Article Text

Statistics from Altmetric.com
Introduction
Hamstring muscle strain-type injuries are common in sports that involve sprinting,1 acceleration, deceleration, rapid change in direction and jumping.2 ,3 Occurring in both recreational and professional sports, these injuries can result in substantial time lost from sport and commonly recur.4 ,5
In the Australian Football League (AFL), hamstring muscle strain-type injuries have displayed a high incidence rate, with a 10 year mean of 6.1 new injuries per club each year and a 23% average recurrence rate.6 A recurrence rate of 17% has been reported in elite soccer players7 with hamstring injuries also recorded as the most common injury accounting for 12% of all injuries and resulting in an average of four missed games per injury.8
The high incidence of hamstring muscle strain-type injuries and potential associated costs has resulted in a substantial amount of research into the factors related to such injuries. Two recent systematic reviews have been completed in an attempt to collate the evidence around risk factors for hamstring injuries.9 ,10 Both reviews identified hamstring muscle weakness and thigh muscle imbalance, muscle flexibility, previous hamstring injury, other previous injury and age as potential risk factors; however, these reviews concluded that single variables were inconsistently identified as associated factors. Both reviews provided a qualitative synthesis of the literature and included risk factor studies as well as intervention studies, where a potential risk factor was modified with a training programme. The inclusion of intervention studies may potentially complicate risk factor analyses, as such studies assume that the factor being modified is associated with the injury and that the factor can be modified by the treatment programme.
The aim of the current review was to assemble all available knowledge and data to identify the intrinsic and extrinsic risk factors associated with hamstring muscle strain-type injuries in sport.
Methods
Search strategy and identification of studies
A systematic literature search was conducted of Medline, CINAHL, Embase, AMED, AUSPORT, SPORTDiscus, PEDro and the Cochrane library from inception to August 2011. Where possible, key words (table 1) derived from the research question were mapped to subject headings (Supplemental file). To ensure all relevant articles were identified, citation tracking of all included articles was performed using Google Scholar, while reference scanning of the bibliographies of included articles was also performed. References yielded by the search were imported into Endnote X3 (Thomson Reuters, Newyork, USA) and duplicates were deleted.
Keywords for search strategy
Study selection criteria
To ensure consistent, unbiased selection of included studies, a set of inclusion and exclusion criteria were derived prior to database searching (table 2). Articles selected were limited to sports-related hamstring muscle strain-type injuries, not including tendon or avulsion injuries, as these commonly represent different pathological conditions and could be associated with alternative risk factors. Since the aim of this review was to identify the risk factors for hamstring injury, studies were required to have discrete data for hamstring injury, assessing some aspect of risk or associated factors.
Study selection criteria
Interventions that aimed to reduce the risk of sustaining a hamstring injury were excluded to limit the potential confounder of the effect of the intervention. Studies were also required to be prospective in nature. A retrospective design is unable to determine whether measured variables predisposed to, or were the result of, injury.11
Studies were required to be published in English and contain human participants. Articles were included if they were published in peer reviewed journals and full text was accessible. Abstracts from conferences and unpublished data were not included as the quality and rigor of such information may be questionable.
The titles and abstracts of each article in the Endnote library were analysed and selection criteria applied independently by two examiners (GF and TP). All articles determined to be potentially applicable were obtained in full text version. Criteria were reapplied to full text versions by both examiners in consultation.
Data collection and analysis
Assessing bias and methodological quality
Studies were not excluded based on quality. The purpose of the quality assessment was to examine the bias of each article rather than to specifically exclude any of them. The methodological quality of the included studies, except the systematic reviews, was evaluated by one examiner (GF) and checked by another examiner (TP) using a checklist validated for the assessment of the methodological rigor of both controlled and non-controlled studies.12 The checklist has demonstrated high internal consistency for non-randomised studies (Kuder Richardson-20 reliability coefficient = 0.89) and good test-retest (r=0.88) and inter-rater (r=0.75) reliability.12
The original scale consists of 27 questions but for the purposes of this review each study was only assessed on the most relevant questions. Questions 4, 8, 9, 13, 14, 15, 17, 19, 23, 24, 26 and 27 relate to intervention studies and were not applied. Of the included items, questions 1, 2, 3, 5, 6, 7 and 10 regarded reporting of aims, methods, data and results. Questions 11 and 12 were concerned with the external validity of studies, while questions 16, 18, 20, 21, 22 and 25 assessed the internal validity and bias. This modified tool has been used previously in a systematic review of factors associated with heel pain.13 Quality assessment results were presented as a percentage score.
