Article Text

Abstract
Repeated sprint ability (RSA) is a critical success factor for intermittent sport performance. Repeated sprint training has been shown to improve RSA, we hypothesised that hypoxia would augment these training adaptations. Thirty male well-trained academy rugby union and rugby league players (18.4±1.5 years, 1.83±0.07 m, 88.1±8.9 kg) participated in this single-blind repeated sprint training study. Participants completed 12 sessions of repeated sprint training (10×6 s, 30 s recovery) over 4 weeks in either hypoxia (13% FiO2) or normoxia (21% FiO2). Pretraining and post-training, participants completed sports specific endurance and sprint field tests and a 10×6 s RSA test on a non-motorised treadmill while measuring speed, heart rate, capillary blood lactate, muscle and cerebral deoxygenation and respiratory measures. Yo-Yo Intermittent Recovery Level 1 test performance improved after RS training in both groups, but gains were significantly greater in the hypoxic (33±12%) than the normoxic group (14±10%, p<0.05). During the 10×6 s RS test there was a tendency for greater increases in oxygen consumption in the hypoxic group (hypoxic 6.9±9%, normoxic (−0.3±8.8%, p=0.06) and reductions in cerebral deoxygenation (% changes for both groups, p=0.09) after hypoxic than normoxic training. Twelve RS training sessions in hypoxia resulted in twofold greater improvements in capacity to perform repeated aerobic high intensity workout than an equivalent normoxic training. Performance gains are evident in the short term (4 weeks), a period similar to a preseason training block.
- Altitude
- Rugby
- Exercise physiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Most team and racket sports involve repeated short duration sprints (<10 s) with brief recovery intervals (<60 s). To achieve a high level of such repeated sprint ability (RSA), athletes must reach high peak speeds (power output) during the initial sprint efforts, as well as incur minimal performance loss in subsequent efforts.1 Performance during RS exercise is limited predominantly by two factors: (1) the ability to match ATP resynthesis rate to utilisation rate and (2) altered extracellular and intracellular ion concentrations. After a single maximal 6 s cycle sprint, muscle phosphocreatine (PCr) is decreased to 35–55% resting level and only recovers to 69% of the initial resting level after 30 s recovery.2 After repeated cycle sprints: 5 and 10×6 s cycle sprints with 30 s recovery intervals, PCr levels are only 27% and 16% resting level, respectively.2 ,3 The resynthesis of PCr is important for performance as following 10×6 s sprints, PCr resynthesis is correlated with total work performed during a further bout after a 5 min rest period.4 In addition, non-oxidative glycolytic contribution to ATP resynthesis declines over successive sprints, seemingly due to lower glycogenolysis and increased activation of pyruvate dehydrogenase complex such that a greater proportion of pyruvate is oxidised.2 With successive sprints therefore there is a decline in ATP resynthesis from PCr hydrolysis and non-oxidative glycolysis, with increasing oxidative contribution resulting in slower ATP resynthesis and deterioration in work capacity/performance. In addition, increased extracellular K+ and H+ may perturb generation and conduction of sarcolemmal action potentials and the release of Ca2+ from the sarcoplasmic reticulum into the myoplasm, thus inducing peripheral neuromuscular fatigue.5 Central fatigue has also been observed after repeated sprint exercise with an increased twitch force elicited by electrical stimulation of the femoral nerve after repeated sprints,6 ,7 indicating insufficient or inefficient central neural drive. The central nervous system is directly sensitive to alterations in oxygen delivery8 and afferent signals from the muscles can also alter central neural function.9 During RS in normoxia cerebral oxygenation and power output decrease in parallel.10 These changes are exacerbated in hypoxia and there is an increased supraspinal contribution to fatigue.11–13 A recent review of optimal training practices to enhance RSA concluded that, due to these multiple dependencies of RSA, a combination of high intensity interval, repeated sprint and strength/power training is required.14
