Article Text

Abstract
Background/aim Groin injuries are common in football and ice hockey, and previous groin injury is a strong risk factor for future groin injuries, which calls for primary prevention. The aim of this systematic review was to evaluate the effect of specific groin-injury prevention programmes in sports.
Methods A comprehensive search was performed in May 2014 yielding 1747 potentially relevant references. Two independent assessors evaluated randomised controlled trials for inclusion, extracted data and performed quality assessments using Cochrane's risk of bias tool. Quantitative analyses were performed in Review Manager 5.3.
Results Seven trials were included: six on football players (four male and two female populations) and one on male handball players. In total there were 4191 participants with a total of 157 injuries. The primary analysis, including all participants, did not show a significant reduction in the number of groin injuries after completing a groin injury prevention programme (relative risk (RR) 0.81; 95% CI 0.60 to 1.09). Subgroup analysis based on type of sports, gender and type of prevention programme showed similar non-significant estimates with RR ranging from 0.48 to 0.81.
Conclusion Meta-analysis revealed a potential clinically meaningful groin injury reduction of 19%, even though no statistical significant reduction in sport-related groin injuries could be documented.
Trial registration PROSPERO registration ID CRD42014009614.
Statistics from Altmetric.com
Introduction
Groin injuries represent 5–10% of all sports injuries.1–4 They are highly prevalent in sports requiring kicking, high-speed direction changes and/or skating motions. In these sports groin injuries account for 10–23% of all injuries.5–10 In football and ice hockey, groin injuries have an incidence of 1.1/1000 h exposure9 and 1.3/1000 players exposure,11 respectively, during a regular season. The hip adductors are the most commonly injured muscle group in sports-related groin injuries.9–12 This is likely due to the eccentric forces stressing the muscle–tendinous complex during side-to-side cutting, kicking and powerful skating.13 ,14 Groin injuries seem to be less frequent in female compared with male football players.4 ,15 ,16 In men, more than 50% of groin injuries are classified as moderate or severe at elite level,9 ,17 resulting in substantial periods of absence from football play. Recent studies showed that the prevalence of hip and groin pain during a season can be up to 70%,18 ,19 suggesting that time-loss injury incidences represent the tip of the injury iceberg, with many athletes often continuing to play, but with pain.20
A previous history of groin injury11 ,17 ,21 or hip adduction strength deficits22–24 has been identified as a significant risk factor for a new groin injury. Groin injury prevention consists of active strength and coordination exercises, with emphasis on the adductor and abdominal muscles,22–26 as these are modifiable risk factors.21 ,27 An exercise programme including strengthening and coordination exercises for adductors and muscles around the pelvis has also been demonstrated to be effective in treatment of long-standing groin pain.28 Similarly, a preseason adductor strengthening programme appeared to reduce the incidence of adductor strains in a group of professional ice hockey players.29 Therefore, it seems reasonable to assume that groin injuries in sports may be prevented through specific prevention strategies targeting relevant risk factors and mechanism of injury despite the fact that this seems to remain unproven in randomised controlled trials.
Preventing groin injuries in sports such as football and ice hockey is of great importance, since these injuries induce substantial disability and loss of playing time, injury-related costs30 and an increased risk of reinjury9 ,17 ,21 and chronicity.9 ,28 ,31 However, to the best of our knowledge, no systematic review or meta-analysis on the prevention of groin injuries in sports has been published to date. The aim of this systematic review was to evaluate the effect of specific groin-injury prevention programmes in sports.
Methods
Search strategy
EMBASE, MEDLINE, SPORTDiscus, LILACS, PEDro and Cochrane Central Register of Controlled Trials were electronically searched from January 1970 to May 2014. A hand-search of the reference lists of relevant articles was also conducted for other potential relevant references. A review protocol was developed according to the PRISMA32 recommendations and published in the PROSPERO database (http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42014009614). The search strategy was constructed and followed the PICO approach (Population, Intervention and Outcome). Search terms were mapped to each component of the PICO and connected with Boolean operators adapted to the individual databases. When possible, filters for randomised controlled trials were applied. The complete search strategy can be seen in online supplementary web-appendix 1.
