Article Text

Abstract
Objective Hypertension is reported to be the most prevalent risk factor for cardiovascular disease in elite athletes. We aimed to review blood pressure (BP) and prevalence of hypertension in different elite athletes, and study whether there was an association between high BP and left ventricular hypertrophy (LVH).
Methods A systematic review of studies reporting BP in athletes using search strategies developed for PubMed and EMBASE, including only studies with ≥100 participants. We collected data on BP, prevalence of hypertension, LVH and methods of BP measurement.
Results Of 3723 records identified, 51 met the inclusion criteria. These included men and women (n=138 390), aged mostly between 18 and 40 years, from varied sports disciplines. Mean systolic BP varied from 109±11 to 138±7 mm Hg and mean diastolic BP from 57±12 to 92±10 mm Hg. Strength-trained athletes had higher BP than endurance-trained athletes (131.3±5.3/77.3±1.4 vs 118.6±2.8/71.8±1.2 mm Hg, p<0.05), and there was a trend towards a higher BP in athletes training ≥10 h compared with others (121.8±3.8/73.8±2.5 vs 117.6±3.3/66.8±6.9, p=0.058), but overall there was no significant difference in BP between athletes and controls. The prevalence of hypertension varied from 0% to 83%. Some studies showed an association between high BP and LVH. Measurement methods were poorly standardised.
Conclusions BP and prevalence of hypertension in athletes varied considerably partly because of variations in methodology, but type and intensity of training may contribute towards higher BP. High BP may be associated with LVH.
- Athletics
- Cardiology
- Cardiovascular
Statistics from Altmetric.com
What this study adds?
-
There was no evidence that blood pressure (BP) was lower in athletes than in controls. A number of studies showed a higher BP in athletes. The prevalence of hypertension in athletes could not be determined reliably because of different definitions of hypertension and poorly standardised methods of BP measurement.
-
A positive linear association between high BP and left ventricular hypertrophy was observed in athletes, but confounding factors may have played a role.
-
Future studies should be designed to determine more precisely the prevalence, determinants and prognostic significance of hypertension in athletes.
Introduction
In Western countries, the prevalence of hypertension has been reported as 14.4% and 21.2% in men aged 20–29 and 30–39 years, respectively, and as 6.2% and 9.9% in women in the same age group.1 High blood pressure (BP) at a young age predicts cardiovascular mortality and morbidity decades later.2 ,3
High BP is the most common abnormal finding during preparticipation cardiac screening of athletes.4–8 The prognostic significance of high BP in athletes is unknown, but still athletes with BP <160/100 mm Hg are given the license to continue with sport participation if they have no signs of end organ damage, such as pathological left ventricular hypertrophy.9 Increased left ventricular mass is considered as subclinical organ damage in people with hypertension.10 ,11 As several studies have demonstrated increased left ventricular mass and increased left atrium size in athletes,12 it is possible that high BP may be a contributing factor13 ,14 that may also link to the increased risk of atrial fibrillation in endurance athletes.15–17 Hence, there is increasing interest in BP in athletes.14 ,18 ,19 BP measurement during preparticipation screening of athletes should be performed according to ‘best clinical care’,20 as outlined in the European Society of Cardiology's guidelines, with hypertension defined as systolic BP (SBP) ≥140 mm Hg and/or diastolic BP (DBP) ≥90 mm Hg after repeated measurements.21 We aimed to review BP and prevalence of hypertension in different athletes, and study the association between increasing BP and left ventricular hypertrophy.
Methods
Literature search
We performed a systematic review of studies reporting BP in athletes by using a comprehensive search strategy developed for PubMed and EMBASE (see online supplementary material). The medical subject headings and text words were: ‘Athlete’, ‘Sport and Professional’, ‘Exercise Test’ and ‘Sudden Death’, combined with ‘Blood Pressure’ or ‘Hypertension’. The electronic search was restricted to studies published before 6 April 2014. In addition, we manually searched reference lists of reviews and original study articles, and our own archive.