RS training (typically 6–15 repetitions of 6 s sprints) 3–5 times/week for 4 weeks has been shown to improve peak and mean speed by up to 6%,15 ,16 possibly due to enhancing muscle oxygen extraction,17 greater activation of type II muscle fibres3 and altered signalling related to mitochondrial biogenesis.18 Training, particularly high-intensity training, in hypoxia has been shown to augment peripheral adaptations to training, such as improved oxidative enzyme activity,19 length density and mitochondrial volume density,20–22 as well as increased expression of hypoxia inducible factor-1α and downstream genes related to oxygen transport and utilisation.20 Hypoxic training appears to possess the ability to develop many of the components that contribute to RSA, and there is some direct evidence that hypoxic training can enhance sprint performance: improved mean repeat sprint power in kayakers23 and anaerobic performance in a maximal 30 s cycle in endurance athletes,24 potentially due to improved oxygen transport and increased glycolytic activity.25 ,26 However, until today only one published study has adopted a repeated sprint training protocol (cycling) in a hypoxic environment (0.14 FiO2) and found increased expression of genes relating to oxygen transport and glycolysis as well as increased exercise capacity when compared to normoxic training.27 Selection of an appropriate hypoxic dose will be critical to maximise training adaptation since if too severe, hypoxic exposure will also impair repeated sprint speed and exacerbate fatigue. This is likely to compromise training quality and hence counteract the possible benefits to be derived from the greater physiological load. We recently found that RS running (10×6 s sprints) at 0.13 FiO2 increased the physiological responses but did not exacerbate the speed decrement associated with hypoxic training.28 The purpose of the present study was to determine whether 12 sessions of repeated running sprint training in 13% FiO2 improved measures of sports specific endurance performance to a greater extent than the equivalent training in normoxia.
Methods
Type of study
Well-trained academy rugby league and rugby union academy players were randomised to complete 4 weeks of hypoxic or normoxic repeated sprint training during the preseason period.
Selection of participants
A total of 42 well-trained academy rugby union and rugby league players were recruited to take part in the study (18.4±1.5 years, 183.0±6.6 cm, 88.1±8.9 kg), which was conducted in accordance with the Declaration of Helsinki 2008. Participants completed a health questionnaire and stated that they had no previous acute mountain sickness, ascent >3000 m in the past 3 months, musculoskeletal injury in the past 6 months or medication during the trial. All participants completed a written informed consent document. Of the 42 participants, 30 completed the training protocol, due to missed training sessions (n=8) and injury (n=4). All RS training replaced field based speed sessions.
Experimental procedure
Participants were split into two groups matched for body size and initial fitness levels, in a single-blind, placebo-controlled design. On the coaches’ request all participants were told they were in the experimental group. Participants completed 4 weeks of RS training on a non-motorised treadmill. Pretraining and post-training, treadmill speed, oxygen consumption (VO2), carbondioxide consumption (VCO2), VE (minute ventilation), respiratory exchange rate (RER) cerebral and quadriceps deoxygenated haemoglobin (HHb), heart rate (HR) and SaO2 were measured during a normoxic RS bout on a non-motorised treadmill and participants also completed field performance tests.
Testing protocol
Familiarisation occurred on three consecutive days 48 h before the first testing day and consisted of participants completing the RS protocol outside and then on the non-motorised treadmill. Participants were instructed to refrain from caffeine or alcohol for 48 h prior to all testing and on arrival to pretesting all participants completed a standardised 15 min sports specific warm up including dynamic stretches and acceleration drills. Participants completed a 20 m maximum sprint, collecting data at 5, 10 and 20 m using lightgate timing devices (Smartspeed, Fusion Sport Ltd, Australia). This was repeated three times with a 3 min rest between repetitions. Participants then completed an RSA test, in which ten 20-m sprints were completed with 30 s rest intervals. Time for each repetition was recorded and totalled, while speed decrement was calculated using the equation of Girard et al29 Finally all participants completed a 20-m shuttle test (Yo-Yo Intermittent Recovery test Level 1 (Yo-Yo IR1 test), BangsboSport, Denmark).
