Article Text

Abstract
Protection of the athletes' health is a clearly articulated objective of the International Olympic Committee. Longitudinal surveillance of injuries and illnesses can provide valuable data that may identify high-risk sports and disciplines. This is a foundation for introducing tailored preventive measures. During the XXIX Summer and XXI Winter Games, comprehensive injury and illness recording through the medical staff of the participating National Olympic Committees and the sports medicine clinics revealed that between 7% and 11% of all athletes incurred an injury or suffered from at least one occurrence of illness during the Games. The incidence of injuries and illnesses varied substantially between sports. In the future, risk factor and injury mechanism analyses in high-risk Olympic sports are essential to better direct injury-prevention strategies. Concomitantly, periodic health evaluations of athletes will be instrumental to optimise health protection.
Statistics from Altmetric.com
Introduction
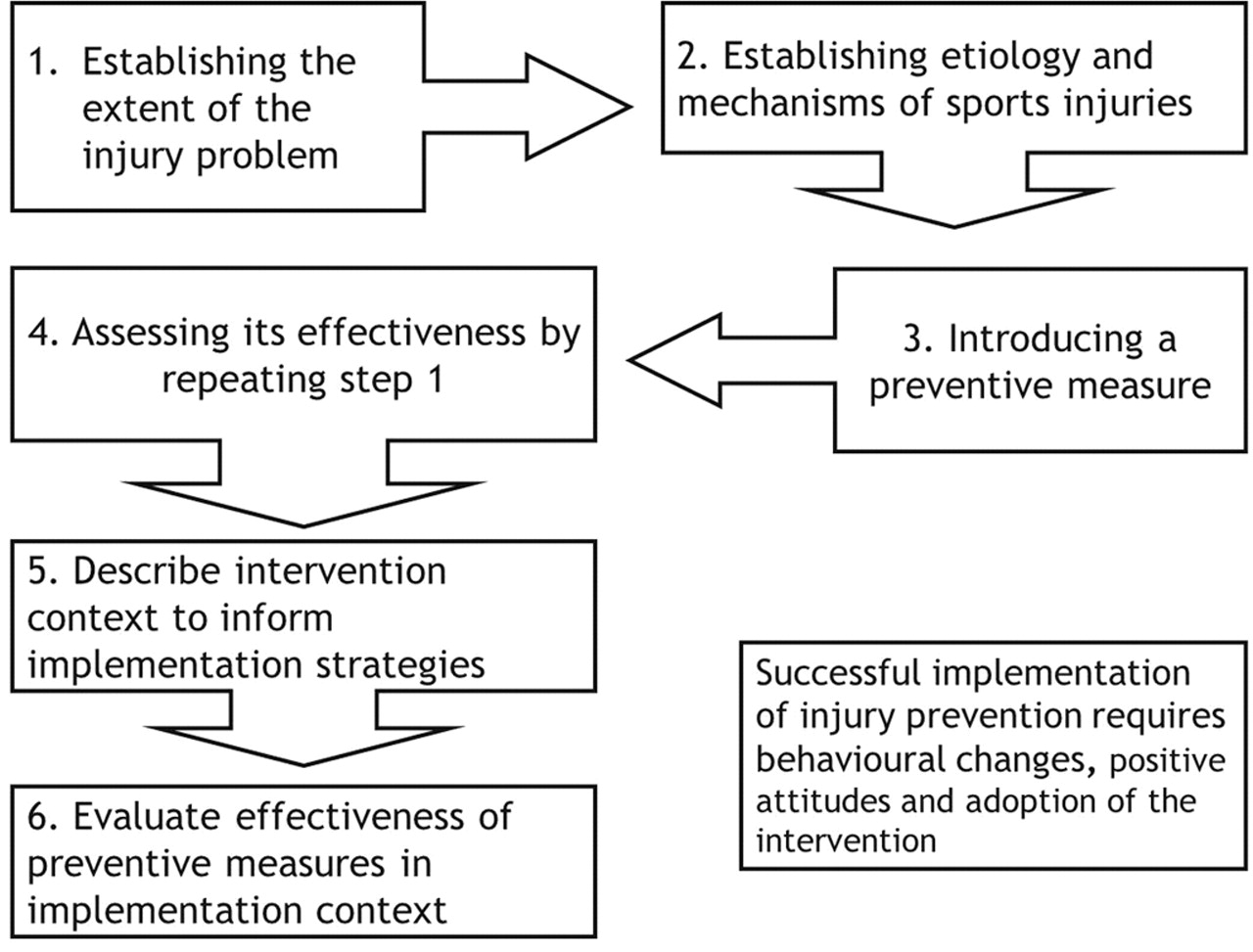
With almost 11 000 expected athletes from more than 200 countries, the XXX London 2012 Olympic Games will be one of the largest sports events ever. More than 2500 athletes participated in the XXI Winter Olympic Games held in Vancouver in 2010. The protection of an athlete's health is an important task for the International Olympic Committee (IOC).1 Systematic injury and illness surveillance monitoring over long periods of time, and the identification of high-risk sports, including the most common and severe injuries and illnesses, is a starting place from which to address injury-prevention occurrence.2 3 Following the six-stage Translating Research into Injury Prevention Practice (TRIPP) model of Finch,4 analysing the extent of a problem such as high injury and/or illness risk in a specific population, is the first step in the development of effective prevention strategies (figure 1).