Inclusion and exclusion criteria
We searched for studies of athletes that reported BP or prevalence of hypertension, using the studies’ own definitions of hypertension. We included studies of ≥100 athletes, with mean or median age between 18 and 40 years, of any epidemiological design (with or without follow-up, and with or without controls), and reported in English language. We excluded studies that were only presented as conference abstracts. If there were more than one publication from the same group, we used the record with most participants, or the newest, if the number of participants were the same. When in doubt, we contacted the corresponding authors.
Outcome variables
The primary outcome variable was BP or prevalence of hypertension in different categories of athletes (defined by gender, ethnicity, sports discipline or level of athletic activity). Secondary outcome variables were (1) method for measurement of BP and (2) association between BP and left ventricular hypertrophy (determined by left ventricular mass or relative wall thickness on echocardiography or by voltage criteria on ECG).
Extraction of data
All data were extracted by one reviewer (CBI) and checked by another reviewer (HMB), using a standardised data extraction sheet.
Statistical analysis
Differences between subgroups of athletes were analysed using t tests for continuous variables. Data are presented as mean with SD. A p<0.05 was considered statistically significant and all tests were two-tailed. The statistical analyses were conducted using SPSS (PASW Statistics 21; IBM Corporation 2013, Armonk, New York, USA).
Results
Study selection
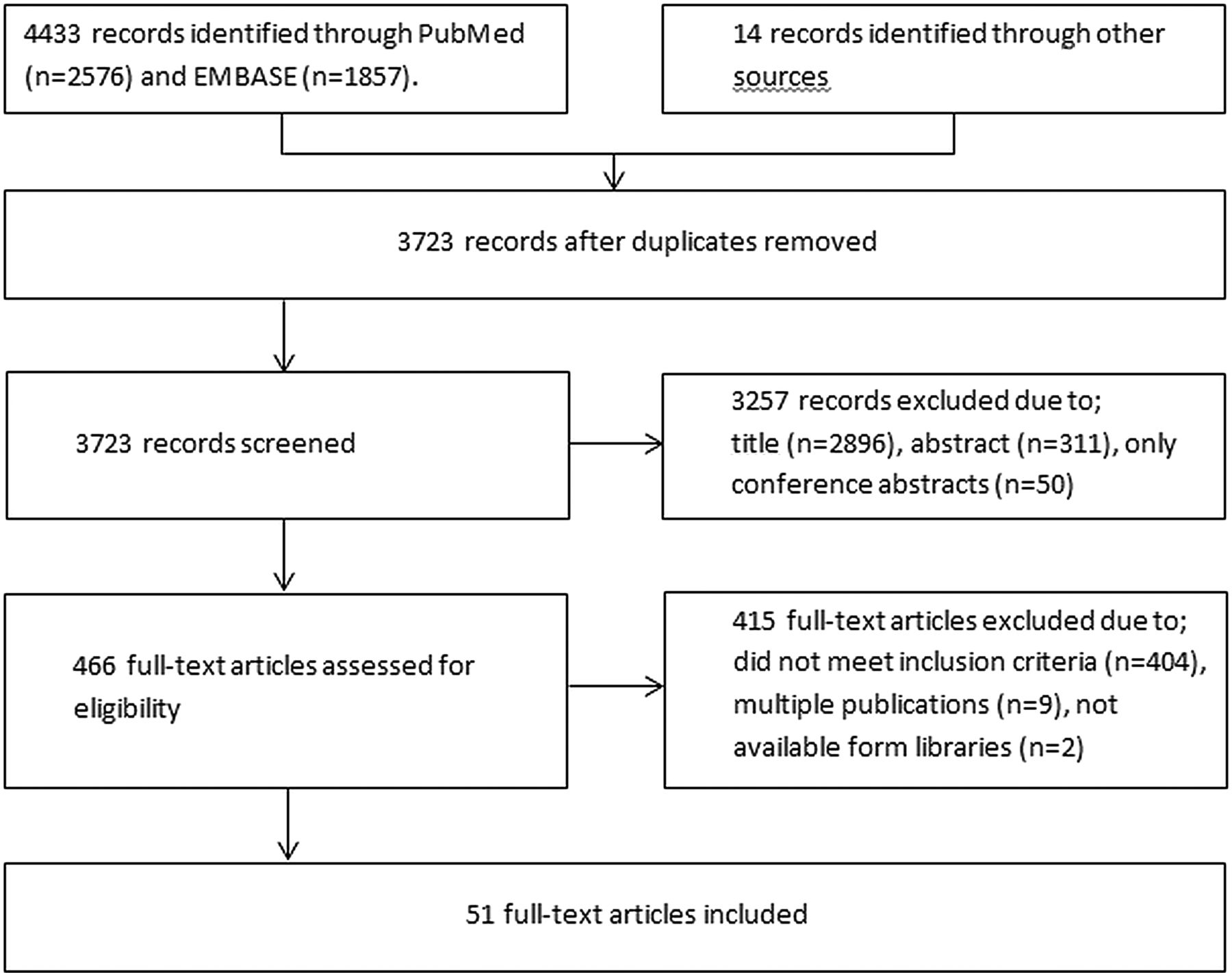
The searches retrieved a total of 4433 records (figure 1). After addition of studies from other sources and removal of duplicates, 3723 records remained. Screening of titles and abstracts excluded 2896 and 361, respectively. Another 404 studies did not meet the inclusion criteria, 9 were duplicate reports, and 2 studies were not available. The remaining 51 studies were included in the review.

