Article Text

Abstract
Background Patellofemoral pain syndrome (PFPS) is the most common overuse injury in runners. Recent research suggests that hip mechanics play a role in the development of this syndrome. Currently, there are no treatments that directly address the atypical mechanics associated with this injury.
Objective The purpose of this study was to determine whether gait retraining using real-time feedback improves hip mechanics and reduces pain in subjects with PFPS.
Methods Ten runners with PFPS participated in this study. Real-time kinematic feedback of hip adduction (HADD) during stance was provided to the subjects as they ran on a treadmill. Subjects completed a total of eight training sessions. Feedback was gradually removed over the last four sessions. Variables of interest included peak HADD, hip internal rotation (HIR), contralateral pelvic drop, as well as pain on a verbal analogue scale and the lower-extremity function index. We also assessed HADD, HIR and contralateral pelvic drop during a single leg squat. Comparisons of variables of interest were made between the initial, final and 1-month follow-up visit.
Results Following the gait retraining, there was a significant reduction in HADD and contralateral pelvic drop while running. Although not statistically significant, HIR decreased by 23% following gait retraining. The 18% reduction in HADD during a single leg squat was very close to significant. There were also significant improvements in pain and function. Subjects were able to maintain their improvements in running mechanics, pain and function at a 1-month follow-up. An unexpected benefit of the retraining was an 18% and 20% reduction in instantaneous and average vertical load rates, respectively.
Conclusions Gait retraining in individuals with PFPS resulted in a significant improvement of hip mechanics that was associated with a reduction in pain and improvements in function. These results suggest that interventions for PFPS should focus on addressing the underlying mechanics associated with this injury. The reduction in vertical load rates may be protective for the knee and reduce the risk for other running-related injuries.
Statistics from Altmetric.com
Introduction
Running is one of the most popular forms of exercise in the USA. Annually, 50–85% of runners will sustain an injury.1 2 Of these injures, patellofemoral pain syndrome (PFPS) is the most commonly reported.3 PFPS often becomes chronic, with up to 91% of individuals reporting continued knee pain 4–18 years after being initially diagnosed.4 In addition, recent research suggests that having a history of PFPS increases the risk of later developing patellofemoral osteoarthritis (OA).5
The aetiology of PFPS is multifactorial in nature. Most investigators agree that PFPS is related, in part, to faulty lower-extremity mechanics. In particular, there is growing scientific support for the relationship between hip mechanics and patellofemoral joint mechanics. In an early cadaveric study, Huberti et al reported that increasing the Q-angle (which would be associated with increased hip adduction (HADD)) resulted in greater contact pressure on the lateral aspect of the patella.6 In a more recent cadaveric study, Li et al demonstrated that increasing femoral internal rotation resulted in greater lateral patellar contact pressure.7 Over time, the repetitive exposure to these motions may damage the cartilage and lead to greater stress on the highly innervated subchondral bone.8 9
There is also emerging evidence that altered hip kinematics during dynamic activities are present in individuals with PFPS. For example, a recent study has found greater peak hip internal rotation (HIR) during running in individuals with PFPS.10 In addition, Willson et al reported that individuals with PFPS run, jump and squat with greater HADD compared with healthy controls.11 They also found greater contralateral pelvic drop across activities.11 Finally, a recent prospective study has found that runners who developed PFPS had greater HADD compared with their healthy counterparts.12
Several investigators have examined the effect of hip abductor and external rotation strengthening on PFPS.13 14 While they have reported improvements in hip strength and reductions in knee pain, most have lacked any follow-up beyond the completion of the treatment. However, in a study by Blønd et al, it was reported that 80% of individuals who had engaged in a strengthening programme continued to have pain 5 years later. In addition, 74% had to reduce their physical activity as a result of pain.15 This suggests that the underlying mechanics were not addressed directly.
There is increasing evidence that individuals can successfully alter their gait mechanics using real-time feedback.16,–,18 19 As an example, White et al studied a group of individuals with a unilateral hip replacement and associated reduced loading on their involved side.16 After 8 weeks of gait retraining using real-time force feedback from an instrumented treadmill, the subjects were able to significantly improve their loading symmetry. These results suggest that the retraining of motor patterns may be a promising approach to reducing PFPS.
