Article Text

Abstract
The Female Athlete Triad is a medical condition often observed in physically active girls and women, and involves three components: (1) low energy availability with or without disordered eating, (2) menstrual dysfunction and (3) low bone mineral density. Female athletes often present with one or more of the three Triad components, and an early intervention is essential to prevent its progression to serious endpoints that include clinical eating disorders, amenorrhoea and osteoporosis. This consensus statement represents a set of recommendations developed following the 1st (San Francisco, California, USA) and 2nd (Indianapolis, Indiana, USA) International Symposia on the Female Athlete Triad. It is intended to provide clinical guidelines for physicians, athletic trainers and other healthcare providers for the screening, diagnosis and treatment of the Female Athlete Triad and to provide clear recommendations for return to play. The 2014 Female Athlete Triad Coalition Consensus Statement on Treatment and Return to Play of the Female Athlete Triad expert panel has proposed a risk stratification point system that takes into account magnitude of risk to assist the physician in decision-making regarding sport participation, clearance and return to play. Guidelines are offered for clearance categories, management by a multidisciplinary team and implementation of treatment contracts. This consensus paper has been endorsed by the Female Athlete Triad Coalition, an International Consortium of leading Triad researchers, physicians and other healthcare professionals, the American College of Sports Medicine and the American Medical Society for Sports Medicine.
- Women in Sport
Statistics from Altmetric.com
Introduction
This consensus statement is the first of its kind and represents a set of recommendations developed following the 1st (San Francisco, California, USA) and 2nd (Indianapolis, Indiana, USA) International Consensus Meetings on the Female Athlete Triad (Triad). It is intended to provide clinical guidelines for physicians, athletic trainers and other healthcare providers for the treatment of the Triad and to provide clear recommendations for return to play. The Consensus recommendations herein were developed using a consensus-based approach similar to that utilised by the International Consensus Statement on Concussion.1 This consensus statement will serve as a supplement to the American College of Sports Medicine (ACSM) revised position stand on the Triad published in 2007. The 2007 position stand provided the scientific evidence documenting the existence and causes of the Triad.2 Practical information for athletes, coaches, parents and a list of resources and helpful information on the Triad can be readily viewed on the Female Athlete Triad Coalition website at http://www.femaleathletetriad.org. This consensus paper has been endorsed by The Female Athlete Triad Coalition, an International Consortium of leading Triad researchers, physicians and other healthcare professionals, the American College of Sports Medicine and the American Medical Society for Sports Medicine.
While agreement exists concerning the primary guidelines and recommendations communicated in this document, the authors acknowledge that the underlying levels of scientific evidence regarding some elements of the Triad, particularly related to treatment strategies, are still evolving. The treatment guidelines and return-to-play recommendations proposed herein are based on the published literature available to date, with consensus from the international team of experts convened at the two meetings. As such, management and return-to-play decisions should be based on informed clinical judgement keeping in mind individual risk factors and concerns as described herein.
Definition of the Female Athlete Triad Model
The Triad is a medical condition often observed in physically active girls and women, and involves any one of the three components: (1) low energy availability (EA) with or without disordered eating (DE), (2) menstrual dysfunction and (3) low bone mineral density (BMD)2 (see figure 1). Female athletes often present with one or more of the three Triad components, and an early intervention is essential to prevent its progression to serious endpoints that include clinical eating disorders (EDs), amenorrhoea and osteoporosis.2

Spectra of the Female Athlete Triad. The three inter-related components of the Female Athlete Triad are energy availability, menstrual status and bone health. Energy availability directly affects menstrual status, and in turn, energy availability and menstrual status directly influence bone health. Optimal health is indicated by optimal energy availability, eumenorrhoea and optimal bone health, whereas, at the other end of the spectrum, the most severe presentation of the Female Athlete Triad is characterised by low energy availability with or without an eating disorder, functional hypothalamic amenorrhoea and osteoporosis. An athlete's condition moves along each spectrum at different rates depending on her diet and exercise behaviours. BMD, bone mineral density.2 Adapted with permission from Lippincott Williams and Wilkins/Wolters Kluwer Health: Medicine and Science in Sport and Exercise.2
In 1997, the Task Force on Women's Issues of ACSM published the first Triad position stand which described a syndrome of three distinct but inter-related conditions: DE, amenorrhoea and osteoporosis.3 Subsequent cross-sectional studies defined the Triad based on critical endpoints for each of the three Triad components to include ED, amenorrhoea and osteoporosis. The components of the Triad are known to be inter-related since energy deficiency associated with DE plays a causal role in the development of menstrual disturbances,4–6 and an energy deficiency and a hypoestrogenic environment associated with amenorrhoea play a causal role in low BMD.7–10
In studies conducted after the publication of the 1997 Triad position stand, investigators identified negative health consequences of the Triad associated with subclinical/less severe conditions than the aforementioned clinical endpoints. Reports of a high prevalence of subclinical menstrual disturbances, including luteal phase defects and anovulatory cycles, were observed in athletes and recreationally active women.11 ,12 Investigators have documented mild-to-moderate low BMD among athletes with oligomenorrhoea and subclinical menstrual disturbances (ie, anovulation and luteal phase defects).13 ,14 Other investigators have identified that a delay in menarche,15 ,16 a history of oligomenorrhoea and amenorrhoea17–19 and/or low BMD (not just osteoporosis) were significant risk factors for stress fractures and bone stress injury in athletes17 ,18 ,20 and female military recruits.21 ,22 Findings from controlled laboratory studies indicated that low EA caused hormone disruptions characterised by suppressed metabolic and reproductive hormones, suppressed bone formation and increased bone resorption.9 ,23–25 A causal relationship for the induction of menstrual disorders associated with low EA was carefully documented in the literature.5 ,26 ,27 The reversal of amenorrhoea was also demonstrated to be related to EA.5 ,27 Therefore, to better reflect the most recent research, as well as to more comprehensively identify athletes at risk for developing negative health consequences, there was a clear need to revise the 1997 definition of the Triad.
In 2007, the Triad was redefined as a syndrome of low EA with or without DE, functional hypothalamic amenorrhoea (FHA) and osteoporosis.2 EA is defined conceptually and behaviourally as the amount of dietary energy remaining after exercise training for all other physiological functions each day.28 The new Triad model represented each component as the pathological endpoint of one of the three inter-related spectrums ranging from a healthy endpoint to subclinical and clinical conditions.2 At the ‘healthy’ end of the continuum, each Triad component is optimised, that is, EA meets total energy expenditure, reproductive and bone health needs; ovulatory menstrual cycles are maintained and bone mass is normal.2 At the ‘unhealthy’ end of the continuum, each Triad component presents the clinical endpoints of the syndrome, including low EA with or without DE, FHA and osteoporosis.2
The goal in presenting Triad conditions along a spectrum was to highlight the importance of recognising athletes who exhibit subclinical abnormalities and thus allow for early intervention. The panel supports the notion that prevention and early intervention remains the key to avoid the more serious clinical endpoints of the Triad (ie, ED, amenorrhoea or osteoporosis). Furthermore, given the recent focus on subclinical menstrual disturbances and bone-related concerns, the panel agreed that the 2007 presentation of the Triad model as a spectrum is most appropriate and most useful for designing treatment and return-to-play guidelines.
Health consequences associated with the Triad
Why is the Triad harmful to an athlete's health?
Chronic low EA can have significant effects on health and physical performance, particularly when a clinical ED is present.29 Low EA plays a causal role in the induction of exercise-associated menstrual disturbances.5 ,30 Hypoestrogenemia associated with prolonged reproductive suppression can negatively impact musculoskeletal and cardiovascular health.7 ,31 ,32 Low EA can also have negative musculoskeletal effects independent of hypoestrogenism.7 ,8 Bone stress injuries, including the spectrum of stress reactions and stress fractures, are more common in female athletes with menstrual irregularities and/or low BMD,15–20 as well as female military recruits.21 ,22 Bone stress injuries also sideline female athletes and reduce competitive performance. Poorer sport performance has been documented in junior elite swimmers who exhibited ovarian suppression and evidence of energy deficiency when compared with their normally cycling counterparts.33 Other medical complications of Triad disorders can extend to the endocrine, gastrointestinal, renal and neuropsychiatric systems.2 ,34–36 A complete discussion of the health consequences of the Triad is beyond the scope of this paper and can be found elsewhere.2 ,37
Screening, risk stratification and diagnosis of the Triad
What are the best tools to screen for the Triad?
Early detection of athletes at risk is critical to prevent the Triad. Screening for the Triad should be undertaken as part of the Pre-Participation Physical Evaluation (PPE).38–40 The PPE should include questions that address all aspects of the Triad spectrums. The current standard screening PPE form, endorsed jointly by six US medical societies,41 includes nine questions related to the Triad. Likewise, the International Olympic Committee (IOC)-endorsed Periodic Health Examination40 proposes eight questions to screen girls and young women for the Triad.
Although there is limited evidence related to the efficacy of screening questions,42 the Consensus Panel recommended that female athletes undergo annual screening with the Triad-specific self-report questionnaire displayed in box 1, followed by a more in-depth evaluation if the athlete has, or is at risk for, any Triad component. While such screening is most typically completed at the collegiate level, the panel recommended screening for younger athletes (high school age) as well.43 ,44 A major point that the panel emphasised is that existence of any one Triad component should prompt more thorough investigation for the others. Screening and early intervention in adolescent females for components of the Triad are especially important when one considers that 90% of peak bone mass is attained by 18 years of age,45 thereby providing a window of opportunity for optimising bone health.
Triad Consensus Panel Screening Questions*
-
Have you ever had a menstrual period?
-
How old were you when you had your first menstrual period?
-
When was your most recent menstrual period?
-
How many periods have you had in the past 12 months?
-
Are you presently taking any female hormones (oestrogen, progesterone, birth control pills)?
-
Do you worry about your weight?
-
Are you trying to or has anyone recommended that you gain or lose weight?
-
Are you on a special diet or do you avoid certain types of foods or food groups?
-
Have you ever had an eating disorder?
-
Have you ever had a stress fracture?
-
Have you ever been told you have low bone density (osteopenia or osteoporosis)?
*The Triad Consensus Panel recommends asking these screening questions at the time of the sport preparticipation evaluation.
What are the most important risk factors to screen for?
