Article Text

Abstract
Objectives To examine the time course of changes in wellness and health status markers before and after episodes of sickness in young soccer players during a high-altitude training camp (La Paz, 3600 m).
Methods Wellness and fatigue were assessed daily on awakening using specifically-designed questionnaires and resting measures of heart rate and heart rate variability. The rating of perceived exertion and heart rate responses to a submaximal run (9 km/h) were also collected during each training session. Players who missed the morning screening for at least two consecutive days were considered as sick.
Results Four players met the inclusion criteria. With the exception of submaximal exercise heart rate, which showed an almost certain and large increase before the day of sickness (4%; 90% confidence interval 3 to 6), there was no clear change in any of the other psychometric or physiological variables. There was a very likely moderate increase (79%, 22 to 64) in self-reported training load the day before the heart rate increase in sick players (4 of the 4 players, 100%). In contrast, training load was likely and slightly decreased (−24%, −78 to −11) in players who also showed an increased heart rate but remained healthy.
Conclusions A >4% increased heart rate during submaximal exercise in response to a moderate increase in perceived training load the previous day may be an indicator of sickness the next day. All other variables, that is, resting heart rate, heart rate variability and psychometric questionnaires may be less powerful at predicting sickness.
- Altitude
- Cardiology prevention
- Fatigue
- Physiology
- Soccer
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
While altitude training camps are often used in soccer to improve performance at sea level,1 ,2 their effect on health and well-being is questionable. At moderate-to-high altitudes, short episodes of sickness or illness can occur, including acute mountain sickness (AMS) and non-AMS-related gastrointestinal symptoms.3 These episodes are problematic as they can potentially negate the expected improvements in exercise performance.4 ,5 The need therefore exists to determine the effectiveness of monitoring player wellness and health status at altitude using simple methods to help prevent sickness and/or maintain the training process.
The use of questionnaires to monitor wellness6 ,7 and health status at altitude8 is common practice. There is also growing interest for indirect measures of cardiac autonomic activity such as heart rate variability9 ,10 and heart rate responses to submaximal exercise.11 These measures have been associated with short-term, training-induced fatigue,7 ,10 AMS9 ,11 and physical performance acclimatisation to altitude.12 ,13 In most studies these variables were only examined once the participants were diagnosed as sick. Therefore, whether these markers show specific patterns before the onset of sickness, and can be used to predict sickness, is still unknown.
The aim of the study was to examine the time course of selected psychometric and physiological markers of wellness and health status before and after episodes of sickness during a high-altitude training camp.
Methods
Study overview
In total, 20 Australian and 19 Bolivian soccer players participated in the study.14 The complete study overview has been reported in our companion papers.12 ,14 The project was approved by the Ethics Committees of the Australian Institute of Sports and of the ‘Instituto Boliviano de Biología de Altura’, the latter through University Mayor de San Andres, La Paz, Bolivia. All players, or their guardians if under 18 years, provided written consent. As the severity and nature of sickness can be subjective, a sickness episode was objectively defined as the inability of a player to attend the morning screening session for at least two consecutive days. Training load was calculated for all players as total training duration (minutes)×session rating of perceived exertion (RPE).15 Resting heart rate and the SD of the instantaneous beat-to-beat R–R interval variability measured from Poincaré plots (LnSD1) were collected daily soon after waking (except day 7) as the players sat quietly. These values were calculated using the last 3 min of a 8 min recording. Additional well-being and health status measures including RPE and heart rate (average over the last minute) responses to a 5 min submaximal run (9 km/h), wellness using a psychometric questionnaire16 and AMS severity (Lake Louise AMS questionnaire)8 were also collected.
Data analysis
To examine which psychometric and physiological markers may predict sickness, we analysed the time course of changes in these variables over the 4 days before the first day of absence. Because subtle changes in training load had a very large effect on these psychometric and physiological variables,7 changes in training load over the 4 days before sickness were also analysed.
All data in the text and figures are presented as mean change or difference with 90% confidence limits (CL) and CI, respectively. All data were log-transformed to reduce bias arising from non-uniformity errors. Standardised differences/changes in all monitored variables were calculated using pooled between-subject SD. Threshold values were >0.2 (small), >0.6 (moderate) and >1.2 (large).17 Uncertainty in each effect was expressed as 90% CL and as probabilities that the true effect was substantially positive or negative. These probabilities were used to make a qualitative inference about the true effect.17
Results
Four players met the inclusion criteria having missed the morning screening on two (n=3) or three (n=1) consecutive occasions (occurring on the 3rd, 5th, 8th and 10th day at altitude).
With the exception of submaximal exercise heart rate, which showed an almost certain and large increase before the day of sickness (4%; 3, 6), there was no clear change in any of the other psychometric and physiological variables (figure 1). After sickness, resting heart rate (almost certain at day 1), LnSD1 (almost certain at day 1 and likely at day 2), RPE response to the submaximal run (very likely at day 1) and Lake Louise score (likely at day 1 and day 2) were moderately to very largely affected and returned to normal within 2–3 days (figure 1). There was no clear change in wellness after the sickness episode.