The Critical Appraisal Skills Programme (CASP)14 was used to assess the quality of the previously published systematic reviews. The tool was modified to include only the most relevant questions. Items 6 and 7 were omitted as they did not allow for a score to be applied.
Data extraction
Relevant data extracted included the type of sport, participant numbers, sample details, number of injuries, risk factors investigated and how they were measured, how hamstring injury was diagnosed, the length of tracking of participants, and the results, including statistical techniques used and statistical results.
Data analysis
Data including means, SD, RR, OR and HR were extracted independently by two non-blinded reviewers (GF, TP). For continuous data, standardised mean differences (SDM) and 95% CI were calculated by dividing the injured and non-injured group means by the pooled SD. The SDM is a measure of the difference between players who sustained a hamstring injury and those who remained injury free. RR, OR and 95% CI were recalculated, where appropriate, from frequency tables of individual studies. The reported ratios were used when the studies did not provide adequate frequency data.
Where the data provided were appropriate, Comprehensive Meta-analysis Version 2.0 (BioStat, Englewood, New Jersey, USA) software was used to conduct a meta-analysis for the proposed risk factors for hamstring injury. To account for methodological or statistical heterogeneity, a random effects model was used. A random effects model makes no assumption about causes of variance in the sample distribution. It generates a wider CI around the pooled effect size than a fixed effects model, therefore it is less likely to find a significant effect and is considered a safer, more conservative option, with more accurate information obtained.15 Heterogeneity was assessed using the I2 statistic.16 This statistical test estimates the proportion of total variation in study estimates that is due to heterogeneity and is not dependent on the number of included studies. A value of 0% indicates no observed heterogeneity, less than 25% is considered to have low levels and a value of 100% indicates a completely heterogenous sample.
Results
Search results
The initial search yielded 1649 articles, 600 duplicates were removed, leaving 1049 potentially relevant articles. After application of the selection criteria to titles and abstracts, full texts of 52 articles were retrieved and criteria applied to the full text. A final list of 26 relevant articles was formed, with citation tracking and reference scanning revealing a further 18 for review, of which eight were included. Reference scanning and citation tracking of the newly included eight articles resulted in no new relevant studies being found. A total of 36 articles were therefore excluded of the 70 retrieved after the initial search, citation tracking and reference scanning had been performed. Eight review articles were excluded because they were not systematic reviews.17,–,24 Another two studies were omitted as they were retrospective designs25 ,26 and a further 11 were excluded on the basis that they had no specific risk factor data for hamstring injury.27,–,37 Six articles were excluded because they did not contain any discrete data regarding incidence or recurrence of hamstring muscle strain-type injury.38,–,43 Another two were excluded because they used an intervention programme,44 ,45 while a further six were excluded as they were either published abstracts46,–,49 or not published in peer-reviewed journals.50 ,51 One case study was excluded.52 A total of 34 articles were included for review.1 ,9 ,10 ,53,–,83
Characteristics and quality of included studies
Quality assessment scores for the included research studies ranged between 7 and 15 out of a possible 16 (table 3). Percentage scores ranged between 44 and 94% (Mean=83%).
Quality assessment scores for included studies
Eleven articles54 ,55 ,57 ,59 ,62 ,64 ,69 ,71 ,75 ,80 ,81 did not report on the reliability and validity of the tests to examine risk factors and subsequently did not score on item 20.
Twelve studies55 ,59 ,60 ,62 ,66 ,70 ,73 ,77 ,78 ,80,–,82 did not use adequate adjustment for confounding variables, particularly previous injury and age. Without adequate adjustment for confounding variables, the results of some studies may not be accurate. The CASP quality scores for the systematic reviews demonstrated that all studies scored 7 out of a possible 8 on the scale (table 4).