The Panel stated that the risk factors that should be assessed for the Triad include: (1) history of menstrual irregularities and amenorrhoea2 ,46; (2) history of stress fractures2 ,46; (3) history of critical comments about eating or weight from parent, coach or teammate47 ,48; (4) a history of depression49–51; (5) a history of dieting51 ,52; (6) personality factors (such as perfectionism and obsessiveness)53–55; (7) pressure to lose weight and/or frequent weight cycling52; (8) early start of sport-specific training52; (9) overtraining52; (10) recurrent and non-healing injuries56 and (11) inappropriate coaching behaviour.52 ,54 Physical examination signs such as low body mass index (BMI), weight loss, orthostatic hypotension, lanugo, hypercarotenaemia, or other signs of an ED, such as parotid gland swelling and callus on the proximal interphalangeal joints (also known as Russell's sign), should also prompt further evaluation. Obtaining an accurate menstrual history is important, starting from age of menarche to the current and the past menstrual patterns, noting months of consecutive missed menses and the number of menses per year since menarche.41 ,57 Evaluation of secondary amenorrhoea in girls can begin after 3 months or more of missed menses.57 A medication history should be obtained, including medications which may affect menstruation and/or BMD, such as oral contraceptive pills or other contraceptive agents, such as depot medroxyprogesterone acetate.58 A history of physician diagnosed bone stress injuries and other fracture history should be noted,41 as well as a family history of ED, osteoporosis59 and/or fractures.
Diagnosis of the Triad
How are Triad conditions diagnosed?
Following screening, accurate diagnosis of any of the Triad disorders is dependent on a thorough evaluation of the athlete by the physician and other members of an experienced multidisciplinary healthcare team. Members of the multidisciplinary team should include a physician, a sports dietitian (a registered dietitian, who preferably is a board certified specialist in sports dietetics)60 ,61and a mental health professional, if the athlete has DE or a clinical ED. Other members of the team may include an exercise physiologist, certified athletic trainer and medical consultants.
The Consensus Panel agreed that essential to the process of screening, evaluation, diagnosis and treatment is the athlete's honesty and willingness to participate in each of these steps. Each member of the multidisciplinary team must develop a therapeutic alliance with the athlete. The process of engagement and active participation in treatment is often ongoing, reflecting the challenges of restoring adequate EA. The panel emphasised that written policies regarding screening, evaluation and treatment of the Triad need to be reviewed with athletes and their parents, and supported by coaches and administrators.
How is low EA diagnosed? The Panel emphasised that low EA cannot be diagnosed by estimating energy balance because athletes who have been in a state of negative energy balance may experience a suppression of physiological functions that restores energy balance and weight stability.2 Weight stability has been reported in amenorrhoeic athletes.62–65 Thus, an athlete could be in a state of energy balance but also in a state of low EA at the same time, and a stable body weight should not be used as an indicator of adequate EA.
As a first pass, overt signs of low EA can be indicated by low energy stores such as a BMI <17.5 kg/m2 or in adolescents <85% of expected body weight. In adolescents, absolute BMI cut-offs should not be used. The BMI percentile method for calculating estimated body weight examines an adolescent's weight in relation to the 50th BMI percentile (which is their expected body weight).66 Deviations for this point are used as an indicator of medical stability to set a target weight and to assess progress in adolescents with DE and ED.66 BMI percentiles adjusted for age and gender are recommended until age 20 by the Centers for Disease Control and Prevention (http://www.cdc.gov/growcharts). When body weight is not particularly low, more detailed information regarding food intake and energy expenditure is necessary to diagnose low EA. Other markers of low EA in the absence of DE and recent weight loss that should be explored include physiological signs of adaptation to chronic energy deficiency, such as reduced resting metabolic rate (RMR),4 ,67 low triiodothyronine (low T3)4 ,67 and a ratio of measured RMR/predicted RMR less than 0.90.7 ,68–70
It is important to note that methods for assessing EA, dietary intake and energy expenditure are improving but are imprecise. An experienced sports dietitian or an exercise physiologist can help provide expertise on completing these assessments. A particular index of daily EA is defined as energy intake (kcal) minus exercise energy expenditure (kcals) divided by kilograms of fat-free mass (FFM) or lean body mass.28 This index has been significantly associated with changes in reproductive6 ,24 and metabolic hormone concentrations and markers of bone formation and resorption9 that occur in controlled laboratory experiments where EA is manipulated using varying combinations of reductions in food intake and increases in exercise energy expenditure in women. From these short-term experiments, a threshold below which detrimental physiological changes in reproductive function, metabolism and bone occur has been identified as 30 kcal/kg of FFM/day.6 The Panel noted that outside the laboratory, determination of EA using this index is more difficult and is dependent on less precise measures of exercise energy expenditure, dietary energy intake and body composition (weight and per cent fat). Strategies to estimate dietary intake include 3-day, 4-day and 7-day dietary logs, 24 h dietary recall and food-frequency questionnaires.71 Regardless of the method chosen, accurate assessment of dietary intake can be challenging due to a number of factors such as under-reporting of intake, modified intake during the period of reporting and imprecise recording of portion sizes.71 Ideally, athletes thought to be at risk for nutritional deficiencies should undergo a comprehensive nutrition assessment by a registered sports dietitian.61 Actual estimates of energy expenditure can be accomplished using heart rate monitors and accelerometers,28 but practical estimates of exercise energy expenditure are also available, and are dependent on self-report. There are numerous web-based calculators of exercise energy expenditure; however, the Panel recommends that the 2011 Compendium of Physical Activities be used to calculate exercise energy expenditure, whereby kilocalories of energy expenditure=metabolic equivalent of task × weight in kilograms × duration of activity in hours.72 All methods of estimating energy expenditure have an error associated with them, and any directional bias needs to be considered on an individual basis.73 The third component of the EA equation is kilograms of FFM, which is obtained from measurement of body weight in kilograms, and from an estimate of body fatness. Various methods can be used to estimate body fat. Dual-energy X-ray absorptiometry (DXA) is a precise method and widely available74; other clinically accessible methods commonly used among athletes include air-displacement plethysmography, skin fold measurements and bioelectrical impedance.75 Having gathered the aforementioned data, one can access the EA Calculator provided on the Female Athlete Triad Coalition website (http://www.femaleathletetriad.org/calculators/) to estimate EA. Ideally, physically active women should aim for at least 45 kcal/kg of FFM/day of energy intake to ensure adequate EA for all physiological functions.2 ,28
How is amenorrhoea diagnosed? The Panel explained that athletes and physically active women presenting with primary or secondary amenorrhoea require evaluation to rule out pregnancy and endocrinopathies since no single blood test can confirm a diagnosis. The diagnosis of FHA in athletes secondary to low EA is a diagnosis of exclusion. An algorithm, modified from the Jameson and De Groot textbook of endocrinology76 for the diagnosis of primary/secondary amenorrhoea can be viewed in figure 2. Endocrinopathies that must be ruled out include (1) thyroid dysfunction, (2) hyperprolactinaemia, (3) primary ovarian insufficiency, (4) hypothalamic and pituitary disorders (genetic or acquired), (5) hyperandrogenic conditions including polycystic ovary syndrome, virilising ovarian tumours, adrenal tumours, non-classic congenital adrenal hyperplasia and Cushing's syndrome.77 ,78 Outflow tract obstruction is important to rule out in patients with primary amenorrhoea. The most common causes of amenorrhoea are usually identified following a thorough medical history, physical examination, a pregnancy test, as well as evaluation of thyroid stimulating hormone, follicle stimulating hormone and prolactin, to assess for thyroid disease, primary ovarian insufficiency and hyperprolactinaemia. A serum oestradiol and/or a progesterone challenge test (medroxyprogesterone acetate 10 mg for 10 days) may be useful to assess the degree of hypoestrogenism. If there is physical evidence of androgen excess (ie, hirsutism, acne and androgenic alopecia), additional laboratory testing may include total and free testosterone, and dehydroepiandrosterone and its sulfate (DHEA/S). An early morning 17-hydroxyprogesterone may be obtained in those with hyperandrogenism to assess for non-classic 21-hydroxylase deficiency (the most common cause of congenital adrenal hyperplasia) on initial or follow-up testing. A pelvic ultrasound may be obtained in those with clinical or biochemical hyperandrogenism to confirm polycystic ovaries or to rule out virilising ovarian tumours.77 ,79 The primary care physician should refer to or consult with an endocrinologist for endocrine disorders they are not experienced in diagnosing or treating.

Amenorrhoea algorithm. Recommended clinical evaluation of an athlete with primary or secondary amenorrhoea, or prolonged oligomenorrhoea, includes a history and physical examination, initial and follow-up laboratory testing and diagnosis by a physician. Referral or consultation with endocrinology is recommended if the diagnosing physician is not experienced with treatment of functional hypothalamic amenorrhoea or other aetiologies of amenorrhoea. DHEA/S, dehydroepiandrosterone sulfate; FHA, functional hypothalamic amenorrhoea; FSH, follicle-stimulating hormone; hCG, human chorionic gonadotropin; LH, luteinizing hormone; PCOS, polycystic ovarian syndrome; TSH, thyroid-stimulating hormone. Modified from Illingworth76.
How is low BMD diagnosed? The Panel has utilised the definitions published by the International Society of Clinical Densitometry (ISCD) for low BMD and osteoporosis in children and adolescents (see box 2) and for premenopausal women (see box 3)80 as well as ACSM suggested criteria for female athletes involved in regular weight-bearing sports.2 Criteria are described below for who and what site should be considered for a DXA scan and how often DXA should be performed.
Definition of low bone mineral density (BMD) and osteoporosis in children and adolescents (ages 5–19)
The diagnosis of osteoporosis in children and adolescents requires the presence of both a clinically significant fracture history AND low bone mineral content (BMC) or low BMD
-
A clinically significant fracture history is one or more of the following:
-
Long bone fracture of the lower extremities.
-
Vertebral compression fracture.
-
Two or more long-bone fractures of the upper extremities.
-
-
Low BMC or BMD* is defined as a BMC or areal BMD Z-score that is ≤−2.0, adjusted for age, gender and body size, as appropriate.