The ultimate goal of gait retraining is to promote learning of new gait patterns. Indications of learning include the retention of new motor skills, as well as their transfer to another unpractised activity.20 Addressing the issue of retention, both Crowell et al (2009) and Barrios et al (2008) reported that gait changes induced using real-time biomechanical feedback were retained at a 1-month follow-up.18 19 However, neither of these studies examined the transfer of the new motor skills to other activities.
In summary, altered hip mechanics have been shown to be related to PFPS. Studies have provided support that individuals can learn to alter their gait mechanics using real-time feedback. However, these techniques have not been applied to runners with PFPS. Therefore, the purpose of this study was to determine the effect of gait retraining using real-time kinematic feedback on hip mechanics for individuals with PFPS. We hypothesised that peak HADD, HIR and contralateral pelvic drop would be reduced following the retraining. We also expected an associated reduction in pain and improvement in function following retraining. We expected all changes to persist at the 1-month follow-up. Finally, we hypothesised that the improvements in hip mechanics seen in running would also transfer to a single leg squat. This activity was chosen because the movement is similar to that which occurs during the first half of stance in running.
Methods
Based on the variability of preliminary data collected in our lab and an a priori power analysis with α=0.05 and β=0.20, we trained 10 subjects in the current study. Male and female recreational runners, between the ages of 18 and 45 years old, were solicited through advertisements and local races. They had to report anterior knee pain during running that had persisted for at least 2 months and were unrelated to overt trauma. Participants had to be running at least three times per week, for a minimum total of 6 miles per week. They also had to currently be free from any cardiovascular condition, any injury other than knee pain and any impairment that could influence their gait. Lastly, subjects could not be receiving any other concurrent treatment for the duration of the study. Prior to inclusion, all subjects provided informed consent according to the institutional review board.
Subjects were evaluated by a licensed physical therapist to determine if they had PFPS. PFPS was operationally defined as pain that was located around or beneath the patella that was rated at least 4 out of 10 on a visual analogue scale during running. In addition, pain had to be reproduced with retro-patellar palpation or patellar compression.
Each potential subject's running mechanics were then assessed to determine if they qualified for the study. First, a video screening during treadmill running was conducted. Subjects who visually appeared to exhibit excessive HADD, indicated by an observable pelvic drop and knees that were nearly touching each other in midsupport, were invited for an instrumented gait analysis. Anatomical markers were placed over the most superior aspect of the iliac crests, the most prominent point of the greater trochanters, the distal aspect of the femoral condyles, the most proximal points of the tibial plateaus, the malleoli, the first and fifth metatarsal heads, and the distal aspect of the shoe. Tracking markers were placed on the bilateral anterior superior iliac spines, L5–S1 and on top of the second metatarsal head. In addition, three markers were placed on the rearfoot of the shoe. Lastly, a rigid clusters of four tracking markers were placed on the distal, posterolateral thigh and distal shank. The positions of the anatomical markers were recorded using a marker placement device.21 These measurements were then used to place the anatomical markers for each subsequent data collection. Use of this device significantly improves the day-to-day reliability of kinematic data, resulting in intraclass correlation values of 0.9 or greater for the hip variables of interest.21 Following the standing calibration trial, a hip motion trial was performed to establish the hip joint centre.22 The anatomical markers were then removed, leaving only the tracking markers for the subsequent collections.
The baseline dynamic motion trials were then collected. Data were first collected as the subject performed five single leg squats to approximately 60°. Then, following a 3 min warm-up on an instrumented treadmill (AMTI, Watertown, Massachusetts), subjects ran for 2 min at 3.35 m/s and 10 trials were recorded. The three-dimensional trajectories were captured at 200 Hz with an eight camera, Vicon motion analysis system (Vicon, Oxford). Force data were collected at 1000 Hz for the primary purpose of identifying stance. A 30 min run then followed to determined baseline pain levels. Subjects reported their pain every 5 min on the verbal analogue scale. If their pain exceeded 7 out of 10 during this run, the test was stopped and the run time recorded.
The data were then processed using Visual 3D (Visual 3D Germantown, Maryland). Joint kinematics were calculated for each stance phase during treadmill running using an X-Y-Z Cardan angle rotation sequence. The variables of interest included peak HADD, HIR and contralateral pelvic drop. Peak values were extracted from 10 individual curves and averaged across subjects. These curves were then time-normalised to create ensemble curves for each variable. Subjects whose HADD during running was excessive (>1 SD above the mean of a database of healthy recreational runners) were invited to participate in the retraining. Joint kinematics for the single leg squat were analysed between 0° and 45° of knee flexion. The single leg squat data were then processed in the same manner as the running data.