Systematic review quality assessment
Fourteen of the prospective studies included investigated hamstring muscle strain-type injuries in Australian football,1 ,54 ,55 ,58 ,63,–,66 ,69 ,71 ,74,–,77 10 studies investigated soccer,53 ,56 ,60,–,62 ,67 ,68 ,72 ,78 ,79 five studies investigated track and field59 ,70 ,73 ,81 ,82 while two studies investigated rugby.57 ,80 The follow-up period varied between 3 weeks and 8 years (Supplemental file).
Evaluation of risk factors
Age
Seventeen studies investigated the influence of age as a risk factor for hamstring muscle strain-type injuries.1 ,53 ,57 ,61 ,62 ,64 ,65 ,67,–,69 ,71 ,74,–,77 ,79 ,82 Seven studies (3199 participants) were included in a meta-analysis using SDM data and three using RR data (figures 1 and 2). The results support age as a significant risk factor for injury (SDM=2.5, 95% CI 0.78 to 4.15, p=0.004, I2=99%). Figure 2 illustrates that athletes of older age tended to be at increased risk of sustaining a hamstring injury (OR=2.46, 95% CI 0.98 to 6.14, p=0.06, I2=73%).

Standardised mean difference and 95% CI for age as a risk factor.

RR for age as a risk factor.
Of the seven studies not included in the meta-analyses, two found age to be a significant risk factor for hamstring muscle strain-type injuries. Hagglund et al67 found age (HR=1.1, 95% CI 1.0 to 1.2, p=0.02) to be a significant risk factor, while Woods et al79 found 17–22 year old age groups sustained fewer hamstring strains than the older soccer players (p<0.01). Two studies reported that age was not a significant factor for injury1 ,57 and a further three studies found that age was not associated with injury recurrence.69 ,74 ,76
Body mass index/height/weight/body composition
Body mass index (BMI)
Seven studies (835 participants) evaluated the effect of BMI on hamstring muscle strain-type injuries.53 ,57 ,61 ,64 ,67 ,74 ,80 Meta-analysis using three studies53 ,61 ,80 demonstrated no association between BMI and hamstring injury (SDM=1.28, 95% CI −1.35 to 3.90, p=0.34, I2=98%).
In agreement with the results of the meta-analysis, BMI was not found to be associated with hamstring injuries in a group of rugby players,57 nor was it associated with recurrent hamstring injuries.67 ,74 Of the four studies not included in the meta-analysis, only Gabbe et al64 showed that BMI >25 was associated with hamstring muscle strain-type injuries (RR=2.41, 95% CI, 1.25 to 4.66, p=0.01).
Weight
Fifteen studies evaluated the influence of weight on hamstring muscle strain-type injuries in 762 athletes.1 ,53 ,57 ,61 ,62 ,64 ,67 ,69 ,71 ,74,–,77 ,80 ,82 The seven studies included in the meta-analysis did not demonstrate a difference in weight between the injured and non-injured groups, although there was a trend towards heavier athletes being more susceptible to hamstring injury (SDM=0.94, 95% CI −0.059 to 1.19, p=0.07, I2=97%) (figure 3).