{kind=link}
TRIPP model: framework for research leading to sports injury prevention.4
The IOC injury and illness surveillance system, developed in cooperation with the International Sports Federations (IFs) and National Olympic Committees (NOCs), was successfully implemented in the 2008 Beijing (injury surveillance only)2 and in the 2010 Vancouver Olympics (injury and illness surveillance).3 It will be further developed and optimised in the 2012 London and 2014 Sochi Olympic Games.5 Major sport events, such as the Olympic Games, constitute an ideal environment for instituting such surveillance. The study population is a relatively homogenous group in terms of skill level, and the study period is defined by the event itself, which is usually characterised by a high standard of environmental factors (eg, safety of venues, optimal preparation of training and competition facilities).6 7 As early as 1998, the Fédération Internationale de Football Association (FIFA) started to survey all injuries incurring during their competitions,6 8,–,11 and other major sports federations followed FIFA's Medical Assessment and Research Centre (F-MARC) lead.12,–,16 Based on these experiences, a group of experts, convened by the IOC, developed an injury surveillance for multisport events.17 During the 2008 Beijing Olympic Games, the IOC performed surveillance on all sports for the first time.2
Continuous injury and illness surveillance during major sporting events will build a foundation for providing evidence for the development of injury-prevention programs.1 The aim of the present paper was to summarise the injuries and illnesses that occurred in the previous two Olympic Games to enable the NOC physicians and medical personnel better prepare for the 2012 London Olympic Games. Practical implications and suggestions for further research to protect the athletes' health are provided.
Methods
In Beijing and Vancouver, all NOCs' head physicians participated in the Olympic surveillance studies and reported daily on the occurrence (or non occurrence) of newly sustained injuries and illnesses (only injuries in Beijing) on a standardised reporting form. The injury definition and data-collection procedures are described comprehensively elsewhere.2 3 17 In addition, information on all athletes treated for injuries and illnesses by the Local Organising Committee medical services were retrieved from the available medical centres located at selected venues. Athletes seen for an injury or illness in the venue medical stations or the central clinics were reported through the central clinic database.
Injury and illness report form
The report form on injuries and illnesses required broad documentation of the respective injury and illness. Detailed instructions on how to fill out the form correctly were given in the booklet with examples for injuries and illnesses. Daily injury information was also received from the polyclinics in the Olympic Villages. Injury and illness report forms were distributed to the NOCs in all required languages.2 3 17
Definition of injury and illness
An athlete was defined as injured or ill if he/she received medical attention regardless of the consequences with respect to absence from competition or training. Following the IOC injury-surveillance system, an injury should be reported if it fulfilled the following criteria: (1) musculoskeletal complaint or concussion, (2) newly incurred (pre-existing, not fully rehabilitated should not be reported) or re-injuries (if the athlete has returned to full participation after the previous injury), (3) occurred in competition or training and (4) occurred during the XXIX Summer Olympic Games 2008 (August 9–24, 2008) or the XXI Winter Olympic Games 2010 (February 12–28, 2010). An illness was defined as any physical complaint (not related to injury) newly occurred during the Games that received medical attention regardless of the consequences with respect to absence from competition or training.3
All information was handled confidentially and the injury reports were anonymised after the Olympic Games. Ethical approval was obtained by the Regional Committee for Medical Research Ethics, Region Øst-Norge, Norway.
