Article Text

Abstract
Introduction Greater trochanteric pain syndrome (GTPS) is common and can cause significant pain and dysfunction.3 While both trochanteric bursae and gluteal tendons have been implicated in the pathology,2,6 the underlying pathology remains controversial. Studies reporting on pathology are limited by sample size or methods, including lack of comparison specimens. Thus the aim of this study was to clarify the role of tendon and bursa pathology in GTPS.
Methods Tendon and bursa specimens were obtained from 64 participants: 35 with GTPS and 29 control participants. Specimens were evaluated by a minimum of two investigators via light microscopy for histopathological and morphological differences. Immunohistochemistry methods were used to evaluate macrophages (CD68), inflammatory cells (CD45) and substance P. Tendon was evaluated used the Bonar score3. Bursa specimens were evaluated via a semi-quantitative scoring system. Second harmonic generation microscopy, via multiphoton excitation fluorescence (MPEF) was used to illustrate morphological findings (Figure 1).
Results Higher levels of pathology were found in specimens from participants with GTPS vs controls. The stroma of the bursa score, mean (SD): GTPS 4.18 (1.65) vs. control 2.53 (1.61), p = 0.051. Bonar (tendon) score, mean (SD): GTPS 12.65 (2.0) vs. control 10.43 (4.83), p = 0.04. There was a higher frequency of SubP in bursa (9/12 vs 6/16, p = 0.047), but not the tendon (8/12 vs. 8/15, p = 0.484) of specimens from participants with GTPS vs controls. There was no evidence of increased frequency of macrophages or other inflammatory cells in the bursa or the tendon specimens from either group.
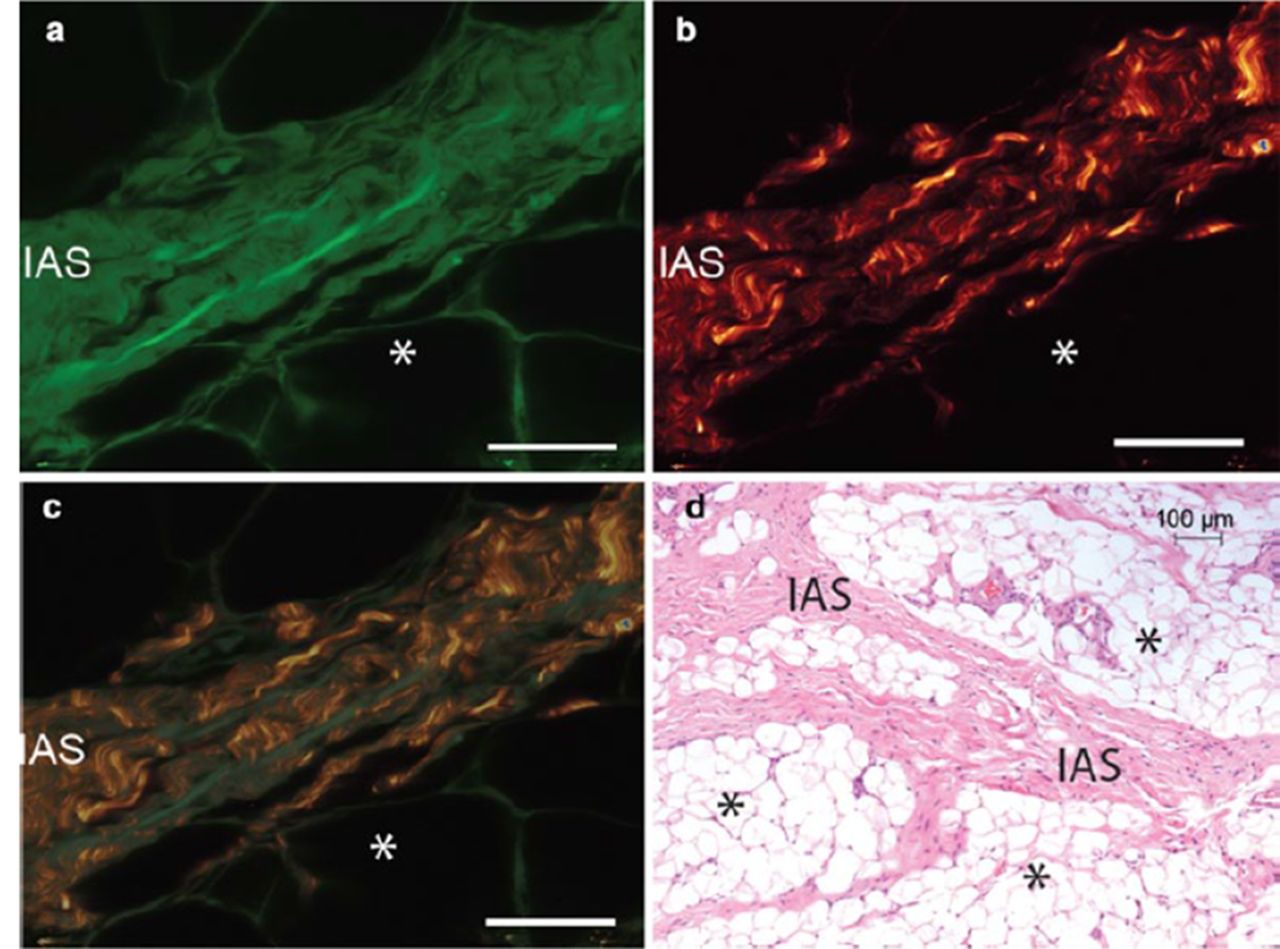
Intra adipose septa were identified and found to be present more frequently in the stroma of bursa specimens of participants with GTPS than controls (27/31 vs 15.27, Fisher exact: p = 0.008), (Figure 1).

{kind=link}
Inter-adipose septa (IAS) were seen more frequently in bursa specimens from people with GTPS than controls. Multiphoton excitation fluorescence (MPEF) (A) demonstrates a highly organised structure; high levels of collagen are seen via (B) and non-collagen fibrillar structures are seen in (C). H and E staining further demonstrates the IAS (D). (a – c scale bar = 25.4 µm, d = 100 µm)
Discussion Tendon pathology present in both groups, with higher degree of pathology in GTPS. More extensive bursa pathology was seen in the GTPS group, along with a higher frequency of SubP in the bursae from the GTPS than the OA group. This may explain why bursectomy appears to be a successful treatment for some people with GTPS.1
The IAS has previously reported in rats,5 but not to our knowledge, in humans. This well organised structure may play a role in bursa stabilisation and shear mitigation. Pathologically it may reduce the ability of the bursa stroma to mitigate compression forces over the tendon.
References
Baker, et al. Arthroscopy. 2007;23:827–832
Connell, et al. Eur Radiol. 2003;13:1339–1347
Fearon, et al. J Arthroplasty. 2014;29:383–386
Fearon, et al. J Sci Med Sport. 2013;doi: 10.1016/j.jsams.2013.07.008
Shaw, et al. J Anat. 2007;211:436–443
Spear, et al. Surg Clin N Amer. 1952;32:1217–1224