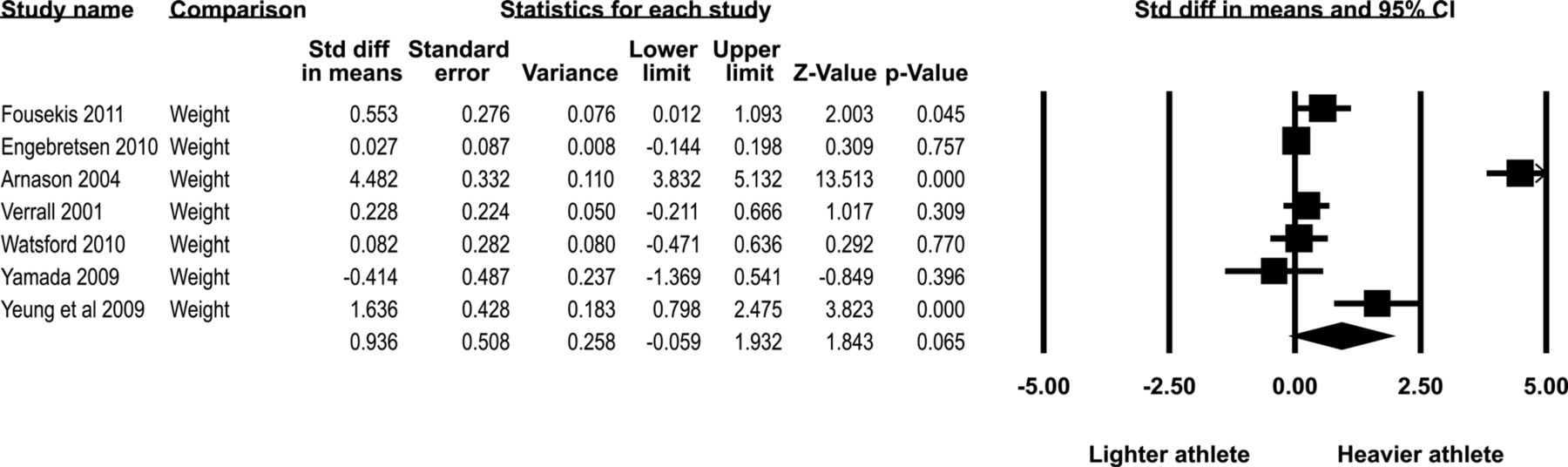
Standardised mean difference and 95% CI for weight as a risk factor.
Two other studies found no association between weight and hamstring muscle strain-type injuries,1 ,57 while four studies did not find any correlation between weight and recurrent hamstring injury.67 ,69 ,74 ,76 However, two studies64 ,71 did demonstrate an association between weight and hamstring muscle strain-type injuries, although Gabbe et al64 identified this association only in football players aged ≥25 years. They reported that for each kilogram increase in body weight, the risk of sustaining a hamstring injury increased by 7%. Since BMI has been correlated with player age and previous injury, this association may be confounded by these variables.71
Height
Fifteen studies (1557 participants) investigated height as a risk factor.1 ,53 ,57 ,61 ,62 ,64 ,65 ,67 ,69 ,74,–,77 ,80 ,82 Seven studies53 ,61 ,62 ,75 ,77 ,80 ,82 were eligible for meta-analysis using the SMD and two studies were included in a RR meta-analysis.64 ,65 Standardised mean difference meta-analysis suggested height did not differ between groups of injured and non-injured players (SDM=−0.03, 95% CI −0.12 to 0.18, p=0.72, I2=8%). For the RR analysis, height was not found to be a risk factor for hamstring muscle strain-type injuries (RR=1.52, 95% CI 0.76 to 3.03, p=0.24, I2=0).
Of the six studies not included in the analysis, height was not significantly associated with first time1 ,57 or recurrent hamstring injury.67 ,69 ,74 ,76
Strength
H:Q ratio
A meta-analysis was completed using five studies1 ,55 ,58 ,68 ,80 that measured conventional concentric H:Q ratio. The analysis included 216 athletes and assessed the results of isokinetic testing at a slow speed (60°/sec). The meta-analysis demonstrated no difference between groups (SDM=−0.50, 95% CI −1.17 to 0.18, p=0.15, I2=70%), (figure 4).