The baseline Lower Extremity Functional Index (LEFI) was then completed. This scale involves rating pain during a variety of activities of daily living including squatting, walking and running and has been found to be valid and reliable for patients with PFPS.23
Gait retraining sessions
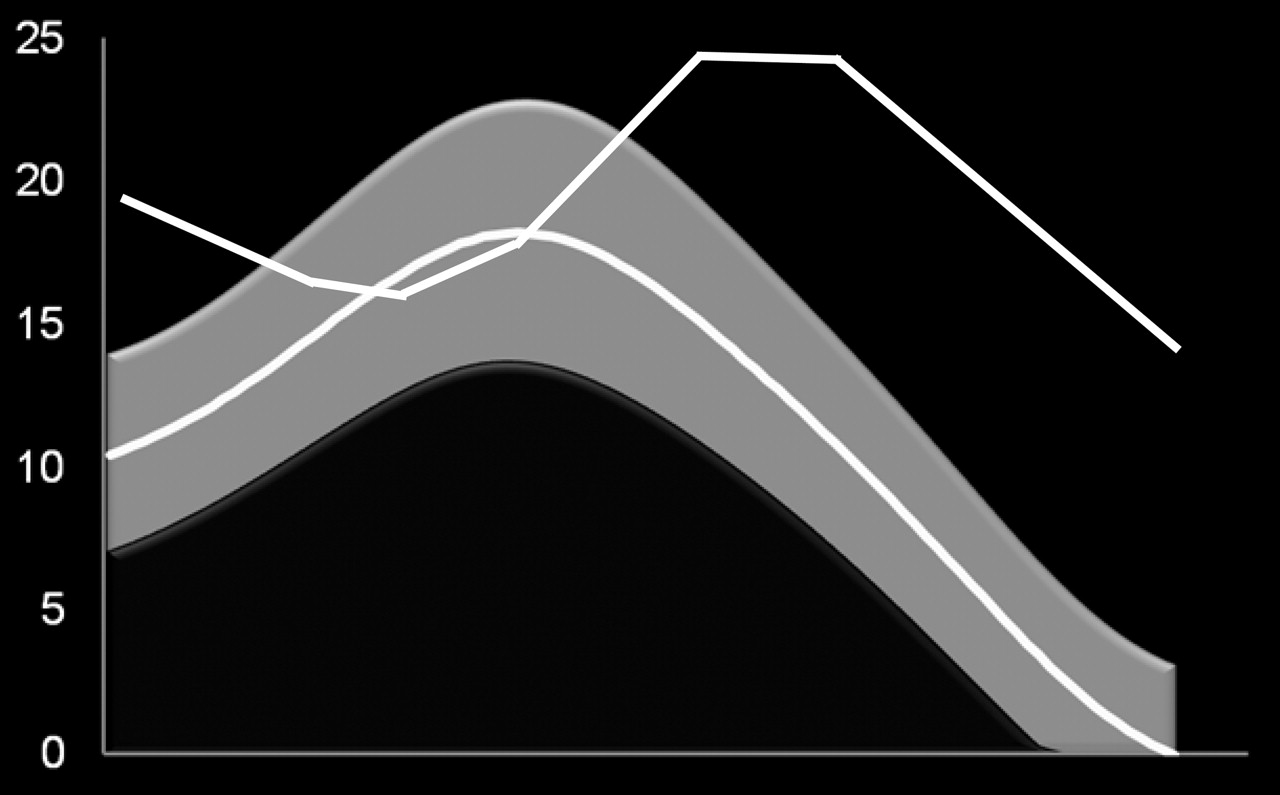
Subjects then began the retraining sessions. In the presence of bilateral knee pain, the leg with the greatest HADD was the focus of the gait retraining. At the beginning of each visit, markers were placed on the subject as previously described using the marker placement device. During the first visit, subjects were oriented to the real-time system. Their HADD angle was provided in real time on the monitor placed in front of them using Visual 3D Professional (Visual 3D, Germantown, Maryland). After some practice with observing the changes in their hip angle on the monitor as they altered their hip alignment, they began the feedback training. As they ran, the stance phase of their HADD graph was provided in real time on the monitor placed in front of them. They were instructed to keep their hip angle within the shaded region representing ±1 SD of normal HADD (figure 1). They were directed to contract their gluteal muscles and attempt to run with their knee pointing straight ahead, while maintaining a level pelvis.