After 48 h rest, participants arrived at the laboratory and completed the standardised warm up. Near infrared-spectroscopy (NIRS) optodes (NIRO 200, Hamamatsu Photonics KK, Japan) were applied to the skin surface above m. vastus lateralis of the left leg and above the left eye to observe the changes in muscle and cerebral tissue deoxygenation (HHb). The [HHb] signals for cerebrum and quadriceps were zeroed after 5 min quiet standing. An HR belt (Suunto Memory Belt, Suunto, Finland) was secured around the chest and a pulse oximeter (Nonin’s 3100 WristOx, Minnesota, USA) was placed on the index finger of the right hand. Finally a face mask was fitted to record the respiratory responses to the exercise protocol through a gas analyser system (MetaMax 3B; Cortex Biophysik, Leipzig, Germany). The RS test was completed in normoxia and consisted of 10, 6 s sprints on a non-motorised treadmill (Woodway Curve, Woodway, Germany) interspersed with 30 s recovery followed by 5 min static recovery. During the test, speed was monitored using a bespoke infrared reflective system and data-logging device (PicoLog 1012, Pico Technology, UK). Capillary blood samples were taken from the left ear lobe pretesting, immediately postcompletion and 5 min after sprint completion, then analysed for blood lactate (BLa) content using a hand-held LactatePro analyser. Strong verbal encouragement was given during all repetitions throughout the testing. Data were analysed off-line using custom written scripts developed in Spike2 software (CED, Cambridge, UK).
Training protocol
Participants completed training at the same time each day in place of RS activity during field based training. Similar to the testing procedure participants completed the standardised warm up and once on the treadmill attached a face mask that was connected to a portable hypoxic generator (Everest Summit II Hypoxic Generator, Hypoxico Inc, New York, USA). Participants were either exposed to hypoxic gas (13% FiO2) or a placebo normoxic gas (21% FiO2) throughout the entire protocol. Each session consisted of the same RS procedure as during testing.
Data acquisition—NIRS
A modified form of the Beer-Lambert law is used to calculate micromolar changes in tissue deoxyhaemoglobin concentration [HHb] across time based on the difference between the optical densities of the emitted and reflected NIR light with two wavelengths (763 and 855 nm). The temporal changes in [HHb] are dependent on O2 extraction dynamics and are considered relatively independent of blood volume changes in the field of NIRS interrogation.30 Thus, we used the changes in [HHb] prior to each sprint to estimate the differences in intramuscular and cerebral deoxygenation status induced by RS training in hypoxia and normoxia.
Data acquisition—pulmonary gas exchange
Breath-by-breath pulmonary gas exchange data were recorded throughout the RS protocol using a portable gas exchange system (MetaMax 3B; Cortex Biophysik, Leipzig, Germany). The area under the curve of the time by VO2 and ventilation (VE) traces were calculated for the different periods of the protocol: during sprints, during the recovery between sprints, during the 5 min recovery period as well as total areas under the curve for the entire protocol.
Statistical analysis
Data are presented as mean±SD. The data set for each variable was tested for normal distribution with the Kolmogorov-Smirnov statistic. Speed, SaO2, HR, VO2, VCO2, VE and BLa data were analysed by two-way repeated measures ANOVA (time×condition). Presprint HHb for cerebral and quadriceps were analysed by three-way repeated measures ANOVA (time×condition×sprints). Post hoc paired sample t tests, corrected for multiple comparisons using the Holm-Sidak step down procedure, were used to locate the specific site of any interaction effect identified. Data were analysed using SPSS V.19.0 for Windows (SPSS, Chicago, Illinois, USA). The level of statistical significance was set at p<0.05.
