furthermore, this information can be visualised tomographically in three planes of view: transverse, sagittal and coronal.
The thickest part of the tendon in the anterior–posterior direction was identified, and subsequently the border of the tendon was identified in the grey-scale image at the thickest part. This procedure was also executed twice at 1.5 cm proximal and distal from the thickest segment, resulting in five bordered slices within 3 cm. Contours were interpolated, and subsequently the volume within a 3 cm length of the tendon could be analysed. The proportions of the four echo-types within this volume were calculated. The distance from the thickest part to the calcaneal bone was calculated and used with the follow-up examination to ensure that the same volume of the tendon was evaluated each time.
One trained researcher (RJdV) performed all UTC scans and could establish the outcomes (combined scanning and analysis of the images) with an intraclass correlation coefficient for intraobserver reliability of 0.88 with a mean difference of 0.80% and SD of 3.7 (unpublished data). A second experienced researcher (HvS) determined whether the UTC scans could be included into the final analysis.
Colour Doppler ultrasonography
A colour Doppler ultrasonography (CDU) examination was performed with a linear high-frequency 12–15 MHz transducer (MyLab30; Esaote Piemedical). The Doppler gain was set at 79%, just below random noise. For CDU, the Doppler frequency was set at 6.6 MHz. Patients were examined by one trained researcher (RJdV), who participated in previous studies on determination of the neovascularisation score.6 15 Patients lay prone on the examination table with the ankle placed in a neutral position during these measurements. To avoid obliteration of the vessels, the pressure of the probe was kept to a minimum. The tendons were examined in longitudinal and transverse planes as described previously.6 The blood vessels observed with CDU were scored using the five-grade modified Öhberg score.6 15 This score was determined as 0 (no vessels visible), 1+ (one vessel, mostly anterior to the tendon), 2+ (one or two vessels throughout the tendon), 3+ (three vessels throughout the tendon) or 4+ (more than three vessels throughout the tendon).
Statistical analysis
The power analysis was based on the primary outcome measure of the trial.12 A total of 27 patients in each arm were required (80% power with two-sided testing at a 5% level of significance).
Analysis was done on the basis of intention to treat. The data remained blinded until the last patient was seen for follow-up and after the analysis, enabling a blinded statistical analysis. After that, the blinding code was broken. The Kolmogorov–Smirnov test was used to evaluate normality of distribution of the data. Parametric tests were used in case of normality and non-parametric tests in case of skewed distribution of the data. These tests were performed for within-group and between-group differences in ultrasonographic scores.
Statistics were performed using SPSS version 16.0.1 (SPSS Science, Chicago, Illinois), and significance was assumed when p values were less than 0.05.
The study protocol was approved by the regional Medical Ethics Committee and registered with ClinicalTrials.gov, number NCT00761423.
Role of the funding source
The sponsor of the study (Biomet Biologics LLC, Warsaw, Indiana) had no role in the study design, data collection, analysis, interpretation or writing of the article. All authors had full access to the data and made the final decision for publication.
Results
Patients
Patients were included from August 2008 to January 2009. In July 2009, the last patient had an appointment for follow-up. The flow diagram (figure 1) shows the progress of the study participants. During the study, there were no patients lost to follow-up. Eight UTC scans could not be used for final analysis, and five CDU examinations could not be performed. The reasons for these missing data are mentioned in figure 1.