Inclusion and exclusion criteria
Data from randomised and cluster-randomised controlled trials were included. We included studies with athletes that reported the incidence of groin injuries as an outcome. Only full text trials in English were considered. Studies conducted in army recruits were excluded.
Review process
Titles and abstracts identified in the search were downloaded into EndNote X7 (Thomson Reuters, Carlsbad, California, USA); cross references and duplicates were deleted. All publications potentially relevant for inclusion were independently assessed for inclusion by two reviewers (EE and KT) and full texts were obtained, if necessary. Any discrepancies were resolved during a consensus meeting, and a third reviewer was available (CB), if needed.
Data extraction
Two reviewers (EE and KT) independently extracted data using a specifically designed standardised form. General study information, participants and intervention characteristics, compliance, withdrawals and outcome measures were extracted. If data were not available from tables or the result section, the authors were contacted. If the authors did not have access to their data, data on outcome were extracted from figures and graphs. Whenever possible, results from the intention-to-treat population were used.
Assessment and risk of bias
The studies included were assessed for the risk of bias by two independent raters (KT and EE), with any disagreements resolved by consultation with a third party (GU). An assessment of the methodological quality was not performed, as no evidence for such appraisals and judgments exists and therefore can be misleading when interpreting the results.33 The use of quality scales and summary scores is considered problematic, due to considerable variations between items and dimensions in scales covered, with little evidence relating to the internal validity of these assessments.34 The risk of bias assessment was done using the Cochrane Collaboration's tool for assessing risk of bias in randomised trials.33 The trial was evaluated across six domains of bias, including one or more items that were appraised in two parts. First, the relevant trial characteristics related to the item were summarised. Second, each bias domain was judged as high or low risk of bias, according to its possible effect on the results of the trial. When the possible effect was unknown or insufficient detail was reported, the item was judged as unclear. When we assessed risk of bias in cluster-randomised trials, particular biases were included in the ‘other bias’ domain, as assessing risk of bias in cluster-randomised trials is recommended in the Cochrane Handbook for Systematic Review of Interventions, V.5.1 (Part 3: 16.3.2).33
Study analysis
Relative risk (RR) and 95% CIs were estimated as relative effect size using the extracted data. In the analysis of cluster randomised controlled trials, we used the intracluster correlations coefficient (ICC) from the trials to adjust for a potential cluster effect. If the authors did not report the ICC we used the ICC from similar trials.
Data synthesis
Review Manager V.5.3 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration) was used to calculate RR. A forest plot was used to allow easy visual comparisons between studies. The level of statistical heterogeneity for pooled data was established using the χ2 and I2 statistics. The χ2 and I2 statistics describe heterogeneity or homogeneity of the comparisons with p<0.05, indicating a significant heterogeneity.35 A fixed-effect model was used when studies were statistically homogeneous. The Mantel-Haenszel36 ,37 method was selected as default option. This method has been recommended when there are low event rates.33 If studies were statistically heterogeneous, the Mantel-Haenszel36 ,37 random-effects model was applied. Sensitivity analyses were planned on the primary outcome, focusing on methodological quality and risk of bias assessment. We considered aspects such as: allocation concealment, outcome assessor blinding, incomplete data, selective reporting and other bias.
Analysis of subgroups or subsets
Possible interactions between groups were evaluated using the technique outlined by Altman and Bland.38 Relations sustained on type of sports, gender and type of preventive programmes were assessed.
Results
Search results
The initial search identified 1747 unique references (figure 1). After exclusion by title and abstract, 33 were read in full text. From the 33 articles, 26 were excluded. The most common reason for exclusion (15 studies) was that studies did not report the incidence of groin injuries in isolation. Eleven studies were not RCTs and were therefore also excluded. Finally, seven studies were included.

Flow chart of included studies.
Description of studies
The most relevant characteristics of the seven included studies are summarised in table 1. For detailed information on study design, participants, exposure and statistics see online supplementary web-appendix 2. Six studies were cluster-randomised controlled trials, where teams or clubs were the unit of randomisation, while one study performed randomisation at the individual level. In total, the included studies involved 4648 participants. Three studies reported exposure data.39–41 Among cluster-randomised trials, one study was adjusted for clustering effects, reporting an ICC value equal to zero.42 Compliance reports were not specified according to prescribed or optimal dosage (see table 1) and only three studies reported intention-to-treat data.