Screen images seen by subjects undergoing real-time gait retraining. The grey region represents the mean (±1 SD) of a previously collected normal group. The subject was instructed to lower their curve to match the shaded region.
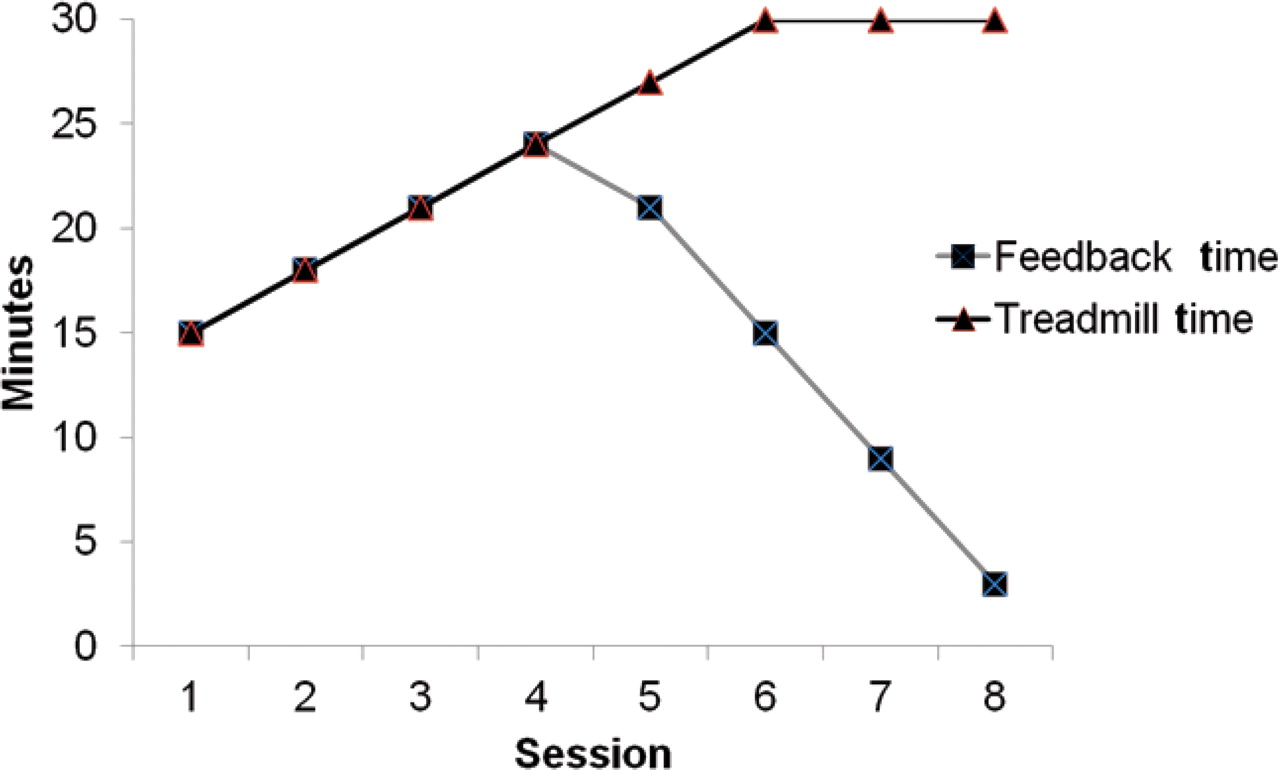
A faded feedback design was used in order to facilitate acquisition and internalisation of the new gait pattern, thereby improving its persistence.24 Run time was progressively increased from 15 to 30 min over the eight sessions (four visits/week for 2 weeks) (figure 2). Visual feedback was provided continually for the first four sessions. Feedback was then gradually removed over the last four sessions in an equal distribution between the beginning, middle and end of the retraining session. Subjects were instructed not to run outside the training sessions.