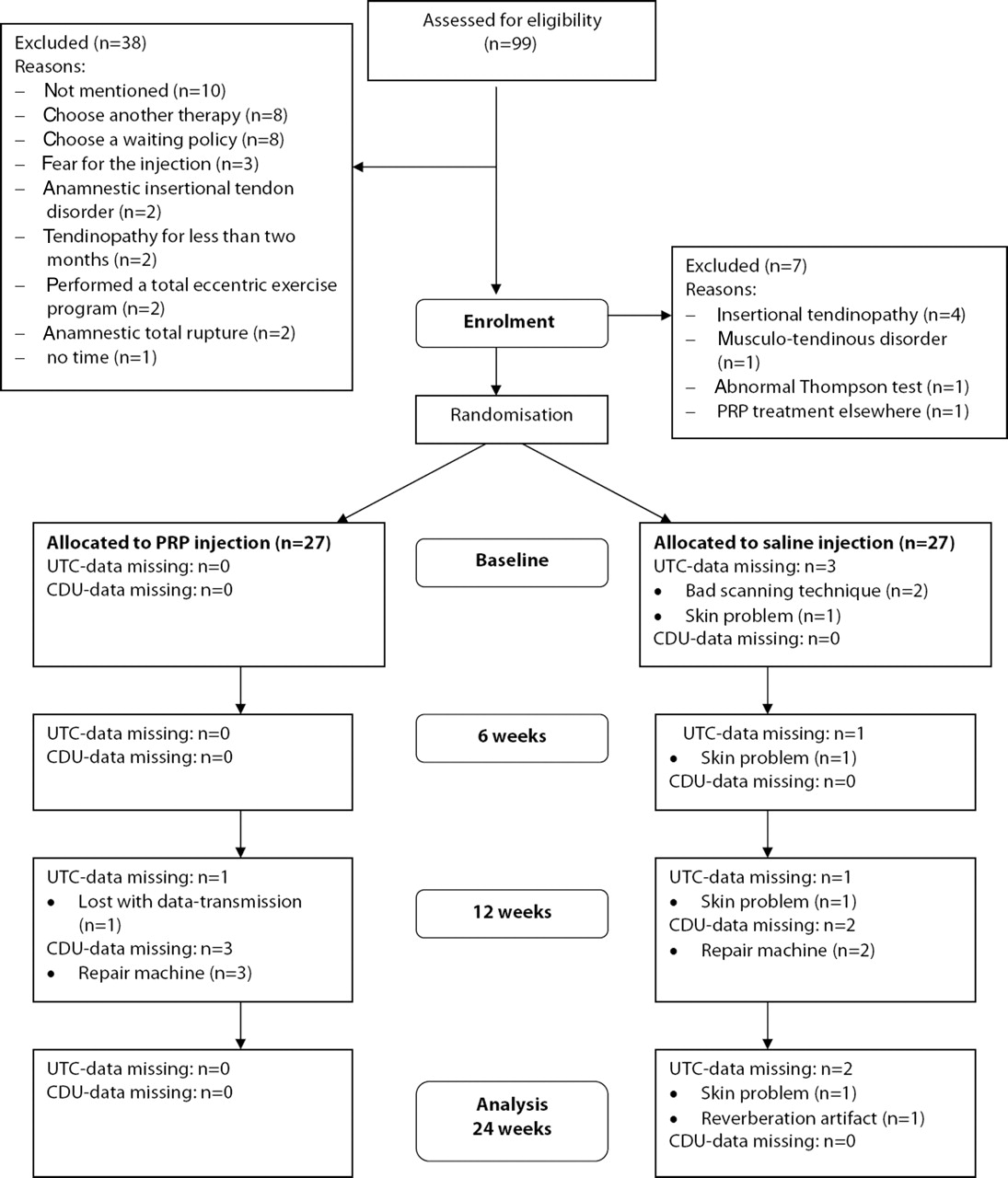
Progress of patients through the study. Eight ultrasonographic tissue characterisation (UTC) scans could not be used for final analysis, and five colour Doppler ultrasonography (CDU) examinations could not be performed. PRP, platelet-rich plasma.
At baseline, the patient characteristics and outcome variables did not differ significantly between the two treatment groups (table 1). All data were normally distributed, and so within-group changes were analysed with paired t tests and between-group differences evaluated with a simple t test.
Patient characteristics and outcome variables at baseline in platelet-rich plasma (PRP) group and placebo group
Mean proportions of UTC echo-types
Echo-types I+II increased significantly from baseline to 24 weeks within the PRP group (95% CI 6.2 to 12.7, p<0.001) and the placebo group (95% CI 8.9 to 16.1, p<0.001). Concurrently, the echo-types III+IV decreased significantly within the PRP group (95% CI −6.2 to −12.8, p<0.001) and the placebo group (95% CI −8.9 to −16.1, p<0.001). There was no significant difference in change in echo-types I+II between both treatment groups from baseline to 6 (95% CI −4.3 to 5.6, p=0.684), 12 (95% CI −2.1 to 10.6, p=0.232) and 24 weeks (95% CI −1.6 to 7.8, p=0.169). Figure 2 illustrates the mean differences in echo-types I+II during follow-up in the PRP group and in the placebo group.

