Article Text

Abstract
Introduction Muscle power of the Plantarflexors has been shown to be a prospective risk factor for Achilles Tendinopathy (AT).1 Several studies have shown associations between Achilles tendinopathy and Plantarflexor power, but little thought has been given to how the individual muscles of the Triceps Surae are affected.
Aim – Compare the Triceps Surae power of runners with and without AT.
Method 41 runners with AT and 27 runners without a history of AT (control group) have participated in this study. Plantarflexor muscle power was measured during concentric and eccentric muscle contractions at 90º/sec using an Isokinetic dynamometer. Testing utilised a knee extended position (both Gastrocnemius and Soleus) and an 80º knee flexed position (significantly inhibiting Gastrocnemius).2,3
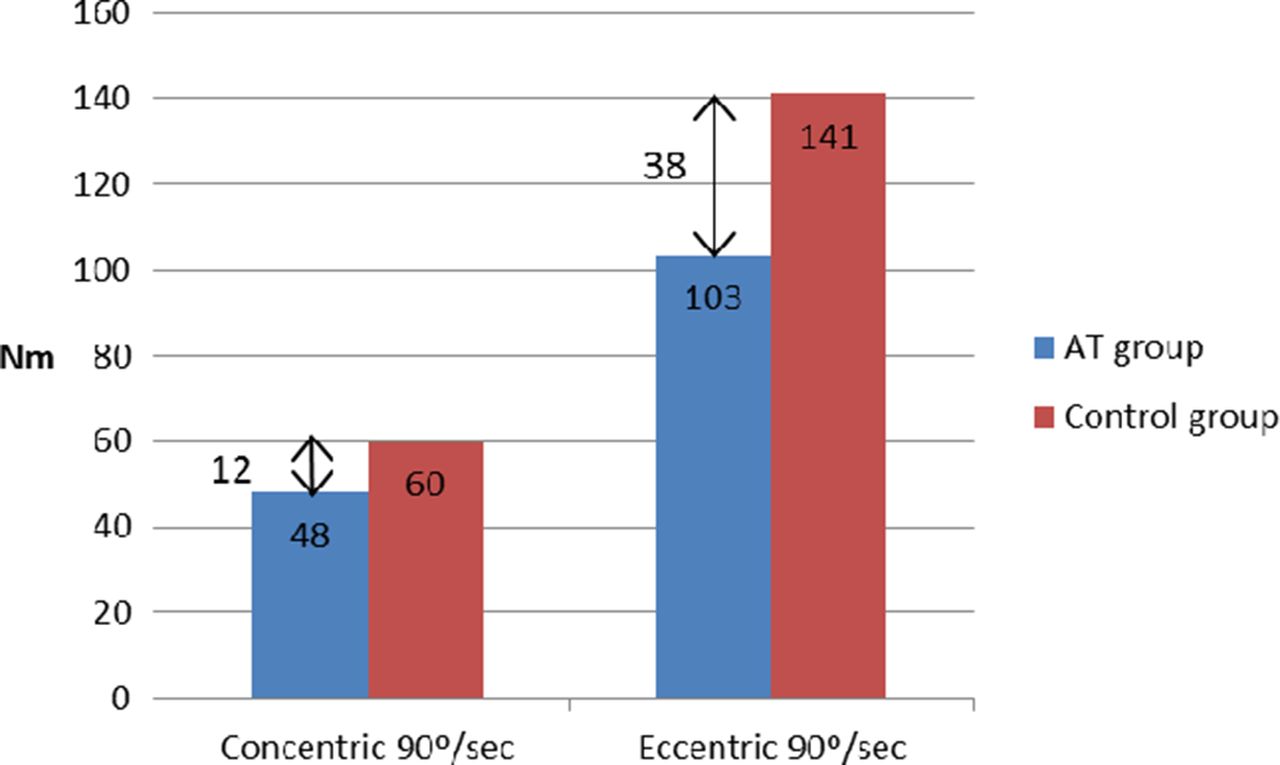
Results Independent t tests revealed statistically significant differences between healthy controls and participants with AT for both test speeds and positions (p = 0.004 for concentric 90º/sec in knee flexion, p ≤ 0.001 for all other test speeds and positions).
Discussion This study shows that participants with AT have weaker Plantarflexors than healthy runners. It also shows that the deficits in power appear similar whether testing was performed with knee extension or flexion, since Gastrocnemius does not contribute significantly to force generation in knee flexion it seems feasible that the Soleus is responsible for the majority of observed deficits in both positions.
Pain was not reproduced during testing for any individual and therefore did not limit performance.
It is possible these neuromuscular deficits are due to central motor inhibition or potentially pre-existing weakness. Resolution of these muscle deficits may be essential to return to normal function, it is unclear whether normal rehabilitation successfully resolves these deficits.

The peak Plantarflexor power for participants with AT and the control group in knee extension (both Gastrocnemius and Soleus active)
{kind=link}
{kind=link}
he peak Plantarflexor power for participants with AT and the control group in knee flexion (Gastrocnemius significantly inhibited)
Conclusion Weakness of Soleus maybe responsible for the majority of the deficits observed in participants with AT. Further work needs to determine how current clinical interventions alter these deficits.
References Lauber, et al . Physiological reports. 2014;2, doi:10.14814/phy2.12044
Mahieu, et al. Am J Sports Med. 2006;34:226–235
Reid, et al. Physical Therapy in Sport. 2012;13:150–155