Flow chart illustrating search strategy.
Study characteristics
Table 1 shows characteristics of the 51 studies, including a total of 138 390 athletes, with a median number of 434 athletes (range 10022–42 386 athletes23). Sixteen studies included non-athletes as controls and the median number of controls was 176 (range 26–9997). The mean or median age of the athletes in all studies was between 18 and 40 years, and about half of the studies had participants within this range only; however, several studies included participants with an age outside this range. Twenty studies included males only and across the 31 studies of both genders, 72.5% were males.
Study characteristics
Most studies (28) included athletes from different sports disciplines, but 16 included athletes from only one discipline, eg, soccer (4),13 ,24–26 American football (3),27–29 triathlon (2)30 ,31 and long distance running (2);16 ,32 other studies classified sports disciplines as either endurance sports, strength sports or a mixture of the two (table 1). The athletes’ level of competition was described in 50 studies and ranged from participation in amateur sport to the Olympic Games. Hours of training per week or previous years of vigorous training were given in 24 studies, and ranged from 4 to 28 h a week and from 2 to 30 years, respectively.
BP in athletes
Table 2 shows BP and prevalence of hypertension in the same studies. Among the 34 studies that reported BP, two-thirds had BP in the prehypertensive range (SBP ≥120–139 and/or DBP ≥80–89 mm Hg).33 Mean SBP varied from 109±11 mm Hg (intercollegiate female college athletes (mean age 20 years))34 to 137.9±7.1 mm Hg (Italian male strength sports athletes (mean age 27.2 years)).35 Mean DBP ranged from 56.9±11.5 mm Hg (young college level athletes in the USA (mean age 18.4 years))36 to 92.2±9.6 mm Hg (male Chinese strength sports athletes with mean body weight 130 kg (mean age 21.7 years)).34 No studies reported ambulatory BP measurements.