Characteristics of the included studies
Time-loss groin injury definition was used in six of the seven included studies,39–41 ,43–45 while the last study used time-loss as well as medical-attention definitions.42 The authors of two studies were contacted to provide extra data for exposure, age of participants and number of groin injuries.42 ,43 Data from van Beijsterveldt et al43 were obtained, but exposure data from Hölmich et al42 were not available. Results of the risk of bias assessment are presented in meta-analysis figures (figure 2A–F). Specific justification for each assessment is included in online supplementary web-appendix 2.

{kind=link}
{kind=link}
{kind=link}
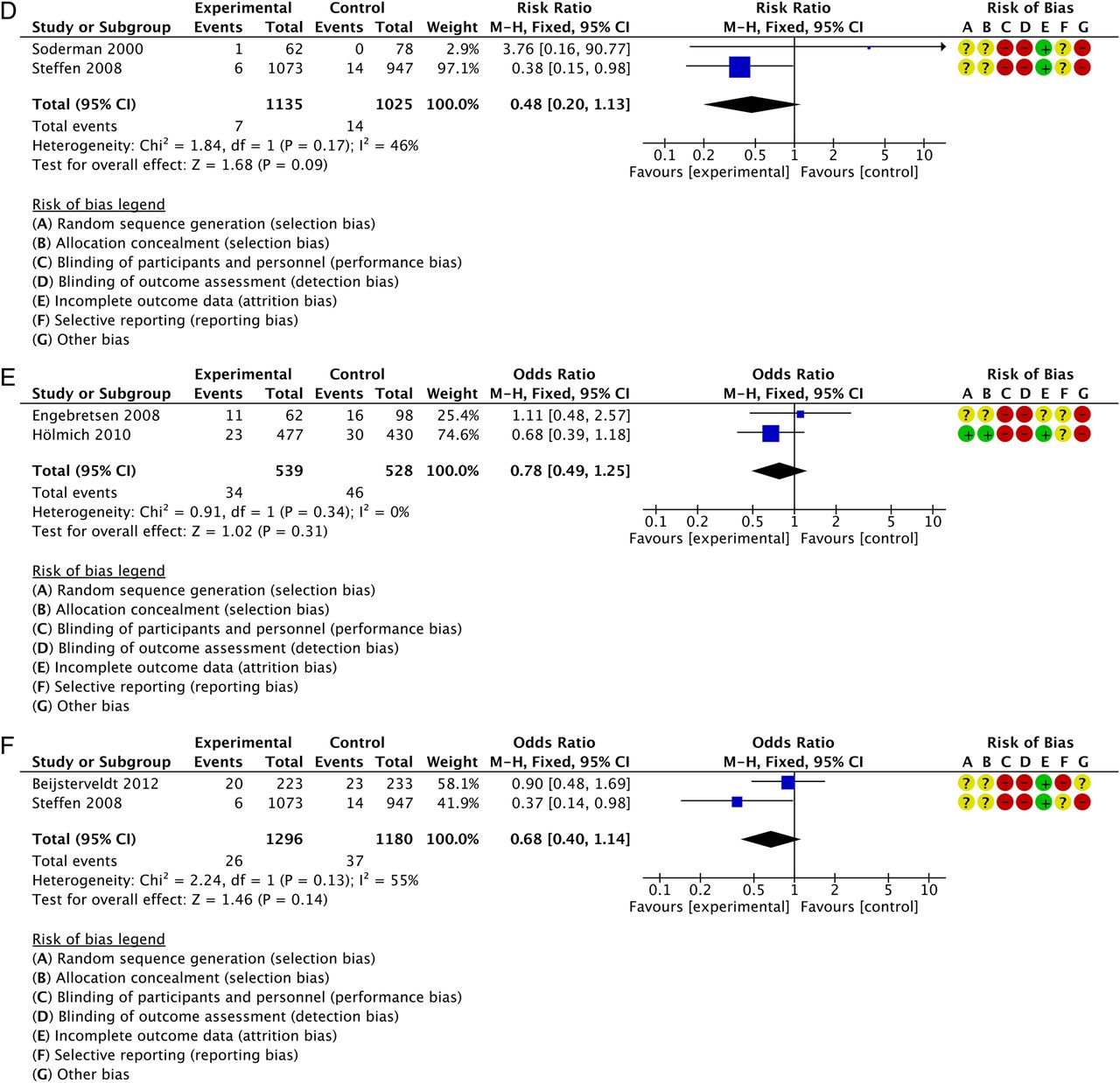
(A) Primary analysis including all seven studies. (B) Subgroup analysis based on type of sport. (C) Subgroup analysis based on gender (only women). (D) Subgroup analysis based on gender (only men). (E) Subgroup analysis based on type of preventative programme (active adductor strength programme). (F) Subgroup analysis based on type of preventative programme (‘The 11’).