Gait retraining schedule. Runtime is gradually increased from 10 min to 30 min. During the first four sessions, the subject receives continuous feedback. Over the last four sessions, feedback is gradually removed.
Following the eight training sessions, another instrumented gait assessment was conducted. Markers were placed using marker positions previously recorded with the marker placement device. Pain during a 30 min run was again recorded. The LEFI was also administered. Subjects then were encouraged to gradually increase their running over the next month to their desired mileage. Subjects returned for a 1-month follow-up assessment of gait, 30 min run pain and LEFI, as described previously.
A repeated-measures analysis of variance was used to compare hip mechanics, pain and function at baseline, post- training and following the 1-month follow-up. Significant results were explored using post-hoc, two-tailed, pairwise comparisons (α <0.05). All statistical testing were performed using SPSS (SPSS, Chicago, Illinois). While hip kinematics were the focus of this investigation, ground reaction forces were collected concurrently as subjects ran on the instrumented treadmill. Impact loading variables have been shown to be related to other running-related injuries such as tibial stress fractures, plantar fasciitis and knee OA.25,–,27 Therefore, in a post-hoc analysis, changes in vertical impact peak (VIP) and average (VALR) and instantaneous (VILR) load rates were assessed as described in Milner et al25 Effect sizes and percentage differences between baseline and post-training were computed for these variables.
Results
One hundred and seventy subjects were initially evaluated to determine the presence of PFPS. Of these, 85 underwent the video screening. Of the 85, 19 underwent the instrumented gait analysis, and 11 qualified. Of these, 10 agreed to participate. All 10 subjects who qualified were female. The subjects' demographic information is presented in table 1. These subjects had experienced PFPS for an average of 75 months (3–264 months). All data were normally distributed as indicated by the Shapiro–Wilk test.