Blood pressure and prevalence of hypertension
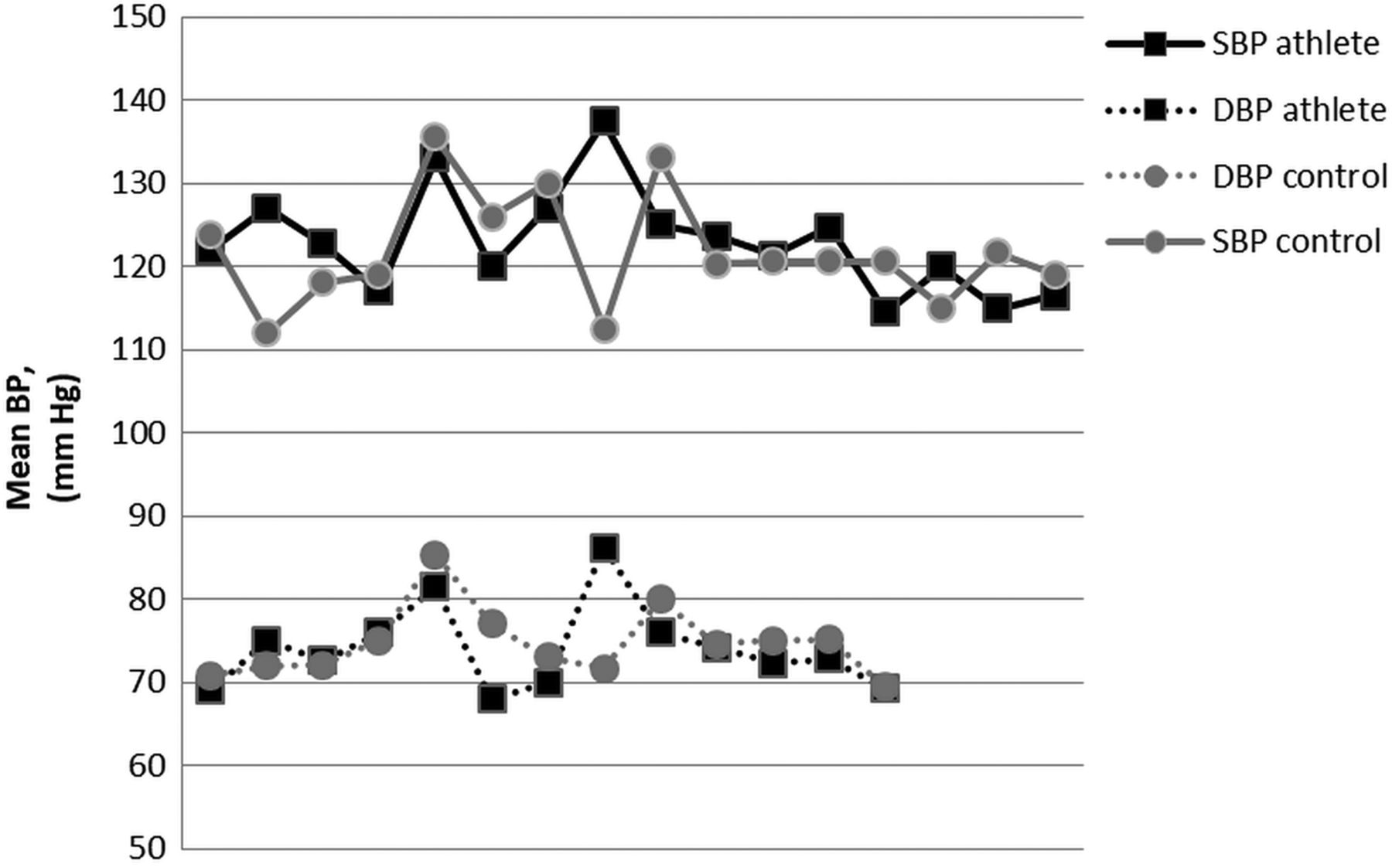
Among the 16 studies that included non-athletes as controls, BP was lower in athletes than in controls in 9 studies and higher in athletes in 7 studies (figure 2). Only 3 of the 16 studies reported prevalence of hypertension in controls and 2 studies found more hypertension among athletes than controls. Overall, there was no significant difference in BP between athletes and controls.