Results
Response rate and coverage of the athletes
All NOCs with more than 50 (Beijing) or 10 registered athletes (Vancouver) were included in the analysis of response rate, and these countries represented more than 94% of all participating athletes.2 3 In Beijing, the head physicians of all the participating NOCs returned a total 1050 injury report forms (72%). In addition, 264 injury report forms were received from medical stations at the different Olympic venues and through daily reports from the polyclinic in the Olympic Village.2 Throughout the 17 days of the Vancouver Olympics, the 33 participating NOCs (with more than 10 athletes) returned a total of 461 out of a maximum of 561 forms (82%).3 In both Olympic Games, the response rate of completed forms by the NOC head physicians decreased with the size of the NOCs (defined by the number of participating athletes).
Injury risk in different sports
In the two Olympics, the overall injury rate was similar at around 10% of registered athletes sustaining at least one injury (table 1). The incidence of injuries varied substantially among the different sports, both in Beijing and in Vancouver (table 2). The risk of sustaining an injury was highest for football, taekwondo, field hockey, handball, weightlifting and boxing in Beijing (all ≥15% of the athletes).2 In Vancouver, injury risk was highest for bobsleigh, ice hockey, short track, alpine and for freestyle and snowboard cross (15%–35% of registered athletes were affected in each sport).3
Injury distribution of injuries from sports registered during the 2008 Summer Olympics (n=1055 injuries) and 2010 Winter Olympics (n=287 injuries)
Injury location and type
In Beijing, the distribution of injuries was as follows: about half of the diagnoses (54%) affected the lower extremity, 20% were related to the upper extremity, 13% to the trunk and 12% to the head/neck. The thigh (13%) and knee (12%) were most commonly injured, followed by the lower leg, ankle and head injuries (9%).2 In Vancouver, for both genders, the face, head and cervical spine (female 20%, male 21%) and knee (female 16%, male 11%) were the most prominent injury locations. In alpine, freestyle and snowboarding, 22 out of 102 injuries (22%) affected the head/cervical spine and one quarter of all injuries affected the knee (24%). Twenty concussions were reported, affecting 7% of the registered athletes. A death occurred in luge.3
Injury mechanism, circumstance and severity
In Beijing, one third of the 1055 injuries (33%) were caused by contact with another athlete. Non-contact trauma (20%) and overuse either with gradual (9%) or sudden onset (13%) were also frequent causes of injury.2 In Vancouver, the three most common reported injury mechanisms were a non-contact trauma (23%), contact with a stagnant object (22%) and contact with another athlete (15%) (table 1).3 While 73% of the injuries in Beijing occurred in the competition,2 in total 287 injuries in Vancouver were evenly distributed between official training (54%) and competition (46%) (p=.18).3
In Beijing, about half of the injuries were expected to prevent the athletes from further training or competition (50%). Physicians estimated that one third of the injuries would result in an absence from sport with up to 1 week.2 In Vancouver, of the 287 injuries, 65 (23%) were expected to result in a time-loss situation for the athlete. Of those with expected time loss, 11 injuries (17%) had an estimated absence from training or competition of more than 1 week (table 1).3
Incidence and distribution of illnesses (registered in Vancouver only)
Among 173 out of 2567 athletes (7%) in Vancouver, a total of 185 illnesses were reported, resulting in an incidence of 72.1 illnesses per 1000 athletes. Illnesses were reported from a variety of sports, and they mostly (63%) affected the respiratory system. The most frequent diagnosis was upper respiratory tract infection (pharyngitis, sinusitis, tonsillitis; 54%).