Total estimate
In total, 4191 players were included in the primary analysis. For the primary outcome, number of groin injuries in the control group versus the intervention group, the effect estimates based on 157 injuries (figure 2A), was RR 0.81 (95% CI 0.60 to 1.09; I2=7% χ2 p=0.37).
Type of sport analysis
The study on handball players did not report any groin injuries.45 The subgroup analysis on type of sport (figure 2B), therefore, included the remaining six football studies,39–44 which showed an effect estimate of RR 0.81 (95% CI 0.60 to 1.09; I2 =7% χ2 p=0.37).
Gender analyses
A gender specific subgroup analysis of two football studies conducted among female players, including active exercise programmes (figure 2C),41 ,44 showed an estimate of RR 0.48 (95% CI 0.20 to 1.13; I2 =46% χ2 p=0.17). Pooled data from the three football studies, including active exercise programmes, performed among men (figure 2D),40 ,42 ,43 showed an effect estimate of RR 0.84 (95% CI 0.60 to 1.18; I2 =0% χ2 p=0.57).
Type of preventive programme analyses
An active adductor strength programme was tested in two studies,40 ,42 with a pooled effect estimate (figure 2E) of RR 0.78 (95% CI 0.49 to 1.25; I2 =0% χ2 p=0.34). ‘The 11’ preventive programme (figure 2F) was tested in two trials,41 ,43 with a pooled effect estimate of RR 0.68 (95% CI 0.40 to 1.14; I2 =55% χ2 p=0.13).
Discussion
The aim of this systematic review was to evaluate the effect of specific groin-injury prevention programmes in sports. No statistical significant reduction in sport-related groin injuries could be documented. Meta-analysis revealed a potential clinically meaningful groin injury reduction of 19% (RR 0.81; 95% CI 0.60 to 1.09).
Subgroup analyses
Football
An identical non-significant estimate was identified in the subgroup analysis in football players (RR 0.81; 95% CI 0.60 to 1.09). Five of the six studies conducted on football players assessed the efficacy of active exercise strategies to prevent groin injuries.40–44 The potential effect of such type of intervention was previously documented in a prospective study of ice hockey players at high risk,29 but has never been tested in a randomised controlled trial. Nevertheless, in a randomised trial an active strengthening programme was very effective in the treatment of long-standing adductor-related groin pain in athletes.28 Moreover, the effect of this therapeutic intervention was found to be long-lasting,46 suggesting a possible secondary preventive effect.
Among the six studies conducted on football players, two studies40 ,41 reported limited compliance. A deterioration of compliance during the season has been shown previously in football studies, which may affect the results, as higher compliance allows for better results in preventive interventions.47 ,48 Compliance was very low in one study40 of a home-prevention programme, where less than 20% of the participants completed 20 or more of the 30 planned sessions. It is important to consider that an active programme under supervision usually gives higher compliance and more benefits in strength and physical conditioning.49
Sex
The sex-specific subgroup analysis, including studies looking at active exercise programmes, showed a non-significant risk reduction of 52% among female football players (RR 0.48; 95% CI 0.20 to 1.13). In comparison, the analysis including male football players showed a non-significant risk reduction of 16% (RR 0.84; 95% CI 0.60 to 1.18). Although non-statistical, the apparent difference in estimates is interesting. We speculate that if this difference exists it could be because these programmes are different in nature. Furthermore, groin injuries in women seem to be more related to hip joint and hip flexors,12 and significant differences in kinematics and muscle activation have been identified between genders during single-leg actions or cutting manoeuvres.50–53 It may be that women could obtain a better effect from preventive interventions focused on lower extremity alignment and neuromuscular control, as suggested by a possible large reduction in groin injuries among women, when initiating balance and coordination type exercises. Among male football players, groin injuries are often related to the hip adductor muscle group,10 ,12 and hip adduction weakness seems to be a significant risk factor in this group of athletes.23 ,24 Considering apparent hip strength54 and coordination differences50–53 between men and women, it seems relevant to consider in the future whether groin prevention approaches must be specifically adapted to sex in the future.