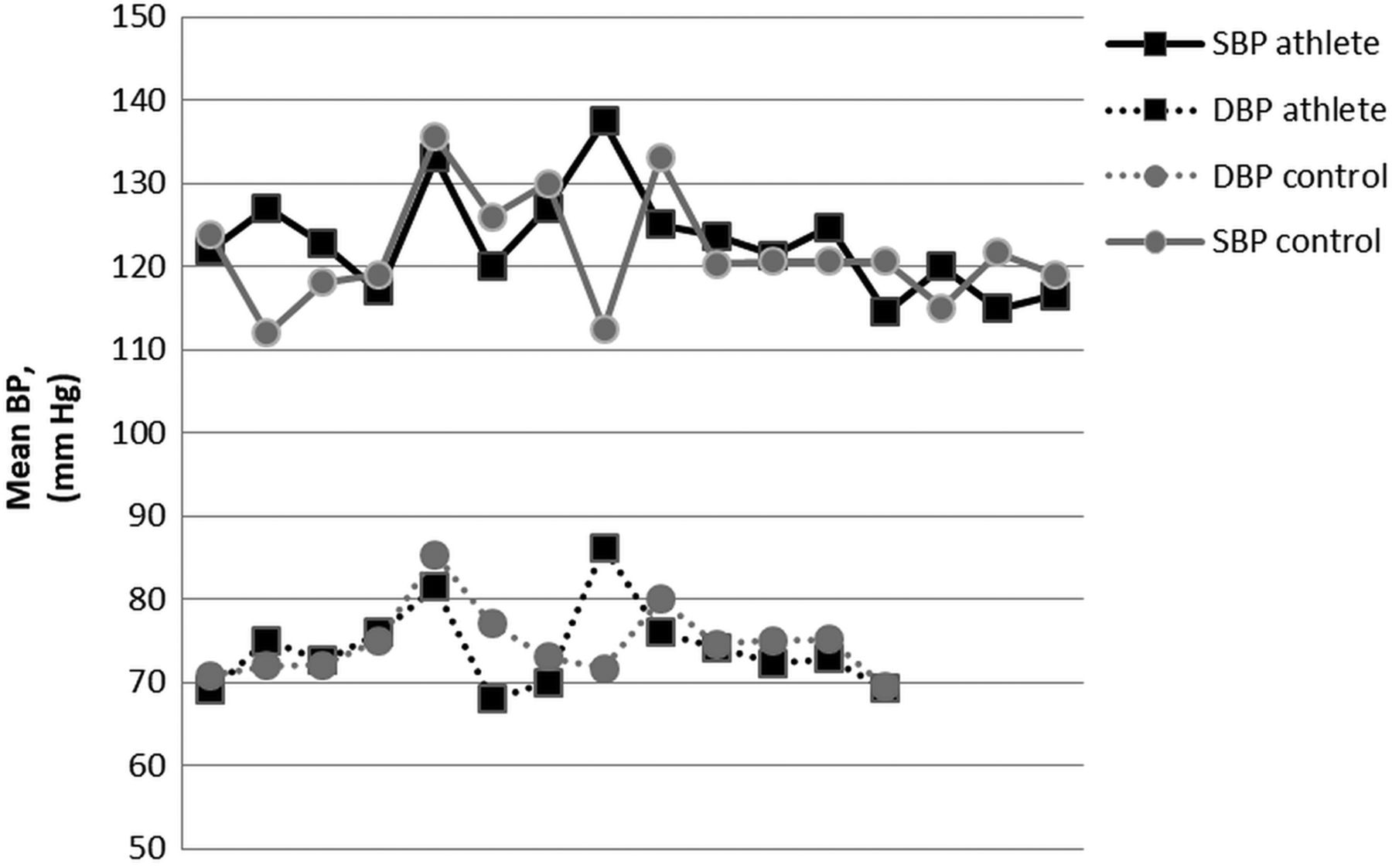
Mean systolic blood pressure (SBP; continuous line) and diastolic blood pressure (DBP; dotted line) in athletes (black squares) and controls (grey circles).
Figure 3 shows the mean BP in different categories of athletes. Males had significantly higher BP than females (121.2±4.5/75.1±2.9 vs 113.5±2.9/71.9±2.6 mm Hg, p<0.05), but there was no significant difference in SBP between white and black athletes. We found that strength-trained athletes had higher BP than endurance-trained athletes (131.3±5.3/77.3±1.4 vs 118.6±2.8/71.8±1.2 mm Hg, p<0.05), while there was a trend towards higher BP in athletes training ≥10 h/week compared with those training <10 h/week (121.8±3.8/73.8±2.5 vs 117.6±3.3/66.8±6.9 mm Hg, p=0.058). There was no major difference between American football, soccer, triathlon and long distance running (figure 4).