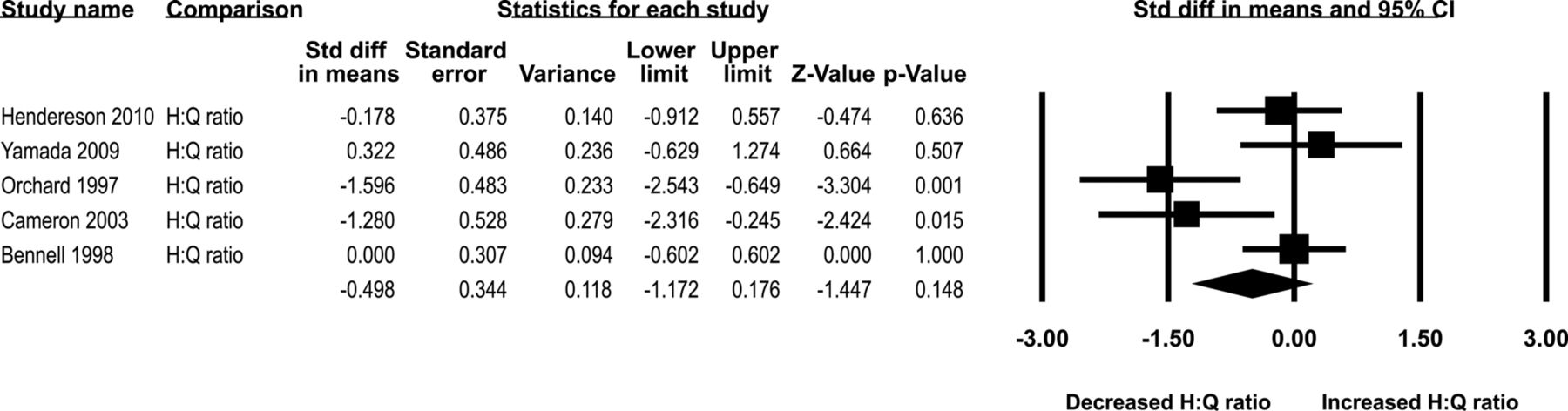
Standardised mean difference and 95% CI for concentric hamstring: quadriceps ratio.
Studies have used a number of other methods to measure H:Q ratio, varying the speed of testing and type of muscle contraction. Yeung et al82 identified that the risk of hamstring muscle strain-type injuries increased with a decrease in conventional concentric H:Q ratio at 180°/sec. A ratio of less than 0.6 was found to increase injury risk by 17 times (HR=17.4, 95% CI 1.31 to 231.4, p=0.03). However, ratios tested at slower speeds and using different concentric/eccentric combinations in the same study were not identified as risk factors. Similarly, Bennell et al55 found H:Q ratios could not predict hamstring muscle strain-type injuries despite measuring ratios at varying speeds and using differing combinations of eccentric and concentric contractions. In addition, Orchard et al1 found concentric H:Q ratios at 180°/sec and 300°/sec were not different between injured and non-injured groups despite being significantly different at 60°/sec. Overall, the evidence for isokinetic H:Q ratio being a risk factor for hamstring muscle strain-type injuries is sparse when considered in isolation regardless of the speed and contraction type.
Croisier et al60 found that identifying an imbalance profile (ie, a player who has a deficit on two or more isokinetic tests) was an effective method of identifying at-risk players. Soccer players were 4.66 times more likely to sustain a hamstring muscle strain-type injury (OR=4.66, 95% CI 2.01 to 10.8) if they were classified as having a strength imbalance in the preseason. Fousekis et al62 and Sugiura et al73 were also interested in imbalances of isokinetic strength and ratio tests between each leg of participants. Both studies used functional H:Q ratios (eccentric hamstrings to concentric quadriceps) and Suguira et al tested at speeds of 60, 180 and 300°/s, while Fousekis et al tested only at 180°/s. Functional H:Q ratio asymmetry between legs was identified as a risk factor only when measured at the slower speed of 60°/s.
None of the studies that utilised isokinetic dynamometry examined isometric H:Q ratios, however two older studies used strain gauges to examine isometric H:Q ratios and did find that a decrease in this ratio was a risk factors for hamstring muscle strain-type injuries.59 ,81
Hamstring peak torque
Four studies (195 participants) gathered data for hamstring peak torque (concentric) values.1 ,55 ,58 ,68 A meta-analysis including all four studies did not support hamstring peak torque as a risk factor for hamstring muscle strain-type injuries (SDM=−0.24, 95% CI −0.85 to 0.37, p=0.44, I2=58%). Bennell et al55 also analysed eccentric hamstring peak torque but did not find any significant difference between groups.
Quadriceps peak torque
Four studies (195 participants) assessed quadriceps peak torque.1 ,55 ,58 ,68 A meta-analysis supported an increase in quadriceps peak torque as a risk factor for hamstring muscle strain-type injuries (SDM=0.43, 95% CI 0.05 to 0.81, p=0.03, I2=0) (figure 5). Bennell et al55 also analysed eccentric quadriceps peak torque in Australian football players but did not find any difference between those who sustained a hamstring injury and those who did not.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Standardised mean difference and 95% CI for quadriceps peak torque as a risk factor.