Source: Lewiecki et al.80
*American College of Sports Medicine (ACSM) defines low BMC or BMD as a Z-score that is less than −1.0 in female athletes in weight-bearing sports.2
Who should get DXA scans for BMD testing
The Panel agreed that indications for obtaining a DXA scan for BMD testing in an athlete should follow the Triad risk stratification (see Clearance and return to play section) and include the following:
-
≥1 ‘High risk’ Triad risk factor:
-
History of a DSM-V diagnosed ED81
-
BMI ≤17.5 kg/m2, <85% estimated weight, OR recent weight loss of ≥10% in 1 month
-
Menarche ≥16 years of age
-
Current or history of <6 menses over 12 months
-
Two prior stress reactions/fractures, one high-risk stress reaction/fracture (see figure 3), or a low-energy non-traumatic complete fracture18 ,82 ,83
-
Prior Z-score of <–2.0 (after at least 1 year from baseline DXA)
-

Treatment of the Female Athlete Triad. The three components of the Triad recover at different rates with the appropriate treatment. Recovery of energy status is typically observed after days or weeks of increased energy intake and/or decreased energy expenditure. Recovery of menstrual status is typically observed after months of increased energy intake and/or decreased energy expenditure, which improves energy status. Recovery of bone mineral density may not be observed until years after recovery of energy status and menstrual status has been achieved. IGF-1, insulin-like growth factor-1.
OR
-
≥ 2 “Moderate risk” Triad risk factors:
-
Current or history of DE for 6 months or greater
-
BMI between 17.5 and 18.5, <90% estimated weight, OR recent weight loss of 5–10% in 1 month
-
Menarche between ages 15 and 16 years
-
Current or history of 6–8 menses over 12 months
-
One prior stress reaction/fracture
-
Prior Z-score between –1.0 and –2.0 (after at least 1 year interval from baseline DXA)
-
-
In addition, an athlete with a history of ≥1 non-peripheral or ≥2 peripheral long bone traumatic fractures (non-stress) should be considered for DXA testing if there are one or more moderate or high-risk Triad risk factors (see figure 3). This will depend on the likelihood of fracture given the magnitude of the trauma (low or high impact) and age at which the fracture occurred. Athletes on medications for 6 months or greater that may impact bone (such as depot medroxyprogesterone acetate, oral prednisone and others),84 should also be considered for DXA testing.
How often should athletes get DXA testing
The Panel agreed that the frequency of BMD assessment by DXA will depend on the initial BMD and ongoing clinical status of the athlete. We agree with the ISCD 2013 guidelines that repeat DXA screening should be obtained when the expected change in BMD Z-scores equals or exceeds the least significant change.85 Those with definitive indications for DXA testing may require BMD testing every 1–2 years to determine whether there is ongoing bone loss, and to evaluate treatment.
Which sites should be screened with a DXA scan
BMD Z-scores (and not T-scores) should be reported for all children, adolescents and premenopausal women.
-
Adult women ≥20 years
-
Weight-bearing sites (posteroanterior spine, total hip, femoral neck)
-
Non-weight-bearing sites, namely the radius (33%) if weight-bearing sites cannot be assessed for any reason
-
-
Children, adolescents and young women <20 years
-
Posteroanterior lumbar spine bone mineral content (BMC) and areal BMD
-
Whole body less head if possible (otherwise whole body) BMC and areal BMD80
-
Adjust for growth delay (with height or height age) or maturational delay (with bone age)
-
Use paediatric reference data, and when possible, report height-adjusted Z-scores.86
-
Non-pharmacological treatment guidelines for the clinical sequelae associated with the Triad
What evidence exists in support of non-pharmacological treatment strategies?
Documentation of weight gain and restoration of menstrual function following amenorrhoea has been provided by Kopp-Woodroffe et al87 and Dueck et al88 in case studies, in a retrospective analysis of female athletes following a clinical intervention89 and in experiments in female cynomolgus monkeys.5 Studies in anorexic women demonstrate the efficacy of weight gain (and fat mass) for restoration of menses.90–93 In case studies of five amenorrhoeic athletes and recreationally active women in whom energy intake was increased via consumption of a sport nutrition beverage (approximately 360 kcal/day) and exercise training was reduced by 1 day/week for 12–20 weeks, weight gain of 1–3 kg was observed and three of the five women resumed menses.87 ,88 In a 1-year prospective case study of two amenorrhoeic athletes undergoing controlled increased energy intake, recovery of menses coincided closely with increases in caloric intake and weight gain; body weight increased by 2.8 kg (5%) and 4.2 kg (8%) at 12 months in the two participants.94 In a 5-year retrospective study of college athletes undergoing non-pharmacological therapy, Arends et al89 reported a significant increase in weight of 9% (mean weight gain: 5.3±1.1 kg) in the 17.6% oligomenorrhoeic or amenorrhoeic athletes who resumed menstrual function (mean time to recovery: 15.6±2.6 months) versus minimal weight gain (weight gain of 1.3±1.1 kg) in those who did not resume menses. Causal evidence of the efficacy of increased energy intake to reverse menstrual disturbances was provided by Williams et al5 in female cynomolgus monkeys who demonstrated that restoration of menses was accompanied by an average weight gain of 5.7%.
Weight gain that leads to recovery of menstrual function is linked to improvement of other clinical outcomes characteristic of exercise-associated amenorrhoea including low BMD90 ,95 ,96 and impaired endothelial function.97 More research is necessary to establish the time course of weight changes and the sensitivity, specificity and success of nutritional and dietary interventions.
What are the components of non-pharmacological treatment for each Triad condition?
Owing to the multifactorial aetiology of the Triad, the Panel has established that an optimal treatment approach must address the underlying cause of the Triad, that is, low EA.2 Energy status must be normalised primarily through modifications of diet and exercise training, if necessary, with the goal of increasing EA.2 ,29 The consensus of our recommendations is focused on restoration or normalisation of body weight as the best strategy for successful resumption of menses and improved bone health.2 ,89 ,90 ,96 ,98 The Panel notes that the development of any Triad treatment plan should include a consideration of the goals of the athlete, her unique diet and training practices, any coexisting conditions and a system for monitoring changes.
Specific non-pharmacological recommendations for interventions in athletes with low EA
Specific treatment recommendations developed by the Panel depend on identifying how low EA developed in the athlete. There may be four unique pathways to low EA, and as such, four unique treatment recommendations.
-
If the cause of low EA is inadvertent undereating, then referral for nutritional education is sufficient. Nutritional education should ideally include a sports dietitian. An exercise physiologist can also complete an assessment of energy expenditure and EA.
-
If the cause for low EA is DE, the referral should be to a physician and for nutritional counselling with a sports dietitian.
-
If the cause for low EA is intentional weight loss without DE, then referral for nutritional education is sufficient.
-
If the cause for low EA involves clinical ED, treatment should include evaluation and management with a physician, nutritional counselling with a sports dietitian and referral to a mental health practitioner for psychological treatment.2 ,99 In this case, the reversal of low EA will not be possible without psychological treatment.2 ,99–102
In general, the primary goal of treatment is to restore or normalise body weight, concomitant with an improvement in overall nutritional and energetic status.2 ,103 ,104 When DE is apparent, the Panel emphasised that the treatment plan in these athletes must focus on the modification of unhealthy attitudes, behaviours and emotions related to food and body image that may perpetuate the DE.101 ,103 ,104 Weight gain is a primary concern for athletes with FHA who are underweight and it is important to emphasise that the amount of weight gain that typically leads to resumption of menses is variable among individuals.87 ,88 ,94 In studies thus far, a range of approximately 5–10% of body weight or 1–4 kg of weight gain has been observed.87 ,88 ,94 This weight gain is often comprised of gains in fat mass in anorexic women,91–93 but in exercising women without clinical ED, gains in FFM have also been observed.87 ,94
Treatment targets for low EA
The Panel identified that targets of treatment are varied and depend on individual circumstances. Specific treatment targets may include one or more of the following:
-
Reversal of recent weight loss105;
-
Return to a body weight associated with normal menses90–94;
-
Weight gain to achieve a BMI of ≥18.5 kg/m2 or ≥90% of predicted weight90 ,91 ,100 ,106 ,107;
-
Energy intake should be set at a minimum of 2000 kcal/day or more likely; a greater energy intake will be required, depending on exercise energy expenditure.94 ,108
Since the treatment goal is to restore or normalise body weight, the Panel recommended an increase in dietary energy intake, a decrease in exercise energy expenditure, or both. Recommendations should consider individual preferences and may depend on where the athlete is in the competitive season (reductions in training volume may not be feasible in season; acceptance of reductions in training volume may be better received vs increased energy intake). Prescribed changes in energy intake to achieve an increased BMI and/or body weight goal should be gradual, beginning with an approximately 20–30% increase in caloric intake over baseline energy needs, or the amount of energy required to gain approximately 0.5 kg every 7–10 days.87 ,88 ,94 For an athlete consuming 2000 kcal/day, this would represent a gradual increase of 200–600 kcal/day, accomplished over several months. If EA (intake kcal−exercise kcal)/kg of FFM can be reliably estimated, the target should be at or greater than 45 kcal/kg of FFM. Specific strategies that have been successful in female athletes have been detailed in case study investigations.87 ,88 ,94
Steps in a plan to increase EA
-
Step 1: Perform an assessment of baseline energy needs that includes a thorough body weight history including questions about associated changes in menstrual status. Energy intake can be assessed using diet logs and dietary analysis programmes. Energy expenditure can be estimated by measuring or estimating RMR and exercise energy expenditure. RMR can be estimated using one of the several algorithms,109–111 and multiplying by an activity factor112 ,113 will account for exercise energy expenditure, thereby providing an estimate of total energy expenditure needs.
-
Step 2: Using the appropriate target for EA, meal plans should be developed that incorporate a variety of factors. Specifically, diet quality, diet variety, food preferences and practical aspects of food availability should be considered. Goals would include achieving an adequate balance of macronutrients and appropriate intake of micronutrients, particularly calcium, vitamin D, iron, zinc and vitamin K. Whenever possible, the recommendation should be to increase intake of real foods versus dietary or meal supplements. Dietary recommendations should include incorporation of energy and nutrient-dense foods such as fortified milk drinks and essential fatty acids in the form of fish, healthy oils, nuts avocados and dried fruit. If there is a possibility of gastrointestinal discomfort with high caloric loads, small and frequent meals should be consumed throughout the day, with timing dependent on practice and competition. Particular attention should be paid to identifying times across the day where dietary energy intake may be particularly low.114 Adjustments in dietary strategies for increasing EA should also take into account changes across the season in accordance with competition schedules.