Blood pressure (BP) in relation to gender, ethnicity, type of training and hours of training per week.

Blood pressure (BP) in different sports disciplines.
Prevalence of hypertension in athletes
Hypertension was defined in 11 different ways in the 25 studies presenting a definition (table 2). The most often used criteria for hypertension ranged from SBP ≥140 or DBP ≥90 mm Hg to BP>140/90 mm Hg. The lowest cut-off value for hypertension was BP ≥130/85 mm Hg37 and the highest cut-off value was ≥160/95 mm Hg.27 Three studies also used antihypertensive medication to define hypertension,18 ,29 ,34 one accepted self-reported hypertension18 and one only included participants with BP≤120/80 mm Hg.38
The prevalence of hypertension varied from 83%34 to 0% (table 2).39 ,40 The prevalence of hypertension was lower in studies that were restricted to athletes within the age range 18–40 years and six studies excluded patients with high BP, mostly >140/90 mm Hg.38–43
Method of measurement of BP in athletes
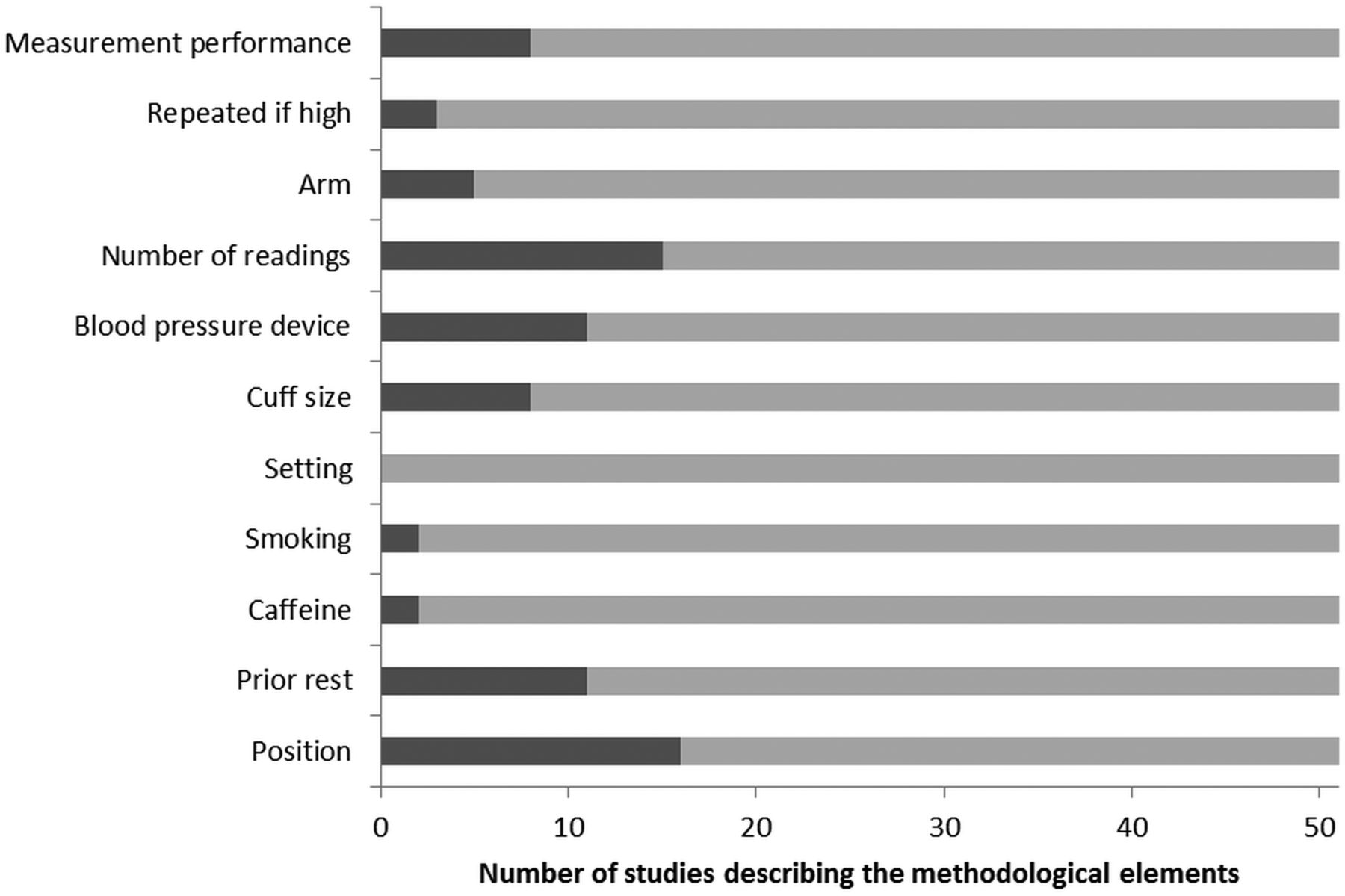
Some descriptions of measurement methods were present in 21 studies (figure 5; see online supplementary figure S3). BP was measured in the sitting position in 10 studies and in a supine position in 6 studies. At least 5 min of rest prior to BP recordings was required in 11 studies, while only 4 informed about time from physical activity to BP measurement.6 ,13 ,44 ,45 Athletes abstained from caffeine and/or smoking prior to BP recordings in two studies6 ,44 and no studies informed about the physical environment where the BP measurements took place. Only eight studies reported whether an appropriate cuff size was used. In the eight studies using a ‘standard’ mercury sphygmomanometer, the method of measurement performance was reported in three studies.45–47 Only the three studies that used an automated BP device reported the device type and manufacturer.13 ,26 ,29 A single measurement was used in five studies, but repeated in three of these if BP was high. The lowest of these values was registered in two studies18 ,48 and the highest in one.27 BP was recorded two and three times in six and four studies, respectively, and there was a significant difference in SBP between one and two BP recordings (127±4.7 vs 118±4.0 mm Hg, p<0.05). Choice of arm for measurement was presented in five studies and no study measured BP in both arms. Three studies recommended repeated BP recordings on a separate occasion if the BP was elevated. Only one study referred athletes with elevated office BP to ambulatory BP measurement.49
