Article Text

Abstract
Background There are conflicting results in the literature regarding the association between radiographic knee osteoarthritis (OA) and symptoms and function in subjects with previous anterior cruciate ligament (ACL) reconstruction.
Aim To investigate the associations between radiographic tibiofemoral knee OA and knee pain, symptoms, function and knee-related quality of life (QOL) 10–15 years after ACL reconstruction.
Study design Cross-sectional study.
Material and methods 258 subjects were consecutively included at the time of ACL reconstruction and followed up prospectively. The authors included the Knee Injury and Osteoarthritis Outcome Score to evaluate knee pain, other symptoms (symptoms), activities of daily living and sport and recreation (Sport/Rec) and QOL. The subjects underwent standing radiographs 10–15 years after the ACL reconstruction. The radiographs were graded with the Kellgren and Lawrence (K&L) classification (grade 0–4).
Results 210 subjects (81%) consented to participate in the 10–15-year follow-up. Radiographic knee OA (K&L ≥grade 2) was detected in 71%, and 24% showed moderate or severe radiographic knee OA (K&L grades 3 and 4). No significant associations were detected between radiographic knee OA (K&L grade ≥2) and pain, function or QOL, respectively, but subjects with radiographic knee OA showed significantly increased symptoms. Severe radiographic knee OA (K&L grade 4) was significantly associated with more pain, symptoms, impaired Sport/Rec and reduced QOL.
Conclusion Subjects with radiographic knee OA showed significantly more symptoms than those without OA, and subjects with severe radiographic knee OA had significantly more pain, impaired function and reduced quality of life than those without radiographic knee OA 10–15 years after ACL reconstruction.
Statistics from Altmetric.com
Introduction
Knee osteoarthritis (OA) is considered an important disease in the western world because it may cause knee pain and disability.1 However, in the orthopaedic literature OA is usually defined solely based on radiographic abnormalities according to classification criteria defined in atlases.2,–,6 In the rheumatological literature, knee OA is defined by radiographic abnormalities in combination with pain or symptoms.7 8 Bedson and Croft9 reviewed population-based observational studies and reported that of subjects with knee pain, between 15% and 76% had radiographic knee OA.
The association between radiographic knee OA and knee pain, symptoms or function has not been consistent,10,–,12 with some studies reporting a weak association.13 The cut-off for defining radiographic knee OA usually includes abnormalities such as one osteophyte and possible joint space narrowing (Kellgren and Lawrence (K&L) grade 2), which is defined in the literature as the mildest grade of OA.2 However, studying the association between pain or function and one osteophyte compared with the association between pain or function and severe radiographic findings, such as definite joint space narrowing, multiple osteophytes, sclerosis and bone enlargements, may give different results.12 Neogi et al14 suggested that radiographic severity was strongly associated with knee pain. However, the association between severity of radiographic knee OA and knee pain, symptoms or function has not been thoroughly explored in subjects with previous anterior cruciate ligament (ACL) injury. Furthermore, increased age, female gender and high body mass index (BMI) have been shown to be significant risk factors for knee OA,15 and also significantly associated with knee symptoms and function.16 Few studies, however, have adjusted for significant risk factors in the analyses of the association between radiographic findings and pain, symptoms or function. This may lead to conflicting results. Ideally, studies should include large populations to enable adjustments for potential confounding factors.
Knee injuries, including ACL ruptures and meniscal injuries, have been suggested as important risk factors for the development of knee OA.17,–,19 Nevertheless, long-term follow-up studies of more than 10 years after ACL injuries are rare, and there are few studies examining the association between radiographic knee OA and knee pain, other symptoms, function or knee-related quality of life (QOL).20 Furthermore, to our knowledge, no studies with more than 10 years' follow-up after ACL reconstruction have examined the association between these variables and radiographic severity. Therefore, the aim of the present study was to investigate the association between radiographic tibiofemoral knee OA using the traditional cut-off for radiographic knee OA (K&L <2 vs ≥2) and knee pain, symptoms, function and QOL 10–15 years after ACL reconstruction. Furthermore, the aim was to examine the association between mild, moderate and severe radiographic knee OA and knee pain, symptoms, function and QOL, respectively.