A successful treatment plan requires standardised periodic monitoring of body weight. Athletes should be weighed on the same scale, wearing minimal clothing, such as shorts and a t-shirt, to reduce the likelihood of falsifying their weight.115 The frequency of weight monitoring depends on the degree to which weight determines health and eligibility to participate in sport. A reasonable frequency is weekly when initiating a treatment programme.
Specific recommendations that target ED
The goals of treatment for exercising women with ED is to normalise pathological eating behaviours, reduce dieting attempts and alter negative emotions and beliefs associated with food and body image.116 Cognitive behavioural therapy (CBT) has been demonstrated to be an effective treatment approach for exercising women with ED117–119 and may be more beneficial than nutritional counselling alone in some women with amenorrhoea particularly if DE behaviour is present.120 CBT may assist women with DE behaviours and body image disturbances to comply with an increased energy intake prescription and associated weight gain.
Specific recommendations that target low BMD
In exercising women with low BMD, the Panel recommendations include increasing EA and optimising weight gain and resumption of menses.121 Calcium and vitamin D status should be addressed.
The aetiology of bone loss among amenorrhoeic women includes energy deficiency-related factors and oestrogen deficiency.7 ,9 ,122 Thus, weight gain and subsequent resumption of menses are key to prevent further loss of bone mass.90 ,95 It is estimated that amenorrhoeic women will lose approximately 2–3% of bone mass per year if the condition remains untreated.90 ,95 ,96 Data on recovery of bone mass in amenorrhoeic athletes secondary to increased energy intake are limited. However, significant improvements in bone health outcomes were observed in case studies of amenorrhoeic female athletes who gained weight.105 ,106 In studies of anorexic women, investigators provide evidence of increases in BMD (1–10%) associated with weight gain and resumption of menses,90 ,95 ,123 ,124 whereas, continual decreases in BMD were observed in those who did not recover menses.90 ,95 Miller et al95 reported that resumption of menses occurred in 75 anorexic women who gained 4 kg of body mass, on an average, and the combined effects of weight gain and resumption of menses contributed to significant improvements in lumbar spine (3.1%) and hip BMD (1.8%). Misra et al90 demonstrated that menstrual recovery and weight gain attenuated further decreases in BMD in 34 anorexic girls aged 12–18 years over a 12-month period of time. In other prospective studies, similar findings are reported.124 ,125
In a retrospective study by Arends et al,89 percentage weight gain was identified as the strongest predictor of resumption of menses in female collegiate athletes, and may also be a predictor of gains in BMD. Findings from case reports105 ,106 and retrospective analyses89 published to date demonstrate that weight gain can lead to substantial increases in BMD in an energy replete environment. Prospective, randomised controlled trials (RCTs) are necessary in large samples of exercising women with amenorrhoea and low BMD to confirm the beneficial effects of increased body weight accomplished by increased energy intake on BMD.
Furthermore, substantial evidence exists in support of the positive effect of weight gain alone on BMD. Weight gain independent of resumption of menses has been shown to have a positive effect on BMD, and to restore the coupling of bone formation and resorption.90 ,124–127 However, in spite of some recovery of bone mass, normalisation of BMD is unlikely to occur with weight gain alone. From a treatment standpoint, energy and oestrogen-dependent mechanisms of bone loss must be addressed in order to promote optimal increases in BMD. In summary, nutritional and hormonal recovery is recommended to improve mineralisation of trabecular bone and the growth of cortical bone.90 ,95 ,128
Weight-bearing exercise is a primary non-pharmacological strategy for increasing and maintaining BMD and geometry across the lifespan.129 Bone tissue is highly responsive to dynamic and high-magnitude loading,130 high-impact loading131–135 and resistance training.136 ,137 Experiments in animals provide evidence of the positive effect of mechanical loading for optimising bone formation.138 ,139 In a recent meta-analysis (n=521; 7 studies—randomised controlled exercise trials ≥24 weeks) of the effects of exercise on BMD in premenopausal women,140 significant improvements in femoral neck and lumbar spine BMD were observed following weight-bearing exercise training. This finding highlights the utility of exercise (aerobic, strength and/or high impact) for improving BMD at weight-bearing sites in premenopausal women. Specifically, programmes with a combination of high-impact loading and resistance training represent effective methods of optimising bone in the premenopausal years.141 Notably, in studies of the effect of high-impact loading or resistance training alone on BMD, investigators demonstrate mixed results.141 ,142 The majority of weight-bearing exercise interventions involved 2 or 3 days of training per week.141 For a review of the effects of exercise and bone, the reader is referred to the ACSM Position Stand on Bone Health and Exercise.143
To date, prospective studies are lacking wherein investigators explore the impact of resistance training and high-magnitude loading on the bone health of amenorrhoeic athletes. However, lean mass has been reported to be a strong predictor of hip BMD among anorexic adolescents144 and also adolescent athletes and non-athletes.145 In agreement with these results, a longitudinal study assessing skeletal recovery in anorexic women over the course of 6–69 months demonstrated that per cent change in FFM was a significant positive predictor of the change in hip and lumbar spine BMD and, furthermore, was a stronger predictor of BMD change than the change in fat mass or body weight.95 These results suggest that increases in lean mass may be an important component of weight recovery, and, as such, the lean mass gained through resistance training may be beneficial for BMD in amenorrhoeic athletes. Increases in lean mass may also be beneficial for increasing bone size,146 thus improving bone strength and decreasing the risk of fracture, and improving athletic performance.
The Panel expressed concerns that high-impact activity in females with low BMD (±fractures) may in fact result in fracture.147 Further studies are necessary to determine the impact of combined weight-bearing programmes on BMD and fracture risk in athletes with low BMD. There is also the notion that oestrogen may be permissive for the osteogenic effects of mechanical loading,148 as data have demonstrated poor osteogenic benefits of mechanical loading in chronically amenorrhoeic athletes.128 ,149 ,150
What is the recommended time course of non-pharmacological treatment (including follow-up)?
Treatment of the Triad conditions by increasing EA will result in recovery of physiological systems at different rates. Notably, the time to resumption of menses may vary among exercising women and is dependent on the severity of the energy deficiency and duration of menstrual dysfunction.89 ,90 ,94 An increase in EA can positively alter metabolic hormone profiles within days to weeks, with concomitant changes in body weight occurring over weeks and months. Weight gain has been observed as a clinically positive outcome associated with resumption of menses and enhanced bone health in exercising women.87 ,90 ,95 ,105 ,106 The recovery of menstrual function with strategies to increase EA can occur within several months94 but may take longer than 1 year.89 Improvements in BMD will occur more slowly, often over several years. Whether or not BMD can be restored to levels appropriate for age and training status remains unclear.151–153 A schematic of the time course of recovery of Triad factors is displayed in figure 3.

Female Athlete Triad: Cumulative Risk Assessment. The cumulative risk assessment provides an objective method of determining an athlete's risk using risk stratification and evidence-based risk factors for the Female Athlete Triad.16 ,17 ,46 This assessment is then used to determine an athlete's clearance for sport participation (figure 5). ‡Some dietary restriction as evidenced by self-report or low/inadequate energy intake on diet logs; *current or past history41 ,57; ** ≥90% EW66 ,91 ,100 ,107; absolute BMI cut-offs should not be used for adolescents. ***Weight-bearing sport2; † high-risk skeletal sites associated with low BMD and delay in return to play in athletes with one or more components of the Triad include stress reaction/fracture of trabecular sites (femoral neck, sacrum, pelvis).18 ,83 BMD, bone mineral density; BMI, body mass index; DE, disordered eating; EA, energy availability; EW, expected weight; ED, eating disorder.
Summary comments regarding non-pharmacological treatment
Overall, successful treatment of athletes and exercising women is contingent on a multidisciplinary approach for recovery from the Triad,2 ,154 including a primary care and/or sports medicine physician, a sports dietitian and mental health practitioner. Depending on the individual situation, consultation from an endocrinologist, orthopaedic surgeon, psychiatrist, exercise physiologist, certified athletic trainer, family members and/or team coach (if applicable) may be helpful. This treatment approach is based on trusting and respectful interactions between healthcare providers and affected individuals. Consideration of the effects of treatment goals on health status, athletic performance and personal identity/lifestyle is necessary to ensure treatment compliance and post-treatment adherence by affected female athletes and exercising women.
Pharmacological treatment strategies for the clinical sequelae of the Triad
Overview
Non-pharmacological measures should constitute initial management in female athletes with the Triad. For treatment of osteoporosis and/or in those athletes with multiple fracture history, the panel emphasised that pharmacological management is to be considered if there is a lack of response to non-pharmacological therapy for at least 1 year and if new fractures occur during non-pharmacological management. Pharmacological management may also be necessary in the psychological treatment of ED and DE, especially if there are significant comorbid conditions.
Low energy availability, disordered eating and eating disorders
The Panel emphasised that low EA indicates that there is a problem, but does not differentiate between transient energy imbalance, DE and clinically significant ED. Individuals who have unintentional low EA or mild DE may respond well to nutritional education designed to eliminate low EA. Individuals with significant DE may benefit from counselling with a mental health practitioner, in addition to nutritional education. In contrast, individuals who have an ED require intensive interdisciplinary attention and treatment. The American Psychiatric Association Practice Guidelines for the Treatment of ED recommend a multidisciplinary team approach to treatment including a physician, mental health provider and sports dietitian.155 Results of small randomised trials involving treatment approaches that include mindfulness training, dialectical behaviour therapy and other therapeutic approaches are emerging.156 ,157 Antidepressant medications, particularly selective serotonin reuptake inhibitors, can be helpful in the treatment of bulimia nervosa.158 The APA Practice Guidelines describe limited evidence to use medications to restore weight, prevent relapse or treat chronic anorexia nervosa. Other psychotropic medications can be beneficial in treating comorbid conditions, such as anxiety, depression and obsessive compulsive behaviour.155
One of the challenges in addressing low EA is that it may be difficult to identify which individuals have an ED that requires more comprehensive treatment. This can be amplified by denial that there is a problem and minimisation of the difficulty in changing behaviours, which are common themes for individuals with ED. The team physician should work closely with the multidisciplinary team to determine the best treatment approach for an individual athlete. Readers are referred to the most recent Diagnostic and Statistical Manual of Mental Disorders, 5th ed (DSM-V) for full diagnostic criteria of ED.81
Menstrual dysfunction
Pharmacological strategies that target menstrual dysfunction are mostly experimental, as are strategies to optimise bone accrual in the adolescent athlete and to optimise BMD in adult athletes and exercising women, defined as at least 20 years old.