Mean demographic data for the 10 subjects who participated in the study
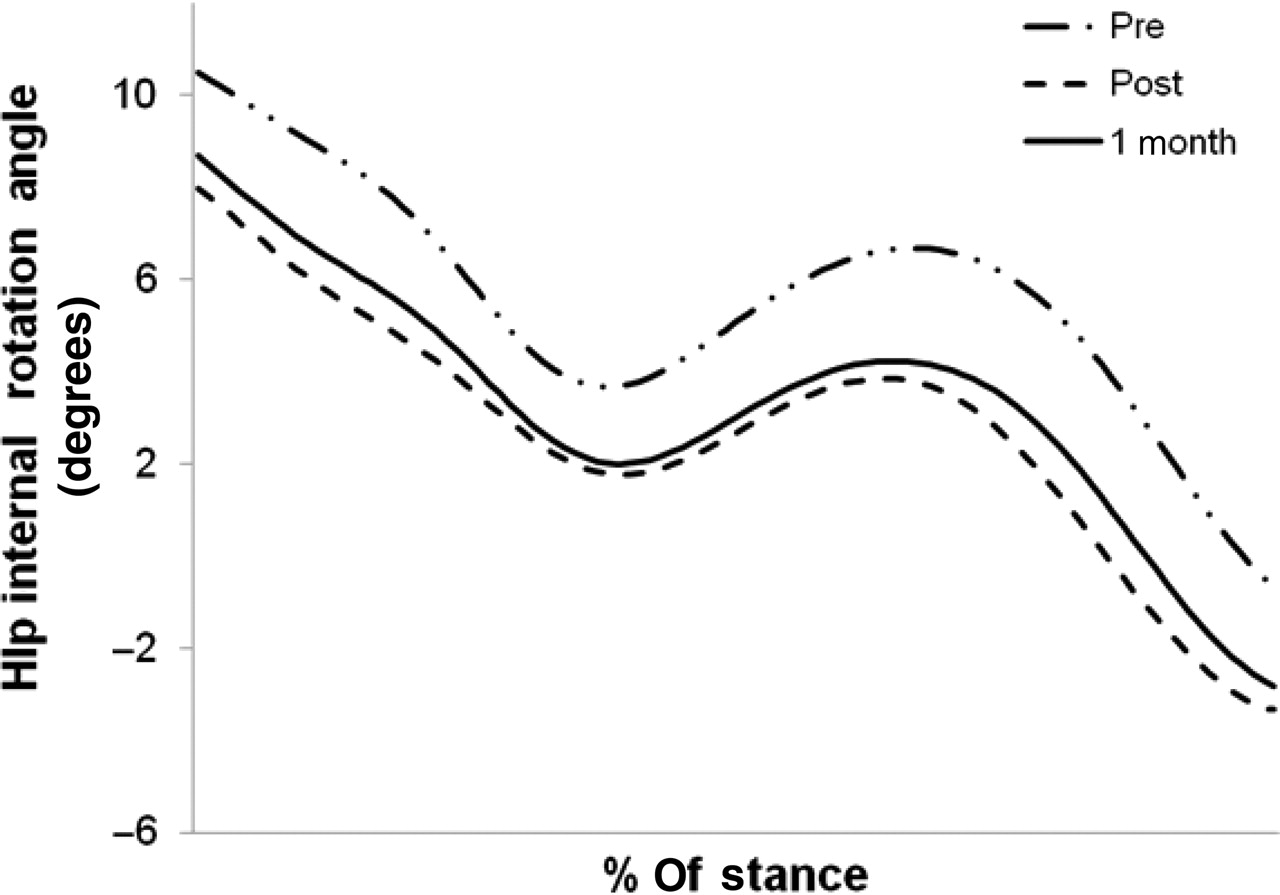
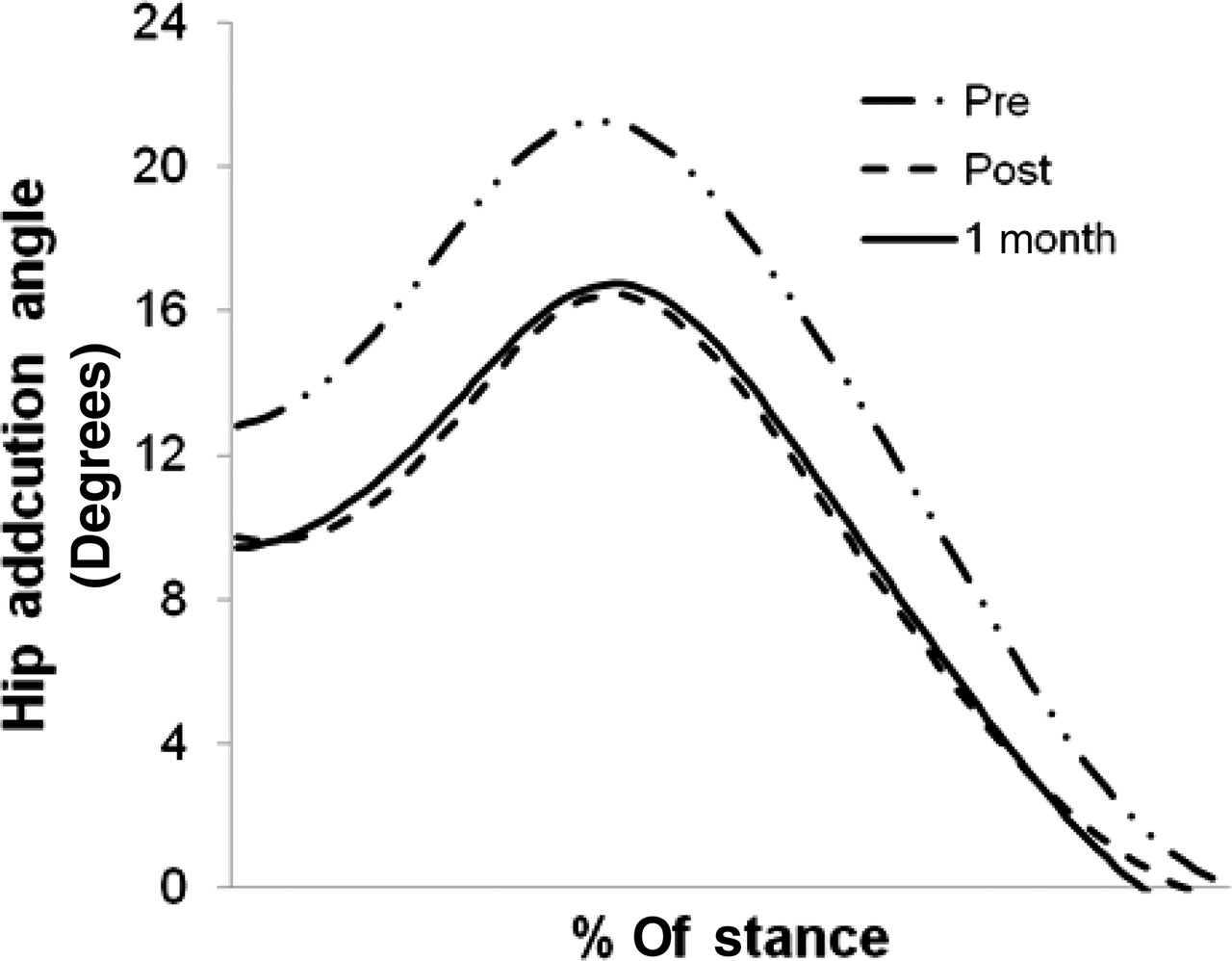
During running, there was a reduction in peak HADD, as well as an overall reduction throughout stance, following the retraining (table 2, figure 3). HIR was also reduced throughout stance. Although not a significant reduction, peak HIR was reduced by 2° and associated with a medium effect size (0.50). A significant reduction in contralateral pelvic drop was also found (figure 4). The reductions in both HADD and contralateral pelvic drop persisted at the 1-month follow-up (figures 3, 4). This was not true for HIR, which was increased slightly (0.8°) at the 1-month follow-up (figure 5).

Mean pattern of hip adduction during running at baseline (pre), following gait retraining (post) and at the 1-month follow-up. Hip adduction is positive.

Mean contralateral hip drop during running at baseline (pre), following gait retraining (post) and at the 1-month follow-up. Contralateral hip drop is negative.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean pattern hip internal rotation during running at baseline (pre), following gait retraining (post) and at the 1-month follow-up. Hip internal rotation is positive.
Hip kinematic variables during running*
In the single leg squat, peak HADD was reduced by 3° (p=0.055) and was associated with a moderate effect size (0.44) (table 3). However, there was no overall change in HIR and pelvic drop during the squat.
Hip kinematic variables during squatting*
Pain was reduced by 86% at the end of gait retraining and the LEFI improved by 11 points (table 4). These findings persisted at the 1-month follow-up. In addition, all subjects reported running at least at their baseline training volume by the 1-month follow-up. Lastly, all subject were running pain-free at the 1-month follow-up.
Comparison of pain and Lower Extremity Functional Index*