Materials and methods
Two hundred and fifty-eight subjects who underwent ACL reconstruction were consecutively included in studies between 1990 and 1997. The subjects were included if they were between 14 and 50 years, and had isolated ACL injury or combined with meniscus injury and/or chondral lesion and/or medial collateral ligament (MCL) injury.21,–,23 The exclusion criteria were injuries to the contralateral knee and fractures in both legs the last year before inclusion. The subjects were operated with a bone–patellar–tendon–bone (BPTB) autograft or hamstrings tendon (HT) autograft previously described by Aune et al.21 The chondral lesions, the MCL injuries and the meniscal injuries suffered prior to or at the time of the ACL injury and the meniscal injuries suffered during the follow-up have retrospectively been extracted from surgeon files of all the subjects included at the 10–15-year follow-up. The MCL injuries were diagnosed by clinical assessment before the ACL reconstruction.
A supervised rehabilitation programme was included postoperatively as a three-phase programme lasting for 6–9 months.21 23 The subjects have been followed-up prospectively at 6 months, 1 year, 2 years21,–,23 and 10–15 years24 25 postoperatively with functional and clinical assessments, but for the aim of this study, only the 10–15-year follow-up evaluations were included.
The Regional Committee for Medical and Health Research Ethics in Norway has approved the study, and the participants signed an informed consent prior to participating at the 10-15 year follow-up.
Assessments
The Knee Injury and Osteoarthritis Outcome Score (KOOS) was used to assess knee pain, symptoms, function and QOL at the long-term follow-up.26 KOOS is a self-administered questionnaire comprising five subscales on pain, other symptoms (symptoms), activities of daily living (ADL), sport and recreation (Sport/Rec) and QOL. The KOOS subscales are organised into categories for each question which are transformed to a 0–100 scale. Zero indicates extreme knee problems, and 100 represents no knee problems. KOOS was developed for short- and long-term follow-up studies and has been validated on several types of injuries to the knee such as ACL and meniscal injuries, and post-traumatic OA.27 28 The Tegner activity scale was used to assess the activity level.29 To calculate BMI, we used the formula weight (kg)/height (m)2.
All the subjects participating at the 10–15-year follow-up went through a radiological assessment of the tibiofemoral joint. The procedure included standing radiographs with the knees flexed in approximately 20° and the feet 5° externally rotated by using a Plexiglas frame (SynaFlexer, Copenhagen, Denmark). The frame has been validated for measuring joint space width in patients with knee OA.30 Radiographs were taken bilaterally from a posteroanterior view.
One radiologist analysed the radiographs using the K&L classification system.2 31 The following definitions for each grade were used: grade 0, no changes; grade 1, doubtful narrowing of the joint space and possible osteophytic lipping; grade 2 (mild), definite osteophytes and possible narrowing of the joint space; grade 3 (moderate), multiple osteophytes, definite narrowing of the joint space and some sclerosis, and possible deformity of the bone ends; grade 4 (severe), large osteophytes, marked narrowing of the joint space, severe sclerosis and definite deformity of the bone ends.
The radiologist performed intrarater reliability test for the reading of the radiographs. The intrarater test was performed with at least a 4-week interval on 35 radiographs of both knees (n=70). The intrarater reliability result for the x-ray evaluation showed κ=0.77.
Statistical methods
We used linear regression to evaluate the association between radiographic tibiofemoral OA and the KOOS subscales pain, other symptoms, ADL, Sport/Rec and QOL with adjustment for age, gender and BMI (SPSS 16.0; SPSS, Chicago, Illinois). First, we evaluated the radiographic OA using a dichotomised radiographic variable: no OA (K&L 0/1=reference category) versus OA (K&L grade ≥2). Second, we evaluated radiographic OA severity in more detail by dichotomising each K&L grade still using K&L grade 0/1 as the reference category: K&L grade 2 versus 0/1, K&L grade 3 versus 0/1 and K&L grade 4 versus 0/1. Standardised β values, standard errors, 95% CI and p values were given for all regression analyses. We used the Mann–Whitney U test for group comparisons of non-parametric data (Tegner), and κ analysis to evaluate the reliability test of the x-ray scores. All tests were two-tailed, and we considered a p value of 0.05 or less as statistically significant.