When considering pharmacological strategies to address amenorrhoea and hypoestrogenemia in athletes and exercising women, the Panel emphasised that it is essential to reiterate that combined oral or non-oral routes of contraceptive therapy do not restore spontaneous menses; indeed, contraceptive therapy simply creates an exogenous ovarian steroid environment that often provides a false sense of security when induced withdrawal bleeding occurs.159 Moreover, combined oral contraceptive (COC) therapy is not consistently associated with improved BMD in amenorrhoeic athletes160–162 and may in fact further compromise bone health given first-pass effects on hepatic production of insulin-like growth factor-1 (IGF-1), an important bone trophic hormone 163–165 (details in ‘Replacement of gonadal steroids’ section). Therefore, the Panel emphasises that non-pharmacological treatment strategies should be prioritised, particularly focusing on achieving resumption of menses,95 ,106 given the importance of menses and normal oestrogen status to bone health.8 ,29 ,128 ,145 ,166
Consequences of hypogonadism (FHA) in athletes for which pharmacological treatment should be considered include:
-
Symptoms of oestrogen deficiency, such as vaginal dryness and dyspareunia;
-
Infertility;
-
Impaired bone health (despite implementation of non-pharmacological therapy).
On the basis of the aetiopathogenesis of the Triad and the specific consequence of associated hypogonadism that requires treatment, several possible pharmacological strategies may be considered if non-pharmacological management is unsuccessful. This paper will address pharmacological options more specific to the consequence of impaired bone health.
Replacement of gonadal steroids
The major gonadal steroids include oestrogen, progesterone and testosterone, all of which are low in the amenorrhoeic athlete.
Oestrogen replacement: Overall, investigators have shown that oral oestrogen–progesterone combination pills are not an effective strategy to increase BMD in low-weight conditions such as anorexia nervosa (in adults and adolescents).167 ,168 Studies of COCs or hormone therapy in athletes with FHA are less definitive.169 Available studies in women with FHA include retrospective,170 ,171 prospective172–174 and cohort studies175 ,176; however, very few RCTs have been performed.160–162 ,177 In addition, most of these studies in women with FHA did not specifically target exercising women with FHA.
Pharmacological treatment that aims to restore regular menstrual cycles with COC does not normalise metabolic factors impairing bone health and will therefore likely not result in reversal of low BMD in the athlete with Triad disorders.2 ,159 ,172 The lack of efficacy of oral oestrogen in improving BMD in conditions of low-weight and possibly normal-weight exercise-induced amenorrhoea has been attributed to the suppressive effects of oral oestrogen on hepatic IGF-1 production.163 ,164 ,173 IGF-1 is a bone trophic factor that is secreted by the liver in response to growth hormone and is also produced locally in an autocrine manner by target tissues such as bone.178 It is speculated that the first-pass effect of exogenous oestrogen through the liver suppresses IGF-1 production and upregulates the synthesis of binding proteins, such as IGFBP-1, which bind to IGF-1, further reducing its bioavailability.163 Given the low endogenous concentration of IGF-1 in amenorrhoeic athletes,145 a further reduction in IGF-1 levels secondary to the administration of oral oestrogen likely limits the beneficial antiresorptive effects of oestrogen.179 In addition, the type and dose of oestrogen have been implicated in the lack of efficacy of oral oestrogen in increasing BMD in energy-deficient states.168 As is stated in the 2007 ACSM Female Athlete Triad Position Stand, however, for women with FHA, increases in BMD are more closely associated with increases in weight than with COC administration,2 ,161 so these treatments likely need to be implemented in combination with non-pharmacological treatment to optimise the effectiveness.161
Transdermal oestradiol administration when given in replacement doses does not suppress IGF-1164 ,180–182 and therefore warrants further investigation as an alternative to COC therapy in the amenorrhoeic female athlete with the Triad. In a RCT in adolescent girls with anorexia nervosa, transdermal oestradiol administered at doses of 100 μg twice weekly, along with cyclic progesterone (2.5 mg daily for 10 days of every month to prevent unopposed oestrogen stimulation of the uterus), increased their BMD without a reduction in IGF-1 levels.180 Bone accrual rates in girls with anorexia nervosa who received transdermal oestradiol approximated that in normal-weight controls after controlling for weight changes, and BMD Z-scores were maintained.180 However, bone accrual needs to exceed that in controls for ‘catch-up’ to occur and for BMD Z-scores to normalise to >–1.0. Likely because other hormonal alterations persist, catch-up does not always occur, as was shown in the same study.180 Although there are no published data regarding use of transdermal oestradiol in FHA, RCT studies are ongoing to address this possible treatment strategy, and further study is warranted.
Vaginal oestradiol administration also circumvents hepatic first-pass metabolism, and a vaginal oestrogen–progesterone combination contraceptive ring is now available. However, data regarding the impact of this form of oestrogen administration on BMD are conflicting with one study suggesting maintenance of BMD, and another suggesting that it may be deleterious to bone compared with no treatment in premenopausal women.183 ,184 Thus further research on vaginally applied oestrogen is necessary.
Data are limited regarding the impact of pharmacological therapies on muscle perfusion, although one study reported an improvement in endothelial dysfunction with use of COC therapy.185
Testosterone replacement: The other gonadal hormone that is low in conditions of low weight and in amenorrhoeic athletes and exercising women is testosterone, which has antiresorptive effects (direct and oestrogen mediated)186 ,187 and also bone anabolic effects.187 ,188 There are no data available on testosterone administration in amenorrhoeic athletes and exercising women. However, a recent study in adult women with anorexia nervosa demonstrated no improvement in BMD with low-dose testosterone administration, despite increases in lean mass and initial increases in surrogate markers of bone formation.189
Normalising gonadotropin pulsatility and secretion
As stated earlier, the Panel contends that increasing EA through nutritional intervention is the best strategy for normalising gonadotropin pulsatility and secretion. From a pharmacological perspective, experimental strategies include administering hormones that are low in Triad conditions and that mechanistically can contribute to amenorrhoea and to low BMD, such as leptin and IGF-1, or administering antagonists of hormones that are high in Triad conditions and can contribute mechanistically to amenorrhoea and low BMD, such as ghrelin, peptide YY (PYY) and adiponectin.
Leptin: Few studies have examined the impact of administering metreleptin to women with FHA.190–192 Although metreleptin improved ovulatory status and increased BMC in women with FHA, the women sustained significant weight loss and reductions in fat mass, even when doses of the drug were carefully titrated.190–192 These data are concerning and suggest that leptin administration is not a good therapeutic strategy to normalise gonadotropin secretion and increase BMD in energy-deficient states, as in amenorrhoeic athletes and exercising women.
IGF-1 replacement: An important contributor to low BMD in amenorrhoeic athletes and exercising women is low IGF-1, particularly in those who are low weight. In adolescents and adults with anorexia nervosa, administering recombinant human IGF-1 (rhIGF-1) increases the levels of surrogate bone formation markers,193 ,194 and in one RCT in adult women with anorexia nervosa, giving rhIGF-1 (a bone anabolic hormone) with oral oestrogen (antiresorptive) led to a 2.8% significant increase in BMD when compared with the group that received neither.194 Data are lacking regarding the efficacy of rhIGF-1 administered alone or with oestrogen in improving bone health in exercise-induced amenorrhoea.
Other hormones: Although in vitro studies and studies in rodents have demonstrated that high ghrelin, PYY and adiponectin inhibit gonadotropin secretion,195–197 and high PYY and adiponectin are deleterious to bone,197–200 there are no data in animals or humans examining the impact of antagonists to these hormones on gonadotropin secretion and bone metabolism. In addition, a ghrelin antagonist runs the risk of eliminating the adaptive increase of an orexigenic stimulus, namely ghrelin, in this energy-deficient state.
Bone mineral density
Data are lacking regarding the efficacy of pharmacotherapy in treating low BMD with or without a fracture history in female athletes. While pharmacological therapy is recommended in postmenopausal women and men ≥ age 50 years201 with osteoporosis, the threshold for pharmacological treatment in the young female athlete with low BMD, stress fractures and/or impaired bone accrual is less clear.
It should be noted that the bones of amenorrhoeic and eumenorrhoeic athletes are subject to greater stress and strain secondary to specific athletic activities than that experienced by bones in non-athletes.202 Indeed, weight-bearing athletes should have higher BMD and other proxy indicators of bone strength secondary to chronic mechanical loading when compared with non-athletes.128 ,130 ,203 The 2007 ACSM Position Stand on the Triad thus suggested that BMD Z-scores of <−1.0 in athletes involved in repetitive or high-impact stress may be low enough to increase fracture risk, especially in those with additional risk factors for the Triad.2 In addition, athletes with Triad risk factors who sustain bone stress injuries may have a delay in return to sport.18 However, it is still not clear whether pharmacotherapy is beneficial in athletes with low BMD in the absence of a fracture history, and more importantly, whether or not treatment in this population prevents fractures and/or improves healing time and recovery in those who have sustained bone stress injuries.
Furthermore, some girls and women may have a genetically determined low peak bone mass, or may have had previous insults to the skeleton (such as poor nutrition and FHA) that have since resolved. In these cases, BMD may have stabilised, in contrast to a female athlete with ongoing low EA and amenorrhoea, who may have continued decreases in BMD, which could increase vulnerability to bone stress injury and fracture. Serial DXA measurements may be helpful in making this determination. There are currently no guidelines regarding the timing of initiation of pharmacological treatment in young female athletes with established osteoporosis or for DXA assessment and follow-up (boxes 2. and 3).
Definition of low bone mineral density (BMD) and osteoporosis in premenopausal women
-
The diagnosis of osteoporosis in premenopausal women cannot be diagnosed on the basis of BMD alone.
-
A BMD Z-score of ≤−2.0* is defined as ‘below the expected range for age’.
-
A BMD Z-score above −2.0 is ‘within the expected range for age’.
-
Osteoporosis is diagnosed if there is a BMD Z-score of ≤−2.0 plus secondary causes of osteoporosis.