Difference in echo-types I+II between the platelet-rich plasma (PRP) group and the placebo group. Error bars denote SDs. Within both treatment groups, a significant increase in echo-types I+II could be observed after 24 weeks. However, there were no significant between-group differences in change in echo-types I+II.
Within the PRP group, echo-type I improved significantly from baseline to 24 weeks (95% CI 5.9 to 11.5, p<0.001). Echo-type II remained stable from baseline to 24 weeks (95% CI −0.8 to 2.2, p=0.350). Echo-type III diminished significantly from baseline to 24 weeks (95% CI 3.3 to 7.0, p<0.001), and echo-type IV also decreased significantly from baseline to 24 weeks (95% CI 2.7 to 5.9, p<0.001).
Within the placebo group, echo-type I increased significantly from baseline to 24 weeks (95% CI 8.9 to 16.1, p<0.001). Echo-type II remained stable from baseline to 24 weeks (95% CI −0.01 to 3.3, p=0.056). Echo-type III decreased significantly from baseline to 24 weeks (95% CI 5.0 to 9.0, p<0.001) and echo-type IV also decreased significantly from the start to 24 weeks (95% CI 3.9 to 7.2, p<0.001).
There were no significant differences in the change in any echo-type at any point in time between both treatment groups. The changes in the proportion of echo-types I, II, III and IV over time in the PRP group and placebo group are shown in figure 3A,B.

(A) Progress of the four different echo-types within the platelet-rich plasma (PRP) group. Error bars denote SDs. Echo-type I increased significantly from baseline to 24 weeks, echo-type II remained stable, and echo-types III and IV decreased significantly. (B) Progress of the four different echo-types within the placebo group. Error bars denote SDs. Echo-type I increased significantly from baseline to 24 weeks, echo-type II remained stable, and echo-types III and IV decreased significantly. There were no significant differences in the change in echo-types compared with the PRP group at any point in time.
Mean neovascularisation score
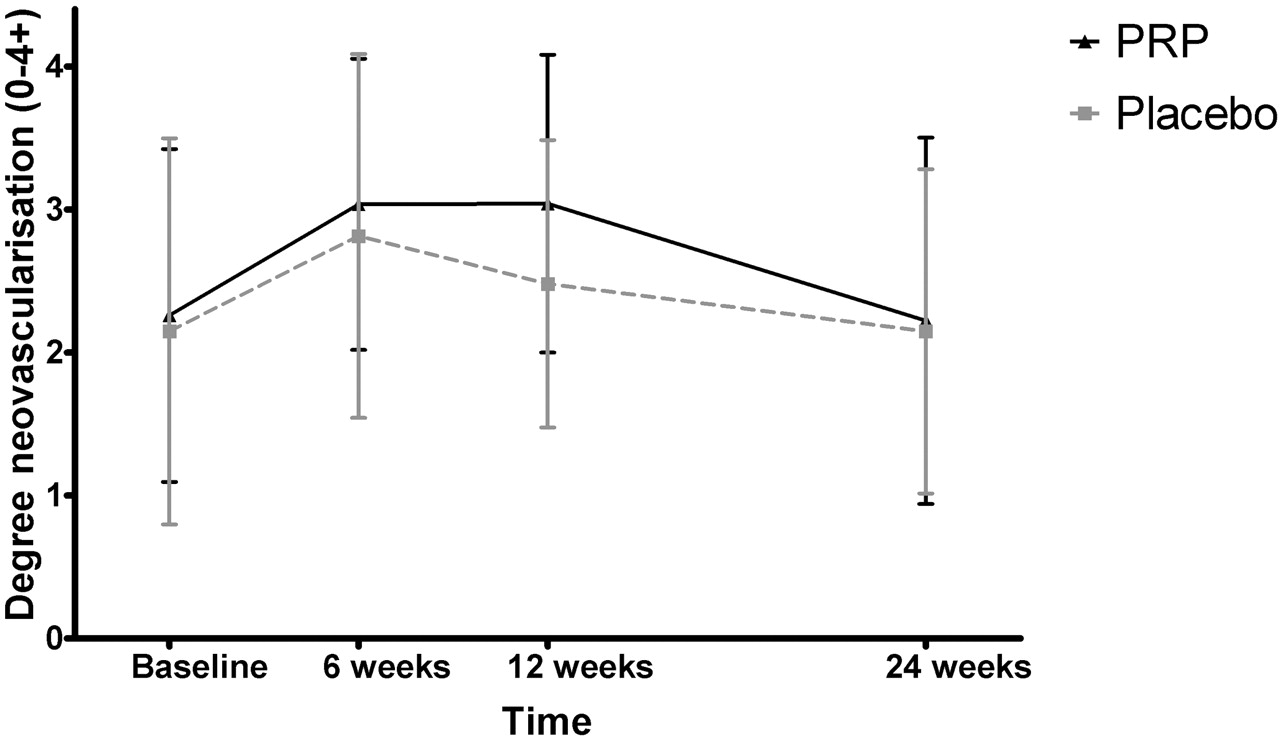
There was an increase in neovascularisation within 6 weeks in both groups (PRP group: p=0.001; placebo group: p=0.002), but these scores returned to pretreatment levels after 24 weeks (PRP group: p=0.89, placebo group: p=1.00). There were no significant differences in change in neovascularisation score from baseline to 6 (p=0.373), 12 (p=0.442) and 24 weeks (p=0.749) between both treatment groups. The mean degree of neovascularisation in both treatment groups is shown in figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in neovascularisation score in both treatment groups. Error bars denote SDs. During the first 6 weeks, the degree of neovascularisation increased within the platelet-rich plasma (PRP) group and the placebo group, but after 24 weeks the neovascularisation score returned to normal. The change in neovascularisation score from baseline also did not differ significantly at any point in time between the PRP group and the placebo group.
Discussion
This study shows that there is no difference in change in tendon structure within 24 weeks after injecting PRP in addition to eccentric exercises in the treatment of chronic midportion Achilles tendinopathy, compared with placebo. In the patients treated with PRP and placebo, there was an initial increase in the degree of neovascularisation, but the change in neovascularisation score was not significantly different between both treatment groups.