Hamstring to opposite hamstring ratio
Risk of hamstring strain increased with a lower hamstring to opposite hamstring (H:Hopp) concentric ratio at 60°/s (p=0.00) in an Australian football population.1 While eccentric hamstring strength asymmetries were predictive of hamstring muscle strain-type injuries in soccer players (OR=3.88, 95% CI 1.13 to 13.23, p=0.03), however concentric strength asymmetries were not.62 In another study of Australian football players, there were no differences in H:Hopp ratios between injured and non-injured groups regardless of the speed of isokinetic testing or type of contraction, except for eccentric 180°/s where a ratio greater than 0.90 was found to be predictive of injury (p=0.02).55
Other strength measures
Engebretsen et al61 found that a simple eccentric strength test was not associated with an increased risk of hamstring muscle strain-type injuries. Sugiura et al73 identified that weakness during concentric contraction of the hip extensors was associated with hamstring injury, but only when tested at 60°/s.
Previous injury
Previous hamstring injury
Thirteen studies reported on previous hamstring injury as a potential risk factor in hamstring muscle strain-type injuries.1 ,53 ,55 ,61 ,62 ,64 ,67,–,69 ,71 ,75,–,77 Meta-analysis including 2952 athletes supports the conclusion of previous hamstring injury being a risk factor for future injury (RR=2.68, 95% CI 1.99 to 3.61, p=0.00)64 ,71 ,76 and (OR=4.06, 95% CI 2.39 to 6.89, p=0.00).53 ,61 ,75 ,77 Heterogeneity was low across studies for OR (I2=29%) and RR (I2=22%).
In addition, Bennell et al55 found that Australian football players with a previous history of hamstring muscle strain-type injuries were 2.1 times more likely to sustain another hamstring injury (p=0.02) and Hagglund et al67 reported a HR of 3.5 (95% CI 1.9 to 6.5, p=0.00) for elite soccer players who had experienced a previous hamstring injury. Koulouris et al69 identified a trend towards increasing risk of recurrence with a history of previous hamstring muscle strain-type injury (p=0.07). Only two studies did not find an association with previous hamstring injury1 ,68 and one study found a past history of hamstring injury to be protective against recurrence (OR=0.15, 95% CI 0.29 to 0.79, p=0.02).62
Other previous injuries
Interestingly, three studies identified other injuries to be associated with hamstring muscle strain-type injuries. Koulouris et al69 demonstrated an association between history of ACL reconstruction and recurrent hamstring injury (p=0.00)69, Orchard70 found that history of calf muscle strain (more than 8 weeks previously) was associated with risk of hamstring injury (RR=1.37, 95% CI 1.08 to 1.76), while Verrall et al74 reported that hamstring injury was associated with a past history of knee injury (p=0.04) and a past history of osteitis pubis.
Flexibility and range of motion
Length and flexibility of hamstring
Five studies assessed the length of the hamstring muscle as a risk factor using the active knee extension (AKE) test.64 ,65 ,70 ,72 ,76 The meta-analysis (407 participants) of two of these studies64 ,65 did not identify AKE hamstring length results as a risk factor. (RR=1.89, 95% CI 0.93 to 3.83, p=0.08, I2=0).
Of the three studies not included in the meta-analysis, Rolls and George72 found no statistically significant relationship between poor hamstring flexibility and hamstring muscle strain-type injuries in young soccer players, and Warren et al76 found no association with recurrence (RR=1.4, 95% CI 0.8 to 2.6, p=0.27). Malliaropoulos et al70 reported that recurrent hamstring injuries were more likely in athletes with an AKE deficit of 10–19 degrees at 48 h after the initial injury, compared with larger and smaller AKE deficits.