Source: Lewiecki et al.80
*American College of Sports Medicine (ACSM) defines low bone mineral content or BMD as a Z-score that is less than −1.0 in female athletes in weight-bearing sports.2
The Panel has concluded that the decision to treat or not with pharmacological therapies does not depend on BMD Z-scores alone, but also on additional risk factors such as fracture history, genetics,204 cumulative Triad risk factors, which have been associated with an increased risk for low BMD and bone stress injury, and rate of bone loss with non-pharmacological management.17 ,46 The Panel suggests that the nature of athletic activity, response to non-pharmacological management as demonstrated by return of menses and/or as noted on serial DXA assessments,2 severity of the medical situation, fracture history and genetic predisposition should all play a role in the decision to treat with pharmacological therapy.
The Panel emphasised caution when considering FDA-approved postmenopausal treatment strategies for use in premenopausal women and children including Triad athletes and exercising women. Bisphosphonates have a very long half-life, and should be used with extreme caution in women of childbearing age for concerns of teratogenicity,205 ,206 although data to date are reassuring. The decision to initiate treatment with bisphosphonates in any premenopausal woman should be made on a case-by-case basis. Consideration should include individual fracture risk and potential medication-related adverse effects. There is concern regarding long-term use of bisphosphonates and the association with atypical femur fractures207 ,208 and osteonecrosis of the jaw.209 In addition, there are no published studies of bisphosphonate use in exercising and athletic women with Triad disorders. In one study in adult women with anorexia nervosa, bisphosphonate therapy (specifically risedronate) increased lumbar spine BMD compared with placebo189; however, a study in adolescent women with anorexia nervosa demonstrated no increase in spine BMD with alendronate given for a year.210 Bisphosphonates act by inhibiting bone resorption, and the differential effect of bisphosphonates in adults versus adolescents may relate to increased bone resorption in adults compared with a reduction in bone resorption in adolescents.211 There are a few special considerations for using bisphosphonates in the younger population, such as glucocorticoid-induced osteoporosis and osteogenesis imperfecta212–214 The Panel emphasised that any use of bisphosphonate therapy in young women with the Triad should only be executed by or in consultation with a board-certified endocrinologist or specialist in metabolic bone diseases. “It must be emphasized that the aforementioned pharmacological therapies are not currently approved by the FDA for increasing BMD or for fracture reduction in young or adult athletes.”189 ,215
To date, there are no published studies of denosumab or teriparatide use in girls and women with Triad disorders. A preliminary report in older women with anorexia nervosa demonstrated that treatment with teriparatide for 6 months increased bone formation (158%) and lumbar spine BMD (anteroposterior spine 6% and lateral spine 10.5%) compared with placebo.216 There is also a case study that suggests that 4 weeks of teriparatide was associated with bone healing, reduced pain and resumption of normal activities in two premenopausal women with stress fractures.217
Pharmacological treatment considerations
Which athletes and exercising women should be targeted for pharmacological therapy?
The Panel emphasised that non-pharmacological therapy is the mainstay of treatment for all athletes with one or more components of the Triad.
The Panel concluded that there is no evidence at this time to unequivocally recommend pharmacological therapy in athletes with the Female Athlete Triad disorders due to lack of evidence-based research in this population. The Panel discussed that lack of response to non-pharmacological management (see definition below) may present a situation in which pharmacological therapy would be considered in an athlete with low BMD and a clinically significant fracture history. ‘Pharmacological medications other than oestrogen and progesterone are not recommended in the absence of a fracture history’.
Pharmacological therapy may be considered in an athlete with:
-
BMD Z-scores ≤−2.0 with a clinically significant fracture history (boxes 2 and 3; figure 3) AND lack of response to at least 1 year of non-pharmacological therapy (mainstay of treatment).
-
BMD Z-scores between −1.0 and −2.0 with a clinically significant fracture history (boxes 2 and 3) and ≥2 additional Triad risk factors1,7 ,46 (figure 4) AND lack of response to at least a year of non-pharmacological therapy.
Transdermal oestradiol replacement with cyclic progesterone may be considered in young athletes ≥16 and <21 years of age with FHA to prevent further bone loss during this critical window of optimal bone accrual if they have
-
BMD Z-scores ≤–2.0 without a clinically significant fracture history (boxes 2 and 3; figure 4) and at least one additional Triad risk factor17 ,45 (in addition to FHA; figure 4) AND lack of response to at least 1 year of non-pharmacological therapy.
Lack of response to therapy has been defined as
-
A clinically significant reduction in BMD Z-scores after at least 1 year of non-pharmacological therapy, or
-
Occurrence of new clinically significant fractures during non-pharmacological treatment over the course of 1 year.
Further research is warranted to assess the outcomes of pharmacological management and potential risks in this population. Although stress fractures are generally believed to be less concerning than non-stress fractures, they are a common and frequent cause of morbidity, time away from training and competition in athletes and loss of school and work days. In certain instances, these stress fractures can progress to devastating complete fractures at high-risk sites, such as the femoral neck,218 ,219 with consequences that can result in surgery and negatively affect exercise activity and quality of life. Of note, prolonged non-pharmacological management despite lack of response is of concern in younger athletes who are in the process of accruing peak bone mass, because the adolescent and young adult years are a critical window in time during which to optimise bone accrual,149 ,220 and deficits incurred at this time may be irreversible.152
As stated, there are no current treatments approved by the FDA for this specific population.215 Further research on pharmacological treatment alternatives is needed in this higher risk group of athletes with low BMD and a fracture history, as well as those with low BMD without a fracture history.
What therapy can we offer?
Increasing EA and optimising energy status
-
The Panel unanimously agreed that all athletes and exercising women, particularly those who are considered candidates for pharmacological therapy, should be counselled regarding lifestyle and behavioural changes to increase EA and optimise energy status.
-
Non-pharmacological management should continue, even if pharmacological therapy is prescribed.
Calcium and vitamin D
-
Calcium-rich foods should be recommended with optimal calcium intake between 1000 and 1300 mg/day.221
-
Vitamin D status should be optimised. Daily intake of 600 IU of vitamin D is recommended by the Institute of Medicine for adolescents and adults up to age 70.221 Higher doses may be needed if they are deficient or insufficient in vitamin D. The panel recommended that vitamin D levels be maintained between 32 and 50 ng/mL.222
Oestrogen administration in female athletes with FHA or prolonged oligomenorrhoea who have failed non-pharmacological management
-
In athletes and exercising women with FHA and prolonged amenorrhoea of hypothalamic origin who meet criteria for pharmacological therapy, a reasonable option is oestrogen administration with cyclic progesterone after ruling out other causes of amenorrhoea. It is also essential to consider contraceptive needs of the athlete. Before starting therapy, a thorough history and examination should be conducted to rule out contraindications for oestrogen therapy.
-
COC therapy containing 20–35 μg of ethinyl oestradiol may maintain BMD in those with very low BMD measures, although data are not definitive.168 ,172 Most of the studies in adolescents and adults with anorexia nervosa and in amenorrhoeic athletes suggest that COC therapies are not effective in increasing BMD161 ,162 ,167 ,168 or in reducing stress fractures,161 although they are effective for contraceptive needs when used in recommended doses.
-
Transdermal oestradiol (100 μg of 17β oestradiol) with cyclic progesterone maintains BMD Z-scores in adolescents with anorexia nervosa,180 and is a consideration for low-weight, amenorrhoeic athletes who meet criteria for pharmacological intervention. Athletes who are symptomatic with this dose for oestrogen-related side effects such as nausea, bloating and breast tenderness may be started on a lower dose of the transdermal patch (50 μg) and the dose increased to 100 μg after 1 month.
-
Cyclic progesterone is necessary in those on transdermal oestradiol to avoid deleterious effects of unopposed oestrogen on the uterine lining, and we recommend 200 mg of micronised progesterone or 5–10 mg of medroxy progesterone acetate for 12 days of every month.223 ,224
-
Of importance, the combination of transdermal oestradiol and cyclic oral progesterone in the described doses has unproven contraceptive efficacy, and other contraceptive methods are necessary if contraception is desired.
-
If oestrogen replacement is considered in an athlete with a known or family history of thrombophilic disorders, we recommend consulting with a haematologist to assess whether tailoring the oestrogen dose, route and regimen to minimise risk is an option, with full written informed consent of the patient.225 If oestrogen replacement is instituted, management should include ongoing follow-up with a haematologist.
-
Testosterone, DHEA, leptin or rhIGF-1 replacement is not recommended at this time in athletes who meet criteria for pharmacological therapy, due to lack of studies in the female athlete population and potential adverse effects.
When should pharmacological options other than oestrogen be considered as options for treatment?
Pharmacological options other than oestrogen replacement/COC
-
In rare instances, pharmacological management other than oestrogen replacement/COC therapy can be considered when athletes meet the criteria for osteoporosis and have failed non-pharmacological therapy (with recurrent fractures), and meet one of the following criteria
-
Contraindications to oestrogen;
-
Lack of response to oestrogen replacement after ≥18–24 months in a compliant patient;
-
Eumenorrhoeic athletes/exercisers (not hypoestrogenic) who meet criteria for therapy;
-
Athletes with multiple debilitating fractures and significant morbidity.
-
-
For the last two indications, patients should undergo a complete metabolic work-up, and genetic testing may be considered depending on the history of the patient and her family history.
-
Other pharmacological options include bisphosphonates and teriparatide, which are effective strategies for treating postmenopausal osteoporosis226 ,227 and osteoporosis in special populations,212 ,213 but for whom data are limited, that is, in younger women, including female athletes. If such options are considered, the athlete/exerciser should be referred to an endocrinologist or an expert in metabolic bone diseases for further management, and treatment should be implemented only in conjunction with the endocrinologist or expert in metabolic bone disorders.
-
Teriparatide is administered once daily as a subcutaneous injection and is bone anabolic. While this is a promising agent in adult athletes and studies are ongoing, data regarding its efficacy in a younger population are lacking at this time. Of note, this drug is contraindicated in pregnancy, and there is a black box warning for those at increased baseline risk for osteosarcoma, namely children with open epiphyses, individuals with unexplained elevations of alkaline phosphatase, those with Paget's disease and individuals with a prior history of external beam radiation therapy or implant radiotherapy of the skeleton (Product Information: FORTEO(R) subcutaneous solution, teriparatide subcutaneous solution. Eli Lilly and Company, Indianapolis, IN, 2004).