All impact-loading variables were reduced and associated with moderate to large effect sizes (table 5). VALR and VILR were reduced by 18 and 20% respectively.
Comparison of vertical impact loading variables during running
Discussion
The purpose of this paper was to determine whether gait retraining, using real-time kinematic feedback, improves hip mechanics, pain and function in runners with PFPS. In addition, we were interested in whether learning had occurred by assessing the persistence of these changes and their transfer to another activity. We found significant reductions in HADD, contralateral pelvic drop, pain and the LEFI after completion of the treatment. These changes were maintained at the 1-month follow-up and partially transferred to the single leg squat.
Subjects reduced their HADD during running by 5.0° or 23% following gait retraining (figure 3). According to Huberti, this reduction should decrease compression on the lateral aspect of the patella.6 These compressive loads have been reported to overload the subchondral bone and result in pain.9 28 29 It is therefore very plausible that the large reduction in pain seen in this study was related to the altered loading of the patellofemoral joint as a result of reduced HADD.
While not provided as feedback, HIR and pelvic drop were also reduced following the retraining. The 23% reduction in HIR was likely due to its coupled motion with HADD. As with HADD, a reduction in HIR has been shown to increase the load on the lateral patellar facet.7 The reduction in HIR was less consistent across subjects and thus was not statistically significant. However, it was associated with a moderate effect size (0.50) and may have contributed to the reduction in pain experienced by some of these subjects. The significant reduction observed in contralateral pelvic drop may lead to a reduction in tension on the iliotibial band on the stance leg. This, in turn, may reduce the tension in its attachment to the lateral patella, thereby allowing the patella to track more normally.30 31 Reductions in these combined motions likely contributed to the reduction in pain noted.