Results
Field testing
Training significantly increased distance covered in the Yo-Yo IR1 test (table 1) and gains were significantly greater in the hypoxic (33±12%) than the normoxic group (14±10%, p=0.002). Five metre sprint performance and total time taken in the 20 m RS test improved after training (p<0.05), but there were no significant differences between the hypoxic and normoxic training groups (table 1). There were no significant changes to 10 or 20 m sprint performance or speed decrement in the 20 m RSA test (prehypoxic 4.0±3.0% and posthypoxic 2.7±1.6% vs prenormoxic 5.1±3.9 and postnormoxic 3.7±2.1%, time effect p=0.317).
Field testing performed in normoxia before (PRE) and after (POST) 4 weeks of training in either hypoxia (HYP) or normoxia (NRM) (n=30)
Physiological measures during RSA laboratory test
VO2, VCO2, VE, SaO2, HR and BLa
There was a tendency for a greater increase in total oxygen consumed during the test after hypoxic than normoxic training (hypoxic 6.9±9%, normoxic −0.3±8.8%, independent t test, p=0.06; table 2). There was a significant increase in total VCO2 for both groups (hypoxic 8.1±8.9%, normoxic 5.6±9.5%, p<0.05), but no significant difference between the groups (table 2). There was no significant change in total VE, SaO2, peak HR or capillary BLa concentrations after hypoxic or normoxic training and no difference between groups (table 2).
Physiological parameters of RSA test on non-motorised treadmill performed in normoxia before (PRE) and after (POST) 4 weeks of training in either hypoxia (HYP) or normoxia (NRM) (n=26)
Cerebral and quadriceps deoxygenation
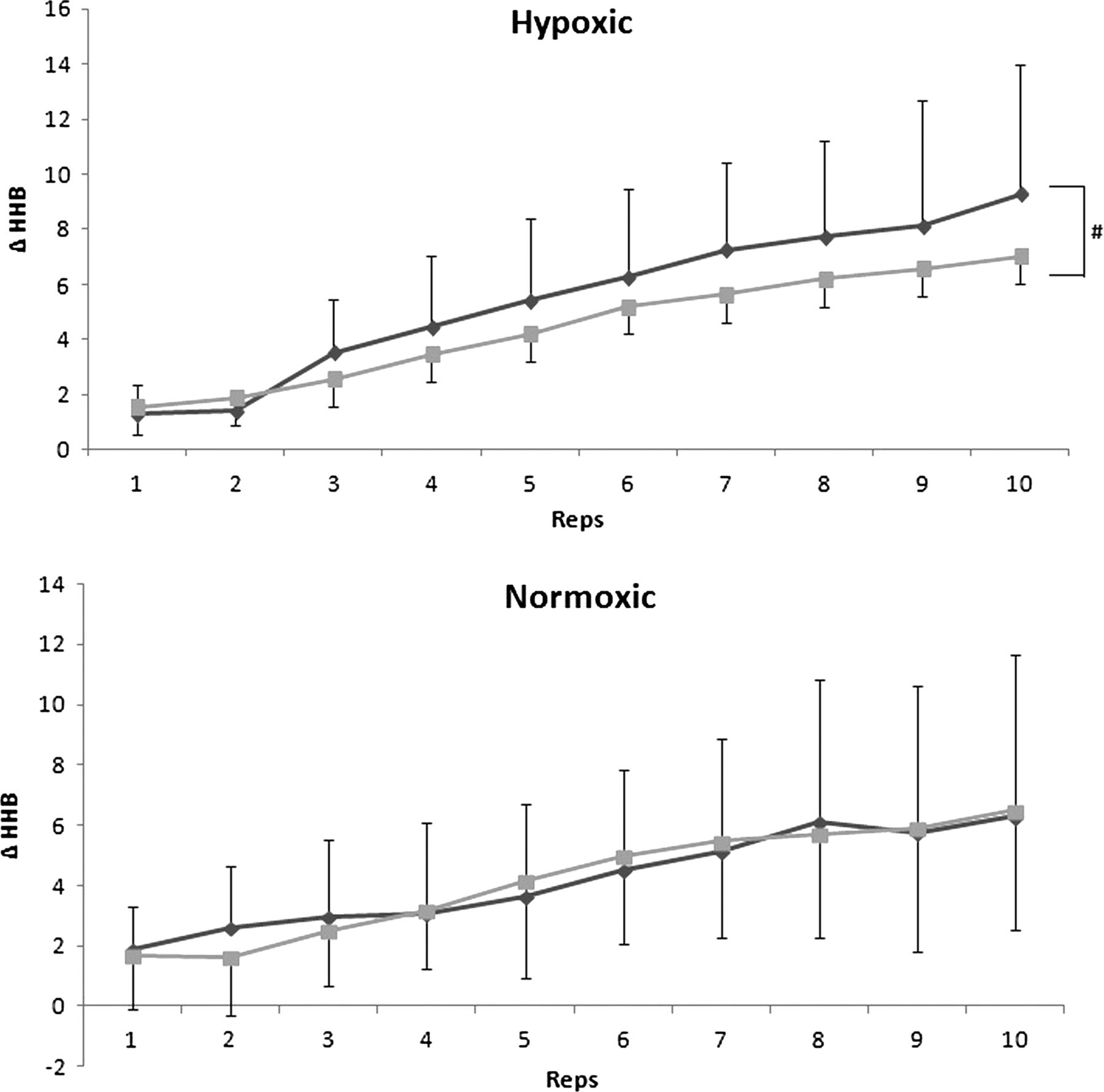
Cerebral deoxygenation (HHb presprint) tended to be lower across sprints after hypoxic training, but there was no change in response after normoxic training (time×condition×sprints, p=0.09; figure 1). Quadriceps deoxygenation during the repeated all-out sprints did not change as a result of training (p=0.948; figure 2).

Change in cerebral deoxygenation (HHb) prior to each sprint repetition during pretesting (PRE) and post-testing (POST; n=26), # denotes time×condition×sprints p=0.09  .
.

{kind=link}
{kind=link}
Change in quadriceps deoxygenation (HHb) prior to each sprint repetition during pretesting (PRE) and post-testing (POST; n=26)  .
.
Distance covered and speed decrement
Total distance covered throughout the treadmill RSA test improved after training in both groups (p=0.02) but this was not statistically significant between the groups (p=0.263). Speed decrement during the RSA test improved after training in both groups (p=0.059) and improved to a greater extent in the hypoxic (27±37%) than in the normoxic group although non-significantly due to variability in the data (1±51%; p=0.122; table 2).
