Article Text

Abstract
Introduction Musculoskeletal pain (MSK) is known to cause neuroplasticity and changes to muscle representation and motor control.1 Patellar tendinopathy (PT) is a MSK pain that can persist for many years and causes dysfunction in the patellar tendon. Local tissue changes fail to explain tendon pain because pathology may or may not cause pain. Importantly, it is not known how the central nervous system modulates or interprets tendon pain and whether it is similar to other chronic/persistent pain conditions.
Corticospinal excitability is an important determinant for muscle function and differences between healthy and tendinopathic participants may correlate with altered muscle function associated with tendinopathy. The corticospinal changes in people with tendon pathology and no pain may contribute to our understanding of the “chicken or the egg” in pathology and pain. This study investigated whether there were corticospinal excitability differences between people with and without tendon pain and tendon pathology.
Methods Thirty jumping athletes (n = 6 women, n = 24 men) aged over 18 years with and without PT participated in the study. PT was diagnosed clinically. Ultrasound was used to assess for the presence of tendon abnormality.
Objective measures of SLDS pain (numerical rating score out of ten) and maximal voluntary isometric leg extension torque were recorded. The VISA-P questionnaire was administered. Single pulse transcranial magnetic stimulation (TMS) was applied over the motor area projecting to the quadriceps muscle group to obtain measures of corticospinal excitability. Surface EMG was placed on the rectus femoris muscle to record the motor evoke potentials (MEP).
Stimulus-response curves were obtained and the slope and peak values were used to establish the strength of projection. Results of tendinopathic and healthy individuals were compared. Within participant analysis was conducted to investigate the cortical changes associated with either unilateral or bilateral pain. People with tendon pathology were analysed separately to controls to determine the effect of pathology on corticospinal excitability.
Results Pilot data only (n = 11) is provided at this time with a full data set currently being analysed (n = 30). The mean VISA-P was 97.5 for healthy (n = 4) and 57.75 for people with PT (n = 7). The mean SLDS was 7.5/10 for people with PT.
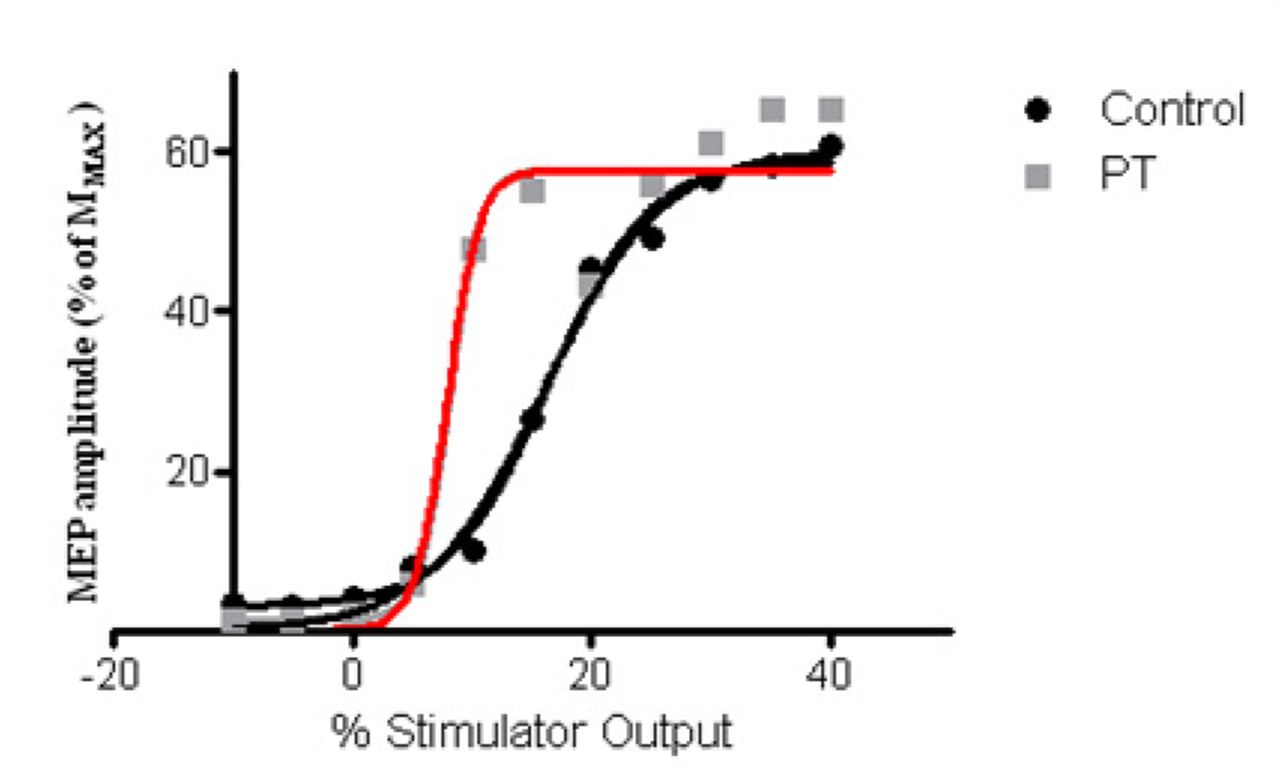
PT increased cortical excitability, evidenced by a steeper slope in the stimulus response curve of people with PT compared with healthy people (p = 0.029, Cohen’s d = 3.08). Figure 1 shows an example of a control participant and a participant with PT.
{kind=link}
Stimulus response curves shown for a control participant and a participant with pt. the y axis is the motor evoked potential as a percentage of Mmax obtained by direct stimulation of the femoral nerve
The x axis is the percentage stimulator output.
These changes were positively related to symptom duration (r2 = 0.57) – the longer the duration of symptoms, the more pronounced the increase in cortical excitability.
Discussion People with PT have increased corticospinal excitability affecting motor control. Differences identified indicate that symptom duration impacts cortical excitability. It may be important to measure and consider these cortical changes in the rehabilitation of people with PT.
Reference 1 Tsao H, Galea M, Hodges P. Eur J of Pain 2010;14:8,832–839