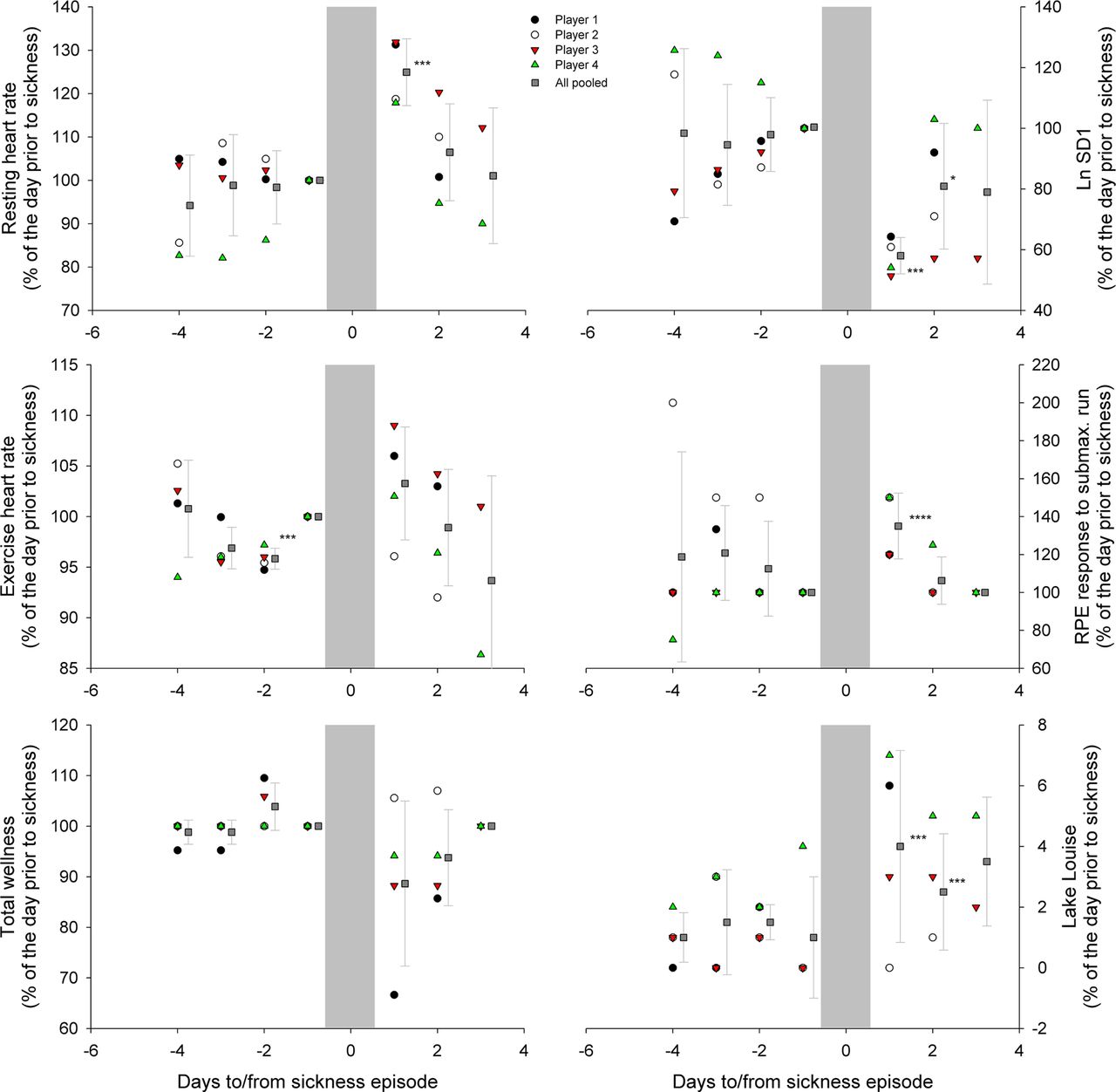
Individual and mean (±SD) values for the four sick players. Changes in resting heart rate, resting vagal-related heart rate variability (LnSD1), heart rate response to the 5 min submaximal run, rate of perceived exertion response to the 5 min submaximal run, total wellness and Lake Louise scores. Symbols indicate clear standardised changes compared with the day before sickness, with *, **, *** and **** standing for small, moderate, large and very large changes, respectively. Access the article online to view this figure in colour.
Changes in daily training loads and exercise heart rate in players presenting with a >4% increase in submaximal exercise heart rate, irrespective of sickness status, are shown in figure 2. There was a very likely moderate increase in perceived training load (day 3 vs 2) the day before the heart rate increase (day 2 vs 1) in all players who became sick. In contrast, there was a likely small decrease in training load in the majority of players who also showed an increased heart rate but remained healthy (n=23 players, substantially decreased in 15, increased in 7 and no change in 1).