Discussion
Four weeks of RS training in normobaric hypoxia resulted in significantly greater improvements in the Yo-Yo IR test than equivalent training conducted in normoxia. Participants also tended to cover more distance with a smaller speed decrement and consume a larger volume of oxygen during the 6-s RS test after hypoxic training indicating greater total energy expenditure and work performed (table 2). This performance improvement was perhaps possible as a consequence of the lesser cerebral deoxygenation incurred during RS after hypoxic training, since cerebral deoxygenation has been related to central fatigue.12
The hypoxic group had a twofold greater increase in distance covered in the Yo-Yo test (33%) compared to the normoxic group (14%) after 4 weeks of training (12×RS sessions), which compares favourably to the training induced improvements observed in previous studies (7 weeks RS vs interval training +28 vs +13%31; 10×RS training sessions, +8%18). The Yo-Yo IR test is correlated with physical performance and the amount of high-intensity running in soccer,32 basketball,33 rugby league34 and handball.35 Hence the magnitude of Yo-Yo IR1 performance improvement induced by hypoxic RS training is likely to translate to improved intermittent sport performance. Yo-Yo performance is 9.5% higher in elite (international honours) than moderate elite (professional leagues) football players, which correlates with a 10% increase in distance covered at high intensities (200 m) during a game.32 On this basis, the large gains in Yo-Yo performance in the hypoxic group in the present study would translate to an extra 600 m distance covered at a high intensity in a match. To put into perspective for our participants, elite rugby players have been shown to achieve a significantly higher distance covered in the Yo-Yo IR1 than subelite players (1660 m vs 1560 m).34 During our pretesting, three players in the normoxic group and one in the hypoxic group were in this elite category, while after hypoxic training seven players moved into the elite category compared to only two players in the normoxic group. This demonstrates that the short term (4 weeks) use of hypoxic RS training is able to elicit a greater gain in intermittent sports specific endurance than 7 weeks of traditional RS training.31 Therefore, this is a highly practical and efficient preseason training technique.