Three studies measured hamstring length using the passive knee extension (PKE) test.53 ,61 ,72 A total of 907 participants were included in the meta-analysis. There was no significant difference between the injured and non-injured groups (SDM=1.13, 95% CI −1.08 to 3.35, p=0.32). There was significant heterogeneity across the studies (I2=99%). Fousekis et al62 also found no association between bilateral asymmetries in hamstring length and hamstring muscle strain-type injuries. In contrast, two studies established that a reduced mean ROM for the knee flexors increased the chance of hamstring injuries occurring in soccer players.56 ,78
In addition, another study showed mean hamstring musculotendinous stiffness (p=0.04) and mean leg stiffness (p=0.03) were greater in AFL players who subsequently sustained a hamstring muscle strain-type injury.77
Other range of motion tests
Three studies found reduced hip extension ROM (or reduced hip flexor length) to be associated with subsequent hamstring injury.56 ,63 ,68 Gabbe et al63 identified that for each 1° increase on the modified Thomas test (ie, decreasing hip flexor flexibility), the risk of hamstring muscle strain-type injury increased 15% in players aged ≥25 years. Hip internal and external ROM was not associated with injury (p>0.05).64
There is some evidence for an increased probability of sustaining a hamstring injury with decreased quadriceps flexibility65 ,78 or dorsiflexion lunge ROM (RR=2.32, 95% CI, 0.97 to 5.56, p=0.05).64 However, bilateral asymmetries in flexibility for the quadriceps and plantar flexor muscles were not shown to be risk factors for injury.62 Slump test,64 ,76 lumbar spine flexion, lumbo-femoral ratio,54 straight leg raise,76 ,82 and sit and reach test results,1 ,54 were not significantly different between athletes who subsequently went on to strain a hamstring or suffer a recurrence and those who did not.
MRI data
Three studies assessed hamstring muscle strain-type injuries with MRI to determine risk factors for re-injury.66 ,69 ,74 Athletes with an injury volume greater than 21.8 cm3 were 2.3 times more likely to be reinjured (95% CI, 0.94 to 5.81, p=0.04) and an MRI-measured injury transverse size greater than 55% were 2.2 times (95% CI, 0.88 to 5.32, p=0.02) more likely to be reinjured.74 Although Verrall et al74 did find the cross sectional area (CSA) of the injured tissue on MRI to be significantly associated with risk of recurrent hamstring injury, both Koulouris et al69 and Gibbs et al66 found no association between CSA or length of injury on MRI and risk of recurrent injury.
Convalescent interval, injury location, principal muscle injured, and the number of muscles injured were not associated with the risk for recurrent injury within the same playing season.74
Limb dominance
No significant differences were observed in the number of hamstring injuries between the dominant and the non-dominant leg.1 ,68 ,74 ,78 In addition, preferred kicking leg did not correlate with injury in Australian football players.1
Playing position
The incidence of hamstring muscle strain-type injuries in rugby union was significantly higher for backs (8.6 injuries/1000 player hours; 95% CI, 6.5 to 10.6) than for forwards (3.0 injuries/1000 player hours; 95% CI, 1.9 to 4.1),57 while soccer goalkeepers sustained significantly fewer injuries than outfield players (p<0.01).79
Functional measures
Ten studies looked at a variety of different functional measures to try and identify athletes who may be at risk of hamstring muscle strain-type injuries. Movement discrimination scores were worse in the subsequently injured group compared to the non-injured group (p=0.01),58 while subsequent hamstring injury in university rugby players could be predicted by a slower time on a motor imagery task.80 For the non-counter movement jump test, the odds of sustaining an injury increased by 1.47 with every 1 cm extra achieved (OR=1.47, 95% CI 1.02 to 2.12, p=0.04).68 A functional leg length discrepancy of >1.8 cm was also found to be a risk factor for hamstring muscle strain-type injuries (OR=3.80, 95% CI 1.08 to 13.33, p=0.03).62
Measured factors that did not significantly correlate with injury or recurrent injury included level of abdominal strength, VO2max results, various measures of anaerobic fitness1 pain provocation test, time to ascend stairs pain-free, mechanism of injury,76 maximal average power, counter movement jump (CMJ), CMJ on one leg, standing jump, peak O2 uptake, player exposure,53 jumping ability, running speed61 and knee laxity asymmetry.62
Ethnicity
Three studies evaluated the ethnic origin of athletes as a potential risk factor. Two studies found an association with a significantly increased risk in players of Aboriginal descent (p=0.04),75 and players of black origin (p<0.05).79 One study found no significant difference in incidence of hamstring injuries as a function of ethnic origin.57
Work rate
Two studies did not show any significant findings for a difference in the amount of time spent in training and games78 and frequency of off season running (p=0.14).65
Type of activity
A significantly higher proportion (68%, p=0.00) of hamstring muscle strain-type injuries were sustained during running activities than during any other activity, but the highest severity injuries were sustained during kicking.57
Discussion
The risk factors most consistently associated with hamstring muscle strain-type injuries were age, previous hamstring injury and quadriceps peak torque. Some risk factors require further research to adequately clarify their involvement due to inconclusive results, small sample sizes or very few studies on their influence. These risk factors include hamstring flexibility (measured via the AKE test), weight, hip flexor flexibility, quadriceps flexibility, ankle dorsiflexion lunge ROM, playing position, proprioception (movement discrimination test), mental imagery, ethnicity, hamstring peak torque (strength) and H:H ratio.