Results
Two hundred and ten subjects participated in the study (81%): 90 females (43%) and 120 males (57%). The subjects' characteristics are presented in table 1. Of the 210 subjects, 29 (14%) were operated with HT graft, and 181 (86%) with BPTB graft. Isolated ACL injury was detected in 82 subjects (39%), and 128 subjects (61%) had additional meniscal injury, MCL injury or chondral lesion, or a combination of these (table 2). Eleven subjects had chondral lesions grade 3 (n=5) and grade 4 (n=6). Only 10 (8%) of the total of 121 (100%) subjects with meniscal injuries suffered the meniscal injury during the follow-up period. A total of 137 partial meniscal resections (91%) and 13 sutures (9%) were performed in the 210 subjects before the ACL reconstruction (22%), at the time of ACL reconstruction (53%) or during the follow-up period (25%). The activities performed at the time of injury comprised pivoting sports in 129 subjects (61%), mainly handball (n=37, 18%), soccer (n=70, 33%) or basketball (n=9, 4%), alpine skiing in 46 subjects (22%) and other activities or unknown activity in 23 subjects (11%) and 12 subjects (6%), respectively. No significant difference in median Tegner activity scale was shown between subjects with or without radiographic knee OA. Fourteen subjects (7%) suffered a graft rupture during the follow-up period, and four subjects (2%) suffered a partial graft rupture verified through arthroscopic procedures.
Subject characteristics at the 10–15-year follow-up (n=210)
Additional injuries at the 10–15-year follow-up (n=210)
Forty-five subjects (21%) were injured in the contralateral knee during the follow-up period, including isolated ACL injuries in 19 subjects (9%), ACL partial tear in one subject (0.5%), ACL in combination with meniscal injury in 11 subjects (5.5%) and isolated meniscal injury in 14 subjects (6%).
Seventy-one per cent of the subjects had radiographic signs of knee OA according to K&L≥grade 2 (table 3). The corresponding number for the contralateral knee was 25%. Moderate or severe knee OA (K&L ≥3) was detected in 24% for the target knee and 6% for the contralateral knee, respectively.
Frequency (%) of the Kellgren and Lawrence scores for involved and contralateral knee (n=210)
Table 4 shows unadjusted and adjusted results for the association between each KOOS subscale and radiographic knee OA (K&L <2 vs ≥2). No significant associations were detected, except for symptoms. The adjusted analysis indicated that subjects with radiographic knee OA at the level of K&L≥grade 2 had on average approximately six points lower KOOS other symptoms scores than those without radiographic knee OA.
Multiple regression analyses of the association between the Knee injury and Osteoarthritis Outcome subscales and Kellgren and Lawrence grade ≥2 versus grade <2 (n=206)
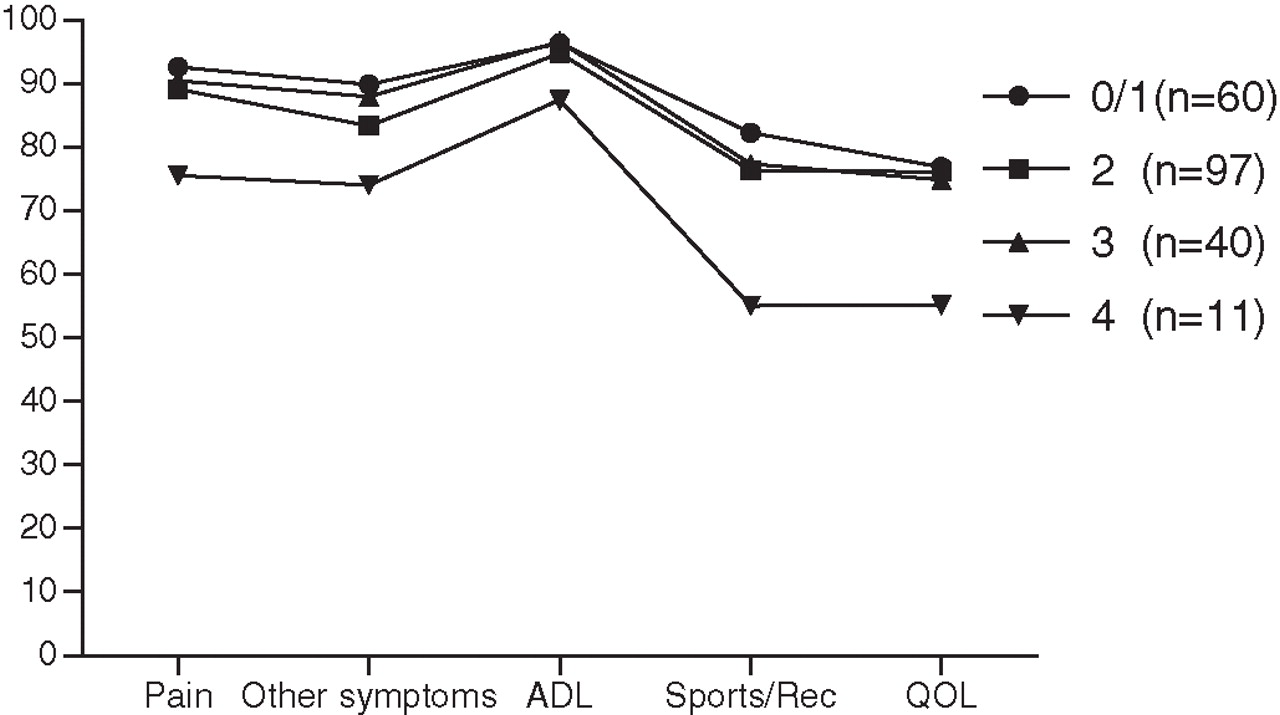
Figure 1 shows the mean values for the KOOS subscales for each K&L grade. No significant associations were detected between the KOOS subscales and mild or moderate radiographic knee OA adjusted for gender, age and BMI (table 5). Subjects with severe radiographic knee OA had significantly lower values for the KOOS subscales than those without OA.