Discussion
This paper summarises the first two IOC surveillance projects and provides a direct comparison of the injury and illness occurrence of athletes between the 2008 Beijing Summer and 2010 Vancouver Winter Olympic Games. The findings show that of all participating athletes in the two most recent Olympic Games, about 10% and 7% suffered an injury or an illness, respectively. Certain team sports (such as soccer, ice hockey, field hockey, handball and basketball), martial art or weight class sports (such as taekwondo, boxing and weightlifting) and speed sports (such as bobsleigh and the skiing and snowboard disciplines) emerge as sports with high injury risk.2 3 Upper respiratory tract infection was the major cause of illness during the Vancouver Games.3
Incidence and distribution, type and cause of injuries
In Vancouver, the injury incidence was slightly higher than reported from the Summer Olympics in Beijing 2008 (111.8 vs 96.1 injuries per 1000 athletes).3 As illustrated for Winter sports by Torjussen and Bahr17 and for Summer sports by Junge et al,6 17 choosing the appropriate method to report the risk of injury in sports is challenging if one is comparing different sports or disciplines where exposure may differ considerably. During the Olympics, for example, athletes may perform 15 jumps in a high jump competition, take eight throws in a javelin competition, do one ski run in a 50 km cross-country race, five runs in snowboard cross, play several matches in soccer, basketball, or ice hockey and ‘only’ one to four starts in a 100 m sprint competition. Thus, as an alternative to relative injury risk where the risk is expressed as rate corrected for exposure, for example, injuries per playing hours/matches/runs, using the absolute injury risk is highly relevant for the present summary, where injuries and illnesses are expressed as the total number of injuries/illnesses per registered athletes for each sport/discipline.3
Having this in mind, athletics, soccer and ice hockey caused the greatest portion of injuries in the 2008 Summer2 and 2010 Winter Olympics.3 However, this does not necessarily mean that athletes in these sports were at the greatest risk of injury. The explanation is that these sports have a great number of competing participants. When calculating the injury risk in relation to the number of participating athletes, the picture is somewhat different. In Beijing, the risk of sustaining an injury was highest for soccer, taekwondo, field hockey, handball, weightlifting, boxing, basketball and athletics.2 These findings are consistent with the literature.6 11 18,–,22 In Vancouver, freestyle and snowboard cross, bobsleigh, ice hockey, short track and alpine skiing were the sports with the highest injury risk;3 this is consistent with new data from the FIS (The International Skiing Federation) injury-surveillance system.23,–,25
In both Summer and Winter sports, many of the injuries occur as a result from athlete-to-athlete contact, typical for team sports characterised by tackling. In addition to this, a lot of the winter sports also involve high speeds. In freestyle and snowboard cross, for example, athletes race while passing challenges such as turns, jumps and waves. Combined with the speed component, competing in heats may promote an additional risk-taking attitude for the athletes.24 Parallels can also be drawn to for example, velodrome and road cycling, when the athletes position themselves for the final sprint. However, overuse injuries constitute a high proportion of injuries in sports as swimming,13 athletics,12 beach volleyball14 and cycling.26 Capturing overuse injuries, including their injury mechanisms through the current injury surveillance methodology is still a challenge and a new standardised methodology to quantify overuse injuries in surveillance studies needs to be developed.27
The lowest injury risk during the Beijing Olympics was observed for water sports such as sailing, canoeing/kayaking, rowing, synchronised swimming, diving and swimming,2 which extends the findings in these sports at non-Olympic settings.21 22 28 The low injury risk for athletes competing in the Nordic skiing disciplines compared with alpine, freestyle and snowboard athletes is not surprising as they are not exposed to high speed on icy surfaces with minimal protection.24 29
In Vancouver, a major concern was that every fifth injury affected the head, neck and cervical spine, mainly diagnosed as abrasion, skin lesion, contusion, fracture or concussion. The figures for concussions were twice as high as reported from the Summer Olympic Games.2 Consequently, identifying mechanisms for concussion incidents should be of major importance. In many cases, head and knee injuries result in long absence from training and competition, and the prevention of concussions and severe knee ligament sprains, including anterior cruciate ligament ruptures, is important.
Incidence and distribution, type and cause of illnesses (registered in Vancouver only)
The incidence of illnesses from Vancouver is comparable with data from athletics (7%),12 aquatics (7%)13 and football (12%).11 Almost two thirds of the illnesses affected the respiratory system (62%) caused by infections (64%), which is a higher rate than reported in swimming (respiratory system 50%, infection 49%).13 Airway inflammation has been shown to often affect elite swimmers, ice-hockey players and cross-country skiers.30 It has been documented that good sanitation, early recognition and isolation of ill players can successfully reduce infections and illness in a team setting.31
Practical implications and further research
Introducing and implementing successful preventive measures relies, in part (eg, importance of compliance),4 on the proper characterisation of risk factors and mechanisms.32 Two recent reports describing situations leading to serious injuries in World Cup alpine skiing and snowboarding revealed that individual technical errors and inappropriate tactical choices33 and technical errors at take-off for jumping29 were primary causes of the injuries. These studies implicate that closer evaluations are necessary on course design and setting, race conditions, visibility and speed, and other technically difficult obstacles, such as height and distance between jumps.29 34
Analysing the inciting event of an injury, the moment when the injury occurs, will also be crucial for the better understanding of high-risk injury situations in Summer sports. Two main injury mechanisms have been identified for anterior cruciate ligament injury; one is during plant and cut and one-legged jump shot landings in team handball and basketball, the other when a large valgus force is combined with internal tibial rotation with the knee close to full extension.35 36
Hamstring strain injuries, typically occur during maximal acceleration and deceleration movements. A recent paper showed that hamstring muscles are most susceptible to strain injuries during the late swing phase of sprinting.37 Video analysis reveals that they occur during the final eccentric phase of the swing phase strike. This suggests that preventive measures should focus on eccentric hamstring strengthening exercises.38
By using video analysis and a model-based image-matching technique, detailed information on joint kinematics can be obtained from uncalibrated injury video recordings.39 This approach will help to better understand injury mechanisms and optimise preventive tools. The IOC research group is now analysing the most serious injuries sustained in Vancouver in an effort to improve the knowledge on injury risk factors and mechanisms in high-risk sports. A similar project will be started after the London Games to analyse high-risk Summer sports.