-
Bisphosphonates are effective in increasing BMD in adult women with anorexia nervosa,189 but should be considered in athletes who meet criteria for pharmacological intervention with options other than oestrogen replacement, only when no other strategy is effective or when other strategies are contraindicated. Reproductive age women taking bisphosphonates should be prescribed birth control measures and counselled at length regarding the very long half-life of these medications and potential teratogenic effects on the fetus should pregnancy occur. If bisphosphonate therapy is prescribed, a time limit for these ongoing treatments, as in adults, should be considered due to potential risks of prolonged therapy.205 ,206
-
There are no known studies using denosomab for osteoporosis treatment in premenopausal women or children, and thus this pharmacological alternative is not recommended and remains experimental in this group.
Clearance and return to play
Despite widespread awareness and educational efforts on the Female Athlete Triad,2 ,3 ,228 there have been no standardised guidelines for clearance and return to play. As a result, many female athletes with the Triad are being cleared at their preparticipation physical examination without being adequately assessed, managed or treated, and often return to play without structured follow-up.
How can risk stratification be used to evaluate health and participation risk?
Recent studies assessing health outcomes of single and combined risk factors for the Triad have demonstrated that there is an increased cumulative risk for the outcomes of low BMD,46 stress fracture and bone stress injury,16 ,17 resulting in a dose–response relationship that is related to the magnitude of risk of Triad disorders and subsequent impact on bone health and susceptibility to fracture. These findings are of significance with regard to management of the Triad, clearance and return to play, and emphasise the important role that risk stratification may have in optimising the athlete's health and minimising risk for injury and illness.
Prospective return-to-play data have demonstrated that female collegiate runners with menstrual dysfunction had more severe bone stress injuries on MRI compared with eumenorrhoeic runners.18 Low BMD and higher MRI grade bone stress injuries were independent predictors of delay in return to play. In addition, athletes with bone stress injuries in skeletal sites of predominantly trabecular bone structure (femoral neck, sacrum and pelvis) had a delay in return to play compared with those athletes with bone stress injuries at cortical bone sites.18 Marx et al83 found that female athletes with stress fractures in regions of mostly trabecular bone had lower BMD than those at cortical sites. These studies18 ,83 highlight the importance of Triad risk factors on bone stress injury outcomes and the value of risk stratification. Future research is needed to assess the impact of Triad risk factors on return to play.
What is the role of the team physician in the return-to-play decision for Triad athletes?
According to the 2012 Consensus Statement on “The Team Physician and the Return to Play Decision,”229 the physician's duty is “to return an injured or ill athlete to practice or competition without putting the individual at undue risk for injury or illness.” In addition, the team physician's role is to establish a return-to-play process, evaluate the athlete with medical conditions, treat and rehabilitate the athlete and return the athlete to play after it is determined to be safe to do so.
In summary, with increasing evidence that the athlete's risk for unfavourable outcomes of low BMD and/or bone stress injuries is greater with cumulative risk factors for the Triad,16 ,17 ,46 evidence that Triad risk factors may contribute to more severe bone stress injuries and a delay in return to play,18 and due to the lack of standard of care guidelines for the Triad, the Panel recommends the following risk stratification protocol to be implemented (figures 4 and 5). This risk stratification protocol has been translated into a worksheet for the physician (figure 4) that incorporates evidence-based risk factors for the Triad,16 ,17 ,46 and takes into account the magnitude (or severity) of risk, assigning a point value for risk factors in each Triad spectrum based on risk severity (low, moderate and high risk). This cumulative risk stratification protocol is then translated into clearance and return-to-play guidelines for the Triad based on the athlete's cumulative risk score (figure 5). Future research is needed to assess if implementation of a risk stratification model results in improved outcomes for female athletes with Triad disorders.

Female Athlete Triad: Clearance and Return-to-Play (RTP) Guidelines by Medical Risk Stratification. *Cumulative Risk Score determined by summing the score of each risk factor (low, moderate, high risk) from the Cumulative Risk Assessment (figure 4). Clearance/RTP status for athletes moderate-to-high risk for the Triad: provisional clearance/RTP—clearance determined from risk stratification at time of evaluation (with possibility for status to change over time depending on athlete's clinical progress); limited clearance/RTP—clearance/RTP granted, but with modification in training as specified by physician (with possibility for status to change depending on clinical progress and new information gathered); restricted from training/competition (provisional)—athlete not cleared or able to RTP at present time, with clearance status re-evaluated by physician and multidisciplinary team with clinical progress; disqualified—not safe to participate at present time. Clearance status to be determined at future date depending on clinical progress, if appropriate. It is the recommendation of the Consensus Panel that athletes diagnosed with anorexia nervosa who have a body mass index (BMI) <16 kg/m2 or with moderate-to-severe bulimia nervosa (purging >4 times/week) should be categorically restricted from training and competition. Future participation is dependent on treatment of their eating disorder, including ascertainment of BMI >18.5 kg/m2, cessation of bingeing and purging and close interval follow-up with the multidisciplinary team.
Risk stratification and the multidisciplinary team
Who are the members of the multidisciplinary team?
The Panel emphasised that the primary goal of the risk stratification protocol is to optimise health and reduce risk for injury and illness associated with the Female Athlete Triad. Best practice for outpatient management of the Triad can be accomplished with a multidisciplinary team consisting of the team physician, sports dietitian and often a mental health practitioner.102 Other team members may include the athlete's coach, athletic trainer, family members and other professionals, depending on the athlete's unique situation.
What are the recommendations for clearance and return to play based on risk stratification?
Athletes at low risk, by risk stratification for the Triad, can be fully cleared (assuming otherwise healthy). Referral to the multidisciplinary team for the low-risk athletes is not required, and can be individualised. Athletes at moderate risk for the Triad can be cleared provisionally or receive limited clearance. Provisional clearance would include clearance for full training/competition, with the understanding that the athlete will be compliant with the recommendations outlined by the multidisciplinary team. With limited clearance, the athlete is cleared, but there are limitations specified with the athlete's training and competition, based on the athlete's health status. The athlete may be able to participate progressively in more training/competition as health status improves, as specified and outlined by the multidisciplinary team. It is recommended that athletes at moderate or high risk for the Triad be referred by the team physician to the appropriate multidisciplinary team member(s) and that a follow-up be scheduled to assess progress and review results of any tests ordered.
Those athletes determined to be at high risk are restricted from training and competition. In this category, the athlete's status can be provisional or the athlete may be disqualified. If the healthcare team determines that the athlete may be able to reach the stated health goals, the status is provisional, and a plan is outlined by the multidisciplinary team for a given period of time, and re-evaluated as the athlete's health status improves, if appropriate. If the severity of risk is determined to be too high for athletic participation at the time of the preparticipation examination, and prognosis determined to be poor, the athlete is disqualified and clearance/return to play re-evaluated with clinical progress, if appropriate. In such instances, the athlete may require more intensive outpatient treatment, inpatient hospitalisation or residential care prior to reassessment for clearance and return to play.
Similar to the FRAX algorithm developed by the WHO230 ,231 that uses clinical risk factors with or without BMD to assist with clinical decision-making in postmenopausal women and men to reduce fracture risk, it is hoped that this risk stratification developed for the Triad will assist healthcare providers working with female athletes to minimise risk associated with the Triad disorders. With ongoing research, updates to the risk stratification can be implemented in hopes of guiding treatment and decision-making for clearance and return to play.
Treatment contracts
How does the team physician utilise contracts?
Athletes in the moderate-risk and high-risk categories should receive a written contract that is reviewed and presented to them by the team physician after their initial evaluation. Although a verbal contract may be sufficient, the Panel recommends a written contract. The goal of the written contract is to specify the criteria necessary for ongoing or future clearance and return to play for the female athlete with the multidisciplinary team members, and to ensure a shared understanding of how the clinical status of the athlete will be followed with each member of the multidisciplinary team.
The team physician coordinates the treatment goals with each multidisciplinary team member, and includes the specific recommendations in the contract, in addition to the requested frequency of visits and expectations for each team member. The team physician then reviews the recommendations with the athlete, and answers any questions. In the case of the written contract, athlete and team physician sign the contract after it is discussed. (Please see online supplementary appendix for an example of a written contract for the Female Athlete Triad, which can be modified based on the athlete's clearance status.)
Decision-based model for return to play
What other factors play a role in clearance and the return-to-play decision?
In addition to risk stratification, the team physician must take into account the athlete's unique situation in making the final decision for clearance and return to play.232 The decision-based return-to-play model developed by Creighton et al233 points out the complexities in return-to-play decision-making. There are medical factors and severity of risk considerations that need to be considered in the return-to-play decision. In addition, the return-to-play decision also involves consideration of sport risk modifiers (such as type of sport and competitive level) and willingness of the athlete to participate in her treatment. Athletes participating in leanness sports, for example, have been found to be at higher risk for Triad disorders.234 Although low BMI and/or low body weight are included as risk factors in the Triad risk stratification table (figure 3), it is important to recognise that low body fat is not independently associated with menstrual dysfunction, low BMD and stress fracture.19 ,235 It is not the recommendation of the expert panel convened to systematically address body fat in female athletes, but to consider low body fat as a consequence of inadequate dietary intake and/or excessive exercise, and address those issues in the continuing effort to optimise EA, restore normal reproductive function and promote bone health. A decision-based model for the Triad, modified with permission from Creighton et al,233 illustrates some of the complex issues that need to be considered prior to the decision for clearance and return to play of the female athlete (figure 6).