The results of this review showed that there are many risk factors that appear to have little correlation with hamstring muscle strain-type injuries. These were BMI, height, passive length of hamstring, dominant limb, abdominal strength, VO2 max, various measures of anaerobic fitness, pain provocation test, time to ascend stairs pain-free, slump test, mechanism of injury, maximal average power, CMJ, CMJ on one leg, standing jump, peak O2 uptake, player exposure, jumping ability, knee laxity and running speed.
Three other systematic reviews9 ,10 ,83 all found hamstring strength to be a risk factor. The meta-analysis in this review does not fully support their findings. Foreman et al9 and Prior et al10 both associated hamstring muscle strain-type injuries with decreased hamstrings flexibility and previous injury. This review does not support hamstrings flexibility as a risk factor due to conflicting evidence and the meta-analysis did not demonstrate a significant relationship between AKE test results and hamstring injury, although this analysis was approaching significance (p=0.08). All three reviews found previous history of hamstring injury to be significant, which is supported by the findings from the present review.
The study by Arnason et al53 appeared to be a factor in the heterogeneity in the meta analysis for risk factors such as age, BMI, weight and hamstring flexibility (measured via the PKE test). This study was of high quality and involved elite-level soccer players, however the large age range (16–38 years) of the participants may have contributed to the heterogeneous findings. The spread in the age perhaps led to a greater difference shown between injured and non-injured groups, which potentially demonstrates that the risk of injury continues to increase as age increases and that there is an important relationship between age, BMI and flexibility. A meta-analysis cannot compensate for inadequacies in the original data extracted from the studies. There is the possibility for error in the meta-analysis calculations and despite a random effects model being used, heterogeneity may still be a problem.
The large number of variables examined results in a complicated picture of risk profile for hamstring muscle strain-type injuries. The tendency to assess the variables in isolation may further confound the picture, since important interactions between variables may be missed and the influence of some risk factors may be overstated. The findings from this review highlight that the factors of age and previous hamstring injury must be considered alongside any other risk factors being examined. The interaction between risk factors is likely important, since hamstring muscle strain-type injury is considered to be a multi-factorial problem.9
Conclusion
The evidence demonstrates that older age, increased quadriceps peak torque and past history of hamstring injury were associated with increased risk of hamstring muscle strain-type injuries in sport. Further research is required using multivariate models to identify which factors are inter-related. This information could assist researchers to develop effective intervention programmes to prevent these injuries from occurring and decrease their impact on primarily the athletes but also their respective teams.
What is already known on this topic?
-
Hamstring muscle strain injuries (HMSI) are common in sport and there is a high rate of recurrence. Many papers have examined potential risk factors for HMSI, with age and previous hamstring strain being accepted as risk factors, and many others inconsistently identified as contributing to the injury. Qualitative reviews have been undertaken on this topic, but a meta-analysis of risk factor studies has not been performed.
What this study adds?
-
Meta-analysis identified age, previous history of hamstring strain and increased quadriceps peak torque as risk factors for HMSI. Other strength measures such as hamstring:quadriceps ratio, commonly perceived to be predictive of injury, were not associated with HMSI. This study highlights risk factors that require further investigation to confirm their involvement in HMSI and risk factors that have no association and need not be tested in future studies.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmjgroup.com