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of studies describing each of the recommended elements in blood pressure measurements.
Association between BP and left ventricular hypertrophy
Three of the four studies relating high BP to left ventricular hypertrophy showed a significant positive linear association, either between BP and indexed left ventricular mass,13 between resting SBP and left ventricle mass and left ventricle wall thickness,49 or between SBP and the RaVL lead in ECG.29 One study found no association between SBP and relative wall thickness.30
Discussion
The most striking finding in this review was that the methods of BP measurement in athletes were poorly standardised and varied widely. The Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure states that at least two measurements shall be made and the averaged recorded,33 and the European guidelines state that BP shall be measured three times after 5–10 min rest in the sitting position and the mean of the last two measurements shall be registered.21 The IOC has recommended BP recordings from both arms during preparticipation cardiac screening.50 All guidelines also recommend use of ambulatory BP measurements, but nearly all studies in our review were negligent to all these recommendations, as was a study among general practitioners in the UK.51
Given this background, it was difficult to give an estimate of BP or prevalence of hypertension in athletes. Naturally, the prevalence will be dependent on the definition of hypertension and varied from 0% to 83% in a subgroup of heavy weightlifters. The study with the lowest cut-off value (≥130/85 mm Hg) also had the highest overall prevalence of hypertension (45.1%, compared with 17% in an age-matched and gender-matched control group).37 The study with the highest cut-off value for hypertension (≥160/90 mm Hg) still reported a prevalence of 9.5%,27 but this study included athletes with the highest age (36.4±4.5 years), and selectively reported the highest of the measured BPs.