{kind=link}
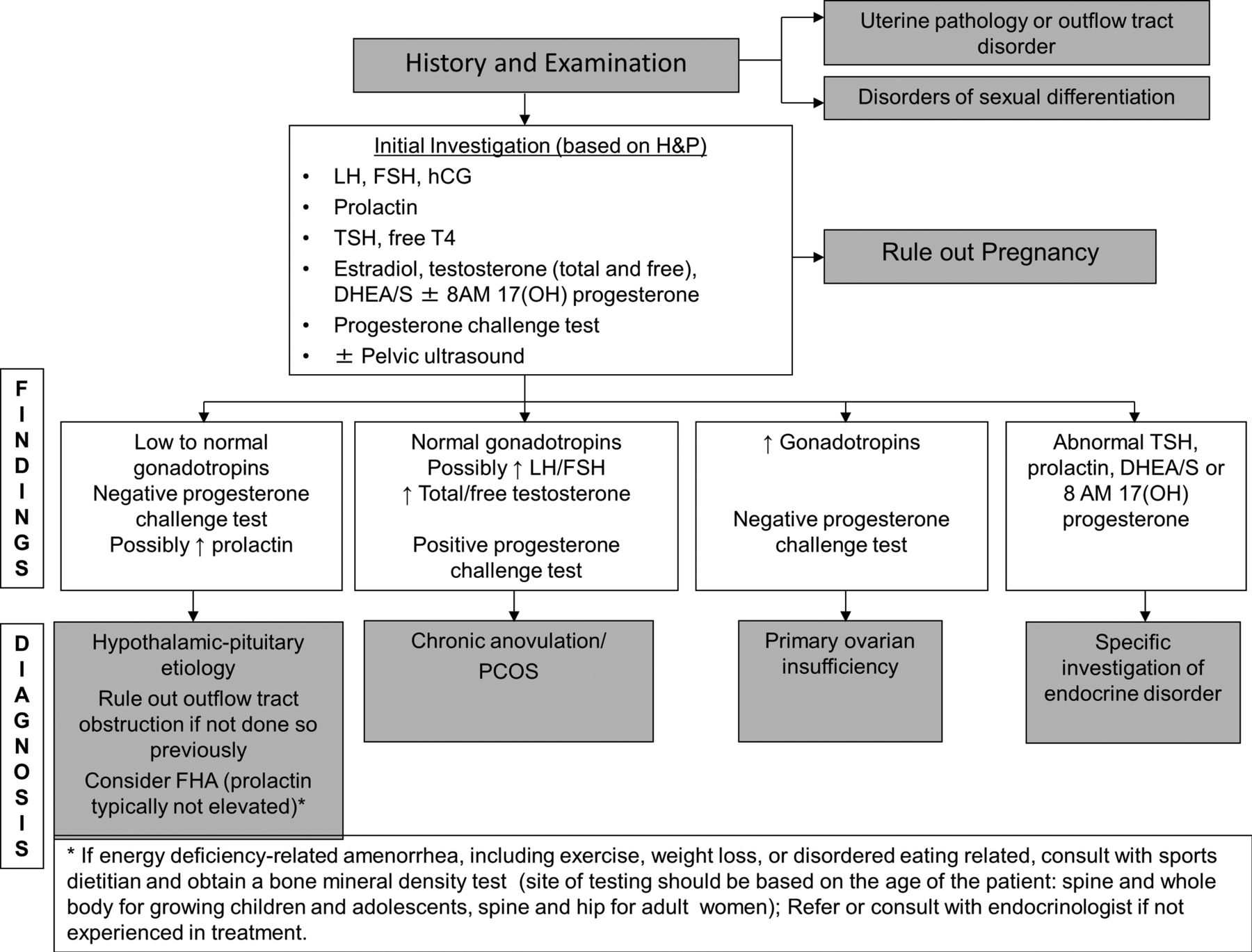{kind=link}
{kind=link}
{kind=link}
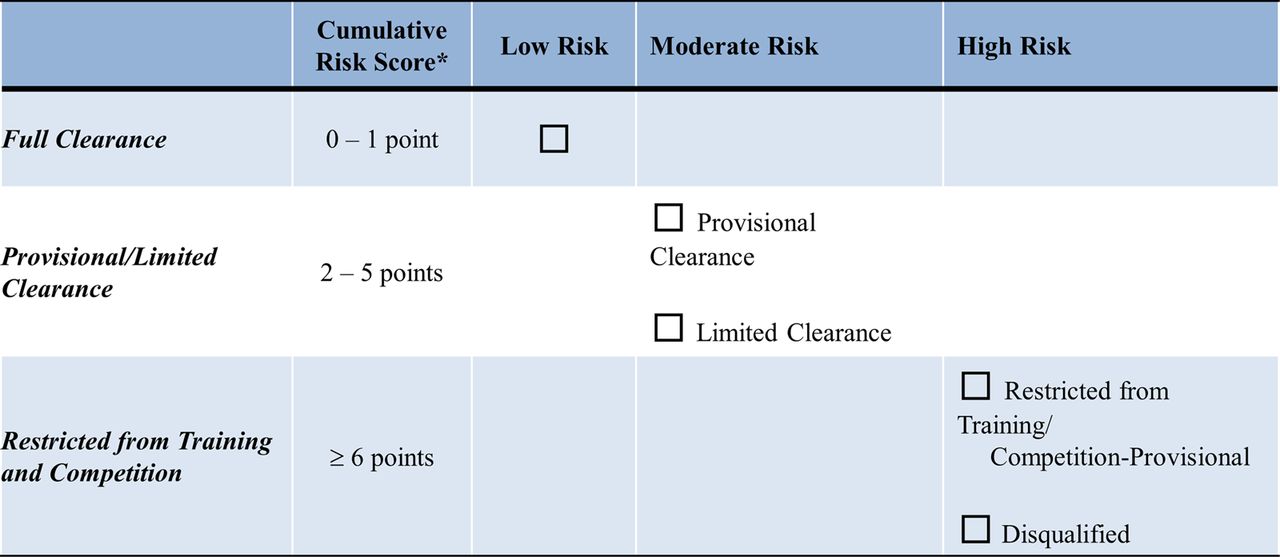{kind=link}
{kind=link}
Decision-Based Return-to-Play (RTP) Model for the Female Athlete Triad. *RTP decision is determined by the primary care or team physician, and is based on a complex and comprehensive synthesis of health status, cumulative risk assessment, participation risk, sport and decision modifiers. 25(OH) Vit D, 25-hydroxyvitamin D; BMI, body mass index; BP, blood pressure; CBC, complete blood count; DXA, dual-energy X-ray absorptiometry; ED, eating disorder; OCD, obsessive compulsive disorder; TFTs, thyroid function tests; TSH, thyroid stimulating hormone; modified with permission from Creighton et al. 233
In the evaluation of health risk and participation risk, an important consideration is also the age of the athlete. The preadolescent and adolescent athlete has more vulnerability to physeal and other skeletal injuries, especially during periods of rapid growth. Adolescence is a period of rapid bone mineral acquisition.45 ,149 ,220 Inadequate EA and menstrual dysfunction may result in a delay of bone mineralisation that lags behind bone linear growth.236 The mechanical stresses from repetitive loading in this population may increase susceptibility to fracture147 in an already vulnerable area of bone, which may have potentially catastrophic consequences. Case reports of devastating displaced femoral neck stress fractures in female adolescent athletes with Triad disorders are concerning and suggest that better screening and management of the Triad is imperative to minimise future fracture risk and potential for life-long disability.219 ,237 ,238 Furthermore, prospective studies are needed to identify thresholds of physical activity and sport beyond which may be detrimental to bone health.
Similar scrutiny should be directed towards athletes meeting DSM-V criteria for an ED.81 While the presence of an ED is considered a high-risk attribute in the Cumulative Risk Factor Assessment (figure 3), it should be noted that patients with EDs have a higher risk of premature mortality when compared with individuals with other psychiatric diagnoses, and that is especially true for those with anorexia nervosa.239 Risk factors associated with a higher premature mortality rate among individuals with anorexia nervosa include: (1) longer duration of illness (>10 years); (2) lower BMI (<16 kg/m2); (3) concurrent alcohol abuse and (4) poor social adjustment.239–241 It is the recommendation of the Consensus Panel that athletes diagnosed with anorexia nervosa who have a BMI <16 kg/m2 or with moderate-to-severe bulimia nervosa (purging >4 times/week)81 should be categorically restricted from training and competition. Future participation is dependent on treatment of their ED, including ascertainment of BMI >18.5 kg/m2, cessation of bingeing and purging and close interval follow-up with the multidisciplinary team.241
In some cases, participation in sport becomes fully integrated with an ED and isolation and treatment of the ED, such that resuming participation in the sport is not a realistic goal for the short or moderate term. It is important that EDs be recognised as a serious mental illness and that their impact and potentially long and pernicious course not be underestimated.
Finally, it is of paramount importance that the team physician has the ultimate say in the decision-making process for clearance and return to play.229 ,232 ,242 Although the team physician has this authority to make the final decision, the decision is often the product of consultation with the multidisciplinary team, and other concerned parties. The physician must always have the athlete's health and safety as the first priority in the decision-making process, which should supersede all other pressures or circumstances that may arise.
Conclusion
Young girls and women with the Female Athlete Triad have significant health risks. Historically, many of these athletes have been cleared for sport participation without appropriate evaluation, management and treatment. Similarly, after medical illness or injury, athletes with the Triad often return to play prematurely, and without adequate treatment and follow-up. It is the team physician's responsibility to ensure that each and every athlete who is cleared for participation in sport or returning to play after an injury or illness return only when it is determined safe to do so. The 2014 Female Athlete Triad Coalition Consensus Statement on Treatment and Return to Play of the Female Athlete Triad Expert Panel has proposed an evidence-based risk stratification point system that takes into account the magnitude of risk to assist the physician in decision-making regarding sport participation, clearance and return to play. Guidelines are offered for clearance categories, management by a multidisciplinary team and implementation of treatment contracts. Future research is needed to study whether risk stratification, clearance and return-to-play guidelines are an effective means of optimising health and reducing risk for injury and illness for the Triad.
Acknowledgments
The authors and expert panel would like to acknowledge the contributions of Jim Whitehead, Executive Vice President and CEO, American College of Sports Medicine; Mimi Johnson, MD; and Tyler Wadsworth, MD. Their encouragement, expertise and support contributed to the successful development of this document.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Expert Panel Members Michelle Barrack, PhD, RD, California State University Northridge, Northridge, California, USA; Louise Burke, PhD, Australian Institute of Sport, Australia; Barbara Drinkwater, PhD, FACSM, Washington, USA; Connie Lebrun, MD, University of Alberta, Edmonton, AB Canada; Anne B Loucks, PhD, Ohio University, Athens, Ohio, USA; Margo Mountjoy, MD, McMaster University, Guelph, Ontario Canada; Jeanne Nichols, PhD, San Diego State University, San Diego, California, USA; Jorunn Sungot Borgen, PhD, Norwegian School of Sport Sciences, Oslo, Norway.
-
Contributors All authors have contributed substantially to the manuscript and have been involved in designing and drafting the manuscript. MJDS, AN, EJ and MM planned, constructed and drafted the article and were also involved in revising the manuscript. NIW, MO, MG and GM were involved in drafting, reviewing and editing the manuscript. RJM and JCG were involved in writing and revising the manuscript and creating tables and figures. Members of the invited Expert Panel participated in Consensus Conference meetings held in June 2012 and June 2013 as well as provided the authors with guidance and feedback on the consensus process and manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.