These findings are important and clinically relevant, as PRP is growing in popularity. Recent reviews supported its use for chronic tendon disorders,17 18 but good clinical evidence is lacking.19 20
Recent studies reported that PRP led to an enhanced tendon structure and increased neovascularisation in standardised surgically induced tendon lesions in horses.21 22 In the present study, there was an increase in organised tendon structure and initial increase in neovascularisation, but no differences were found between the groups treated with PRP and saline. The main reason may be that a traumatic model was used in the equine study, and the effects of PRP might be different in degenerative tendon tissue. It can also be possible that PRP was localised at the site of the lesion for a shorter time in our study because the fluid might have diffused rapidly out of the tendon due to the internal hydrostatic pressure. To reduce this phenomenon, the patients were asked to lay prone on the examination table for 10 min, which is also the suggested time of platelet degranulation and subsequent growth factor release.12 17 18 It is unknown how long the platelets remain locally at the site of the degenerative lesion. In our study, the platelets were not activated prior to injection, based on the assumption that platelets can be slowly activated as a consequence of the exposure to tendon collagen.17
The addition of an eccentric exercise programme may have resulted in dominating positive effects on tendon structure, thereby overshadowing an effect of PRP. Öhberg et al23 previously reported that eccentric training improves tendon structure on conventional ultrasonography, using a qualitative evaluation, at long-term follow-up in Achilles tendinosis. It may also be possible that eccentric training adversely affects any regenerative properties of PRP. The study design makes it impossible to rule out this possibility, although an experimental study on Achilles tendons of rats reported that mechanical load may be a prerequisite for the therapeutic effect of platelets.24
In a recent prospective observational study on the effects of eccentric exercises on tendon structure, there was no improvement in tendon structure after 24 weeks (in our manuscript titled ‘Ultrasonographic tissue characterisation imaging following eccentric calf muscle training in chronic Achilles tendinopathy,’ submitted to the Journal of Sport Rehabilitation). This is in contrast with the findings of Öhberg et al,23 and also in the current study we found that tendon structure improved within 24 weeks of follow-up. There are a few possible explanations for this discrepancy. It could be possible that introducing the needle within the tendon improved the tendon structure, since some studies showed positive clinical effects of needling.17 However, other mechanisms may be responsible. For instance, the populations between the studies may differ. In the present study, a high number of patients were involved in sports participation with a similar high ankle loading activity, quantified with the AAS. It is known that athletes benefit more from eccentric exercise therapy than do sedentary individuals.25 The reason for this finding is unknown, but it has been suggested that the compliance to the eccentric exercises may be of relevance in treatment outcome.13 The reported patient compliance to the eccentric exercises was found to be high in the present study.12