{kind=link}
Mean values for the subscales of the Knee Injury and Osteoarthritis Outcome Score for each Kellgren and Lawrence grade (0–4). ADL, activities of daily living; QOL, knee-related quality of life; Sports/Rec, sports and recreation.
Multiple regression analysis of the association between the Knee Injury and Osteoarthritis Outcome Score subscales* and the Kellgren and Lawrence grades
Discussion
The results revealed that subjects with radiographic knee OA had significantly increased symptoms compared with those without radiographic OA. Furthermore, highly significant associations were detected between severe radiographic knee OA and pain, symptoms, ADL, Sport/Rec and QOL. It has been suggested that a change of 8–10 KOOS points constitutes a clinically relevant difference.27 However, 10 points have been arbitrarily set, and we suspect that it is difficult to state a common number for a clinical important difference for the different KOOS subscales. Therefore, the significantly increased symptoms for those with mild OA (six points in mean difference) may be of clinical importance compared with those without radiographic OA. The significantly increased pain, symptoms and reduced function seen in individuals with ACL reconstruction may be explained by the radiographic abnormalities.
No previous long-term studies including subjects with ACL reconstruction have evaluated the relationship between knee symptoms and function and radiographic knee OA using regression analysis. However, previous studies have evaluated the difference in mean values of the KOOS subscales between ACL injured subjects with and without knee OA.32,–,35 Lohmander et al32 reported significantly increased pain and symptoms in female soccer players with radiographic knee OA compared with those without radiographic knee OA 12 years after ACL injury in line with our results for symptoms. The mean values for the KOOS subscales were, however, generally lower than those reported in our study. For instance, those with radiographic knee OA had a mean value for pain of 70, compared with 84 in our study. Furthermore, their Sports/Rec and QOL values were 24 and 23 points lower than our results, showing that the female soccer players reported more complaints 12 years after ACL injury compared with our cohort of both males and females. Our results showed no significant differences between females and males for the KOOS subscales. The subjects in the study by Lohmander et al were younger than our cohort. They were only female soccer players, they were treated either with ACL reconstruction or non-operatively, and the study assessed both patellofemoral and tibiofemoral OA. Inclusion of both patellofemoral and tibiofemoral OA has been shown to be more frequently associated with knee pain and impaired function.12 In addition, a drop-out rate of 35% was reported in the study by Lohmander et al. These differences may explain the more impaired function found in their study. Meunier et al33 reported significantly increased pain and symptoms, and impaired function in ADL and Sport/Rec in subjects with radiographic OA compared with those without radiographic OA on average 15 years after the ACL injury. The mean KOOS subscales scores reported in their study were more similar to those in the present study except for the lower values for Sport/Rec (62 vs 75 points) and QOL (63 vs 74 points). Meunier et al included both subjects with ACL reconstruction and non-operative treatment, and subjects with grade 1 radiographic changes were included in the OA group. Our unadjusted results on the association between the KOOS subscales and radiographic OA were not very different from those of Meunier et al (pain: p=0.06; symptoms: p=0.01; Sport/Rec: p=0.05). Furthermore, Neuman et al34 studied ACL injured subjects without reconstruction 15 years after the injury, and they reported almost identical mean values for the KOOS subscales as found in the present study. These authors detected no significant differences between subjects with or without radiographic knee OA also in line with another follow-up study of male soccer players.35
The moderate inter-rater reliability results found for different radiological classification systems5 may be another explanation for the differences in results across studies with respect to the association between radiographic knee OA and pain, symptoms and function. The different classification systems emphasise to some extent either osteophytes or joint space narrowing, which may influence the cut-off for radiographic knee OA.2 3 4 Common for the above-mentioned studies and the present study was the long-term follow-up of ACL injured subjects (>10 years), but the studies included different radiological classification systems without attention towards radiographic severity. In the present study, we performed a regression analysis with adjustment for gender, age and BMI, as these factors have been shown to influence both the mean KOOS subscale values and the K&L scores.16 26 37 38 The adjustment for the potential confounding factors did influence the associations, particularly for pain and Sport/Rec.