In contrast to the improvement in Yo-Yo IR1 performance which tests the athlete's ability to repeatedly perform predominantly aerobic high-intensity work,32 single maximal sprint performance over 5, 10 or 20 m was not enhanced by hypoxic versus normoxic RS training. In parallel with the enhanced oxygen consumption during the RS protocol after hypoxic training, this suggests that oxidative rather than non-oxidative metabolism was enhanced by hypoxic RS training. This conclusion is supported by the RS ability field test that showed no significant improvement in either group after the training. The field test involved 20 m RS whereas 6 s sprints were performed on the treadmill equating to approximately 40 m. The absence of performance improvement in the shorter test, which is more reliant on anaerobic energy systems,1 suggests that there is little adaptation of the anaerobic systems in response to hypoxic RS in intermittent athletes. This may have been because the training method was one set of 10×6 s repetitions. Previous work in which glycolytic activity was improved, used three sets of 5×10 s sprints with adequate rest to ensure larger power outputs.27 However, this protocol then failed to induce improvement in the 3 min all out test in cyclists27 suggesting limited improvement in oxidative capacity. This highlights the specificity of the adaptations induced to the training protocol utilised (work and rest durations and work:rest ratio) and hence the specific metabolic demands of the training.
Total O2 consumption during the 6 s RS test tended to increase after hypoxic training (Independent t test, p=0.06). This presumably reflects a greater volume of work performed in the hypoxic group, certainly total distance covered tended to be greater after hypoxic training (table 2). The rapid component of excess postexercise oxygen consumption (EPOC) is thought to reflect the oxygen cost of PCr resynthesis,36 hence the increased EPOC after hypoxic training may indicate increased PCr turnover during the sprints. Postexercise capillary BLa concentration was similar across trials suggesting no change in non-oxidative glycolysis post-training, although increased lactate removal through non-exercising muscles or respiratory muscles37 cannot be excluded with the present data. However, without muscle biopsy and/or 31P-MRS data we are not able to determine the metabolic effects of hypoxic RS training in the present study.
The ameliorated cerebral deoxygenation after hypoxic RS training in the present study may allow maintained central drive and contribute to an improved work capacity during posthypoxic training RS exercise. Central fatigue contributes to the deterioration in performance during RS training as evidenced by reduced voluntary activation.6 This may relate to reduced cerebral oxygenation, since studies in hypoxia have demonstrated that diminished cerebral oxygen availability is associated with decreased central drive and fatigue. Specifically during RS exercise, decreased cerebral oxygenation was associated with decreased work capacity.38 ,39
What are the new findings?
-
Well-trained academy rugby players performing repeated sprint training in hypoxia achieved twofold greater improvements in their capacity to perform repeated aerobic high intensity work.
-
Performance gains are evident in the short term (4 weeks), a period similar to a preseason training block.
-
Further work is required to identify the mechanisms of adaptation.
How might it impact on clinical practice in the future?
-
Athletes and teams in intermittent sports could confidently choose to implement repeated sprint training sessions in hypoxia to improve sports specific endurance in a relatively short period of time.
References
Footnotes
-
Contributors All of the authors were involved in the conception, design, analysis, interpretation of results and drafting of the article.
-
Funding Technology Strategy Board Knowledge Transfer Partnership with London South Bank University and The Altitude Centre Ltd, Part funded by Altitude Centre and Knowledge Transfer Board (Grant number KTP007591). Funded time of research associate and academic supervisors and supplied equipment.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval London South Bank University.
-
Provenance and peer review Not commissioned; externally peer reviewed.