Two-thirds of the studies reported mean BP in the prehypertensive range. There are several possible explanations for this. First, in many of these studies, BP was measured only once and one recording is often higher than the mean of two recordings. Second, the cuff size might have been too small for the muscular upper arms of athletes, which means that BP is measured falsely too high since only a minority of studies reported if they had used an appropriate cuff size. Third, the environment was probably not quiet in most studies and the athletes had no rest prior to the BP recordings. Fourth, the BP was recorded postseason. In a recent study of 132 professional American-style football participants, both SBP and DBP increased significantly from before to after the season.14 There is also the possibility that many athletes do have BP in the prehypertensive range, as suggested by several studies in this review and as supported by the trend towards a higher BP in athletes training ≥10 h/week than in those training <10 h/week. Physical activity has a well-known BP-lowering effect in the general population33 and studies of ‘exercise as medicine’ report a decrease in BP of 4–9 mm Hg33; but the amount of physical activity in these studies is often limited to 30 min most days a week. In our review, most athletes were ‘elite’ or ‘professional’, training on average 14.4 h per week or had been training vigorously for an average of 8.8 years, and it may well be that BP reacts differently to such amounts of training than to more moderate amounts of physical activity. There can be many biological reasons for high BP in athletes. First, the mental stress associated with competition at a high level might increase the athletes’ BP, as indicated by the finding of a larger difference in SBP between professional athletes and controls (4.4 mm Hg, p=0.350), than that between non-professional athletes and controls (0.2 mm Hg, p=0.916, data not shown). Second, BP might be increased due to ‘spurious systolic hypertension’ when BP is measured in the upper arm in athletes.52 Third, some athletes might use BP-increasing drugs, as shown in several studies,18 ,53 which is an argument for collecting information about use of medication during preparticipation screening of athletes.33
We also found interesting differences between subgroups of athletes. For example, male athletes had significantly higher BP than female athletes; this was also found in a small study of 15 pairs in sports dancing, which showed that male dancers had significantly higher BP than their female counterparts, despite similar levels of training.54 We also found higher BP and a higher prevalence of hypertension in strength-trained athletes than in endurance-trained athletes, in accordance with the ‘Morganroth hypothesis’.55 The highest prevalence of hypertension, of 83.0%, was found in professional male Chinese strength athletes, predominantly weightlifters, in the unlimited maximum body weight class.33
There is increasing concern about the effects of vigorous, long-term athletic training on cardiovascular health56–58 and it is possible that some of the harmful effects may be mediated through high BP. High BP in adulthood increases risk of cardiovascular disease in the general population2 ,3; we and others have found an association between high BP and left ventricular hypertrophy in athletes.13 ,54 ,59 Whether this is a benign physiological adaptation to high BP or a beginning of pathological remodelling is not known. It may also be that left ventricular hypertrophy provokes hypertension or that other factors confound the association between high BP and left ventricular hypertrophy. High BP may also be a part of the explanation for the fivefold increased risk of atrial fibrillation in endurance athletes15 ,60–62 and exercise-induced arrhythmogenic right ventricular cardiomyopathy56 through repeated bouts of high BP on myocyte junctions in the atria and the ventricles.
Clinical impact and conclusions
BP and prevalence of hypertension in athletes varies considerably partly because of variations in measurement methods, but type and intensity of training seem to play a role. Strength-trained athletes have significantly higher BP than endurance-trained athletes and vigorous physical activity does not seem to reduce BP in athletes compared with controls. Some studies found an association between high BP and left ventricular hypertrophy, but the clinical impact of high BP in athletes is not known. Future studies should adhere more rigorously to the recommendations for measurement of BP and should be designed to determine more precisely the prevalence, determinants and prognostic significance of hypertension in athletes.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
HMB and CBI contributed equally.
-
Contributors All authors contributed to study design, discussion of the data and the final manuscript. CBI performed the systematic searches and extracted the data. HMB controlled the extracted data, performed the analyses and wrote the first draft of the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.