{kind=link}
{kind=link}
Mean daily training load (SD, upper panel) in all players who demonstrated a >4% increase in heart rate in response to the standardised submaximal exercise and became sick or not. Measures are reported over 4 days. The lower panel shows the changes in training load and exercise heart rate from 2 to 1 day prior to sickness for both groups of players. Numbers indicate standardised changes (90% CI) from 3 to 2 (training load) and 2 to 1 (heart rate) days before sickness, or difference in the change in training load between the two groups. The grey areas represent trivial between-group differences (training load) or within-group changes (heart rate).
Discussion
Our main findings were (1) submaximal exercise heart rate was the only variable to show a consistent pattern (very large increase) before sickness; (2) in all players who became sick, the elevated heart rate was associated with a moderate increase in perceived training load the preceding day; (3) when an increased heart rate was observed following a small decreased training load, players did not become sick; and (4) after sickness, most of the moderate to very large changes in psychometric and physiological measures returned to normal within 2–3 days.
Resting cardiac parasympathetic activity (ie, resting heart rate and LnSD1) was not affected before sickness. There is conflicting data on the responses of the autonomic nervous system to sickness at high altitude, with studies reporting either unaffected18 or increased9 ,11 markers of (cardiac) sympathetic activity. Exercise heart rate was largely increased before sickness, suggestive of an increased sympathetic activity during exercise.11 The explanation why exercise heart rate but not heart rate variability measures was predictive of sickness is unclear, but the greater reliability of exercise heart rate (coefficient of variation 319 vs 1220), and sensitivity of both measures to subtle changes in perceived training load might partly explain these results. In elite Australian Rules Football players under sickness-free conditions, there was a very large negative relationship between day-to-day changes in heart rate exercise and training load, probably as a consequence of exercise-induced changes in plasma volume.21 In healthy players only, the greater the decrease in training load the preceding day, the greater the increase in exercise heart rate.21 In the present study, this relationship was observed in healthy players only (figure 2). In the players who became sick, a moderate increase in perceived training load the previous day was associated with an increase in heart rate, instead of a decrease (figure 2). In addition to sustained sympathetic activity, this increased heart rate could be interpreted as an inability to retain fluids (limiting plasma volume expansion) as a consequence of excessive dehydration. Taken together, these results confirm the need to consider daily training loads when interpreting changes in heart rate measures,7 and that the ‘normal’ relationship may be inverted before sickness.
Importantly, 35% of the players who presented with the criteria suggested to be predictive symptoms (ie, >4% increased heart rate in response to a subtle increase in training load the day before) remained healthy. Additional measures may be needed to improve the sensitivity and specificity of the diagnosis. It is also possible that these players also became sick, but not enough to miss the screening measures. Differences in sickness severity were unfortunately not monitored, which is a limitation of our study and requires further research. We nevertheless believe that adopting a conservative management approach for athletes during altitude training camps is preferred to help reduce the likelihood/risk of illness impairing health and training.
Neither wellness nor Lake Louise scores showed consistent trends before sickness (figure 2). These results are surprising given both the generalised use of the latter questionnaire to assess AMS, and the moderate correlations between Lake Louise scores and cardiac autonomic perturbations.9 Since the four sickness episodes occurred ≥3 days after arrival, and considering that AMS generally occurs within the first hours after arrival at altitude, it is possible that players might have missed the screening for reasons other than AMS (eg, gastrointestinal disorders, and/or upper respiratory tract infection). Taken together, the present data confirm that monitoring physiological data may be more powerful than psychometric indices in predicting changes in player condition at altitude.12
Finally, the large changes in most of the variables after sickness show that these episodes have a substantial impact on player condition. On average 2–3 days are required to fully recover both psychologically and physiologically. Whether physical performance recovers similarly remains to be investigated, but the large relationships that some of these markers (ie, exercise heart rate12) share with performance suggest a similar time course.
Conclusion
Pending confirmatory research on a larger group of players, an increased heart rate during submaximal exercise following a subtle increase in perceived training load the day before may be an indicator of increased risk of sickness the next day. All other variables examined, that is, resting heart rate, heart rate variability and psychometric questionnaires were less powerful at predicting sickness.
What is known on this subject
-
Living and training at high altitude presents a physiological challenge for native sea-level athletes; with depressed immune function, altered autonomic function, acute mountain sickness and sleep disturbance often reported.
-
Psychometric and physiological measures, such as questionnaires or resting heart rate, are used as indicators of general acclimatisation and tolerance to altitude.
What this study adds
-
A >4% increased heart rate during submaximal exercise, in response to a moderate increase in perceived training load the day before, may be predictive of sickness the following day.
-
All other variables examined including resting heart rate, heart rate variability or psychometric questionnaires do not show consistent changes before sickness.
Footnotes
-
Contributors All authors were involved in the conception and design, or analysis and interpretation of data, drafting the manuscript or revising it critically for important intellectual content, and approved the final version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics Committees of the Australian Institute of Sport and of Instituto Boliviano de Biología de Altura, the latter through University Mayor de San Andres, La Paz, Bolivia.
-
Provenance and peer review Not commissioned; externally peer reviewed.