Biological, psychological and social factors have all been shown to influence pain.39 For instance, psychological factors have been strongly associated with functional impairment and pain after adjustment for radiographic severity in patients with knee OA.40 Consequently, the lack of association between radiographic knee OA defined by the traditional cut-off and pain or function may be due to a true weak association. Our adjusted analyses showed that there were significant associations between severe radiographic knee OA and all KOOS subscales. Consequently, the follow-up studies on subjects with ACL reconstruction should emphasise the self-reported knee pain, symptoms, including effusion, locking, range of motion and stiffness and function, in addition to severity of radiographic knee OA, more than the prevalence of radiographic knee OA defined with a cut-off.
Our results revealed that those with a severe radiographic knee OA had significantly lower values on the KOOS subscales than those without OA. However, only 11 subjects had severe radiographic OA, and all these individuals had additional meniscal injury (n=6) or meniscal and chondral injury (n=5). The increased pain and symptoms, and the impaired function in these subjects may be due to the additional injuries and not the radiographic abnormalities. Meniscal injury has shown to be the most important risk factor for development of knee OA in subjects with ACL injury,5 but also for those without ACL injury.41 Therefore, it is difficult to explain the sources of the pain and symptoms in this population. The KOOS other symptoms subscale includes questions related to effusion, locking, range of motion and stiffness. These factors may be associated with the previous ACL reconstruction and the additional meniscal injuries.42 In addition, we detected no significant associations between moderate radiographic knee OA involving multiple osteophytes, definite narrowing of the joint space and some sclerosis, and the KOOS subscales. Brandt et al43 suggested that the synovium and subchondral bone are major sources of joint pain in patients with knee OA, but also that other joint structures, including the menisci and periarticular muscles, may contribute to the knee pain. Nevertheless, it may be reasonable that the increased pain and symptoms, and impaired function detected in our study were due to the severe radiographic changes, and not to the additional meniscal injuries suffered several years ago. However, whether the meniscal injuries or the radiographic abnormalities caused the increased pain and impaired function for those with severe radiographic OA cannot be stated on the basis of these data.
The present study has some limitations: a drop-out rate of 19% may have biased the results, but there were no significant differences in gender or age between the study participants and those who dropped out. No data on the patellofemoral joint was available for this study. There may be a risk of type 2 error in the analyses, and so there may be true differences between those with radiographic OA and those without detected with larger sample size.
This study revealed that only individuals with severe radiographic OA 10–15 years after ACL reconstruction had a significantly increased pain and reduced function compared with those without knee OA. Future research should perform risk-factor analyses to provide further evidence for treatment methods to reduce the development or delay the progression of radiographic knee OA, but also study treatment methods targeting reducing pain and symptoms and increasing function. Finally, future studies on subjects with ACL injury should include an assessment of radiographic severity, and the definition of knee OA should involve both radiographic abnormalities and pain or symptoms.
Conclusion
Subjects with radiographic knee OA had significantly increased symptoms compared with those without radiographic OA. Subjects with severe radiographic knee OA had also significantly more pain, impaired function and reduced quality of life compared with those without radiographic knee OA 10–15 years after ACL reconstruction.
What is already known on this topic
A high prevalence of radiographic knee osteoarthritis (OA) is reported for individuals with anterior cruciate ligament (ACL) reconstruction, but long-term self-reported knee function has been shown to be good. Conflicting evidence exists on the association between symptoms or function and radiographic knee OA.
What this study adds
This study provides analyses on the association between radiographic severity and knee symptoms and function. This study found that subjects with severe radiographic knee OA had increased symptoms and impaired function compared with those without radiographic knee OA more than 10 years after ACL reconstruction.
Acknowledgments
The authors gratefully acknowledge radiologist R Gunderson for grading the radiographs.
References
Footnotes
-
Competing interests None.
-
Funding This study was funded by the South-Eastern Regional Health Authority in Norway through the Osteoarthritis Research Group.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was provided by Regional Committees for Medical and Health Research Ethics in Norway.
-
Provenance and peer review Not commissioned; externally peer reviewed.