As the causes and mechanisms of an injury vary substantially between sports, successful preventive strategies need to be tailored to the respective sport and athlete at risk.2 40 The effect of potential measures to reduce injury risk will be monitored in upcoming Games.
As a new initiative to early address the next generation of future Olympic athletes, the IOC has created a new sporting event for young athletes. The first Summer Youth Olympic Games were held in Singapore in August 2010, and the first Winter Youth Olympic Games in Innsbruck, Austria in January 2012. These events each bring together around 5000 athletes, aged 14–18, from all over the world to participate in high-level Olympic competitions. Little is known about the injury risk of the young athlete competing at high-level sports.40 Consequently, a comprehensive injury and illness surveillance, based on the IOC model for previous Olympic Games, was initiated during the 9 days of the 2012 first Winter Youth Olympic Games.
The IOC and other major IFs, such as the International Football Association (FIFA),11 the International Aquatic Federation (Fédération Internationale de Natation)13 and the International Association of Athletics Federations12 have extended their injury surveillance in a second step to also include illnesses monitoring. In addition, the IOC is currently looking into developing an Electronic Health Record system, to be offered to the NOCs to facilitate periodic health evaluations. This will increase the pre and in-Games knowledge both on injuries and illnesses, and will help the IOC and NOCs to maximise the health protection of their elite athletes.1
In London 2012, the IOC with the NOCs and IFs will continue running the injury- and illness- surveillance system. Following the data from Beijing2 and Vancouver,3 the monitoring of the athletes' health will enable researchers and clinicians to follow the injury and disease trends in the various sports and further the work of the IOC Medical Commission on protecting the health of the athletes. The message from this and other long-term projects initiated by the IOC and the IFs is that we need to monitor the development of injury and illness rates over several years to identify potential risk factor and mechanisms for injury and illnesses in disciplines and sports. By acquiring new knowledge on injury and illness trends, we can optimise and target future research on risk factors, mechanisms and finally, prevention. The key to a meaningful study of epidemiology lies in a well-organised procedure for data collection with coordinated efforts from sports medicine professionals, coaches and athletes, combined with systematic subsequent analyses.
Conclusion
The present data collection procedures were well accepted by the medical staff of the NOCs as demonstrated by the high response rates of injury and illness forms. Ten per cent of the athletes incurred an injury during the XXIX Summer or XXI Winter Games, and 7% of the winter sport athletes suffered from at least one illness. The incidence of injuries and illnesses varied substantially between sports. In the future, risk factor and video analyses of injury mechanisms in high-risk Olympic sports would permit better understanding of injury mechanisms and thus help to direct injury prevention strategies. Periodic health evaluations will be instrumental to preventing injuries and illnesses, and hence, to protect the health of the athletes.
Acknowledgments
The research group wishes to acknowledge sincere gratefulness to the President of the IOC Medical Commission, Professor Arne Ljungqvist, and to NOCs and IFs for their strong support for these studies. The authors gratefully acknowledge the International Olympic Committee (IOC) for funding these studies. The authors also like to thank Professor Karim Khan for his valuable input to this paper.
References
Footnotes
-
Competing interests None.
-
Ethics approval All information was handled confidentially and the injury reports were anonymised after the Olympic Games. Ethical approval was obtained by the Regional Committee for Medical Research Ethics, Region Øst-Norge, Norway.
-
Provenance and peer review Commissioned; externally peer reviewed.