Results of this study suggest that learning had occurred. Reductions in HADD and pelvic drop during running were maintained at the 1-month follow-up. These results are very significant, as they suggest that the underlying mechanics associated with PFPS have been changed, reducing the risk for recurrence. However, longer-term studies are needed to determine whether these changes persist beyond a 1-month period. Another indicator of learning is the transfer of the new mechanics to another, unpractised skill.36 Based on our results, subjects did reduce their HADD by 2.1° (or 18%) during the single leg squat. These changes were seen in the absence of any instruction or feedback during this activity. There was, however, no reduction in either HIR or contralateral pelvic drop. Therefore, the transfer of the new hip mechanics to the single leg squat was greatest for the variable that was provided as feedback for running.
Most importantly, gait retraining resulted in a significant reduction in pain, as well as improvement in function. On average, a 86% reduction in pain was seen. This is remarkable given the chronic nature of the pain (average 75 months, range 3–264 months) these subjects experienced. This pain reduction was greater than most previously published reports, which ranged between 33% and 72%.13 14 32 33 Additionally, the 2-week training period was shorter than other interventions. The subjects' improvement in the LEFI score surpassed the nine point change that has been deemed clinically significant.23 This would suggest that improvements in the mechanics of running carried over to improvements in other activities of daily living.
The improvements in pain and function were also maintained. At the 1-month follow-up, all subjects reported 0/10 pain during a 30 min run, or a 100% reduction from baseline. By comparison, two recent review articles suggest that the long-term success of many conservative interventions is mixed.32 34 Blønd et al reported that at a 5-year follow-up after a strengthening programme, subjects were still limiting their physical activity (including running) because of chronic pain.15 Retraining studies with significantly longer follow-up periods are needed to determine if this novel intervention is more successful than standard treatments for PFPS.
An unexpected benefit of the retraining was the reduction in the impact loading that has been associated with other types of injuries. Milner et al has shown an association of increased VIPs and vertical load rates with tibial stress fractures associated with running.25 In a more recent study, Pohl et al reported a similar association of impact peaks and loading rates with running-related plantar fasciitis.26 In terms of knee pathology, Mündermann et al reported excessive lower-extremity joint axial load rates during walking in individuals with knee OA.27 While the impact loading, on average, was not excessive in the current study, there were individuals with excessive impact peaks and/or loading rates. The association between these impact loads and PFPS deserves further study. However, at a minimum, reducing impacts in these individuals may be protective from the development of other lower-extremity injuries.
Although the study was open to both males and females, it is interesting to note that only females qualified for the study following the screening. This suggests that females with PFPS have a greater tendency to exhibit excessive HADD and that males with PFPS may present with a different associated movement pattern. Indeed, Dierks et al (2008) recently found a subgroup of males with PFPS who exhibited greater hip abduction than controls.35 Therefore, further study of gender differences in the mechanics of individuals with PFPS is warranted.
This study is not without limitations. First, the intervention required motion analysis equipment and, thus, cannot be readily generalised to most clinics. Future studies will consider possible ways in which gait retraining could be performed in the clinic. Second, we are able to only infer possible changes at the patellofemoral joint from the observed changes at the hip. Imaging studies of three-dimensional patellofemoral joint mechanics during running are needed to provide this direct information. Third, while this initial study suggests a beneficial effect of gait retraining, a larger-scale, randomised control trial with a longer follow-up is needed to further substantiate these findings.
Conclusions
Gait retraining in subjects with PFPS resulted in significant reductions in pain and improvements in function. This suggests that addressing the underlying mechanics associated with this injury will reduce pain. These changes persisted at the 1-month follow-up and transferred over to a different, unpractised skill, suggesting that learning did occur. Finally, improving hip mechanics through gait retraining may have an added benefit of reducing impact loading.
What is already known on this topic
▶ Excessive hip adduction and internal rotation play a role in the development of patellofemoral pain syndrome (PFPS) in female runners.
What this study adds
▶ We found that real-time gait retraining in subjects with PFPS resulted in improved hip mechanics, a significant reduction in pain and improvement in function. Gait retraining for individuals who exhibit poor running mechanics should be considered when designing an intervention.
References
Footnotes
-
Funding This work has been supported by a scholarship from the Foundation for Physical Therapy, Inc. Additionally, this study was funded by the American College of Sports Medicine Student Research Grant as well as by NIH 1 S10 RR022396 and DOD W911NF-05-1-0097.
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the University of Delaware.
-
Provenance and peer review Not commissioned; not externally peer reviewed.