A limitation of the current study may be that the neovascularisation score is not validated.26 In a previous study, we found that this scoring system has an excellent interobserver reliability,6 but the test–retest reliability is not known, and so we cannot confirm whether this score could be used in a follow-up study. An in vivo study on equine tendons reported that the number of properly aligned blood vessels, determined in harvested tissue at postmortem, was correlated to the neovascularisation score with the preceding in vivo CDU examination.22 In the present study, we used a comparable machine and similar settings. Moreover, the measurements in the current study were performed under standardised conditions. The degree of ankle plantar flexion was standardised during the examination, and minimal probe pressure should be used to avoid obliteration of vessels.15 Another limitation could be that CDU is less sensitive than Power Doppler ultrasonography for determining the degree of neovascularisation.27 The available machine in our clinic contained merely a Colour Doppler function, but previous studies also showed increased amounts of neovascularisation using CDU.5 7,–,9
Future in vitro studies may be focused on the effects of PRP in the currently developing degenerative models.28 29 The influence of variables that may be of relevance could also be determined, such as the role of platelet activation prior to injection, the duration of collagen exposition to PRP, the concentrations of platelets and the concentrations of specific growth factors in the releasate.
The clinical implication of our study results is that there is no improvement in tendon structure and no effect on neovascularisation with the addition of PRP to eccentric exercises in chronic midportion Achilles tendinopathy, compared with a placebo injection. Particularly when taken together with our companion paper,12 these data argue against clinical use of this form of PRP in present clinical practice.
What is already known on this topic
Patients with Achilles tendinopathy have a disorganised tendon structure, measured with the standardised ultrasonographic tissue characterisation technique, and some degree of neovascularisation, measured with Doppler techniques. From laboratory studies, it is known that the use of platelet-rich plasma (PRP) can enhance the tendon structure and increase the neovascularisation. The effects of in vivo administration of PRP in patients with tendinopathy are not known.
What this study adds
PRP injections in addition to eccentric exercises for the treatment of chronic midportion Achilles tendinopathy do not contribute to an increased tendon structure, and there is no significant effect on neovascularisation, compared with a placebo injection.
Acknowledgments
The authors thank the company Biomet Biologics LLC (Warsaw, Indiana). The authors also thank the patients for their participation and the health professionals for referring. The authors would also like to thank some coworkers of this study, who were not compensated for their efforts. The authors are grateful for the logistic help of C van der Heijden, A de Vries and P Verschoor (Department of Sports Medicine, the Hague Medical Centre, The Netherlands). The authors are also thankful for the help and advice from the radiologists of the Hague Medical Centre Antoniushove, The Netherlands.
References
Footnotes
-
Funding Biomet Biologics LLC, Warsaw, Indiana.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was provided by the regional Medical Ethics Committee ZuidWest Holland.
-
Provenance and peer review Not commissioned; externally peer reviewed.