Type of preventive programme
A non-significant risk reduction of 32% (RR 0.68; 95% CI 0.40 to 1.14) in the number of groin injuries was identified in the subgroup analysis on type of preventive programme. The potential preventive effect of ‘The 11’ programme in reducing the risk of groin injuries in female football players was recently highlighted in a systematic review.55 However, a revised programme, ‘The 11+’, including additional but very similar exercises to allow for variations and progressions, showed no effect on prevention of hip and groin injuries in young female football players.56 Further, in the same study, only 19 hip and groin injuries were included, in approximately 1900 players during a football season, suggesting that this problem is either minor or severely underreported, providing insufficient power to produce robust estimates on hip and groin injury preventative effects in this study.56
Pooled data for the effectiveness of adductor strength programmes in male football revealed a non-significant risk reduction of 22% (RR 0.78; 95% CI 0.49 to 1.25). Exercises in these interventions included concentric and eccentric adductor muscle contractions in coordination with abdominal muscles to target hip adductor weakness.23 We feel that the use of no or minimal equipment, such as elastic bands, progressing into more relevant contraction-specific exercise and positions,57 ,58 could be more beneficial for hip-adductor strengthening as a preventative measure in male football.24 ,57
Risk of bias assessment
In the risk of bias assessment, we considered the seven studies included at high risk of bias concerning blinding of participants and outcome assessors. In these types of preventive studies consisting of active interventions and subjective outcomes, true blinding is considered impossible. Further, the injuries were reported subjectively and participants were aware of the outcome. Thus, the outcome assessors were dependent on the subjective report, which theoretically could be influenced by study participants. Lastly, in five of the six included cluster randomised trials, insufficient information was reported and studies were considered as unclear on selection bias. Despite the fact that all seven studies included had several methodological aspects displaying high risk of bias, no obvious methodological differences in terms of blinding, concealment allocation, outcome definition or study designs, were present between studies. Therefore, we considered the seven studies included to be sufficiently homogeneous to allow for a meaningful meta-analysis, providing the best available evidence.
Studies in the present review mainly included interventions based on active exercise strategies with the aim of improving hip/core strength, and/or lower limb balance and coordination exercises.40–45 The only study with a different approach was the study by Arnason et al,39 including a video-based awareness session in the respective clubs as a one-time intervention. Future studies may need to consider prevention strategies other than those aiming to improve hip/core strength and lower limb coordination. Regular physical screening and load monitoring in place of a sole preseason strategy have been suggested as a worthwhile strategy for early groin symptom identification and prevention.59–61 Future randomised controlled trial studies concerning early groin symptom identification and load management strategies are needed to investigate the effect of this kind of groin injury prevention strategy.
Limitations
More than 4000 players were included in the meta-analysis. However, the total number of injuries was very low (157 groin injuries in total). The outcome (groin injuries) in these studies was rare and large studies with at least 4000 players in each group are required to detect a 20% reduction in the number of groin injuries assuming that 8% of the players develop a groin injury.42 Unfortunately, all analyses in the present study are not sufficiently powered to statistically support the estimates provided, although they all suggest a reduced effect of different groin injury prevention strategies across different groups of athletes.
Owing to the lack of compliance reporting and specific definitions on compliant and non-compliant behaviour in the included studies, we believe that the estimates of the present study may, in fact, resemble the interventions’ ‘true’ effectiveness (effect when applying intervention in real life), and not necessarily their efficacy (effect when applying intervention under controlled research conditions).62 Three of the included studies39 ,42 ,45 did not report information about compliance, and in the remaining four,40 ,41 ,43 ,44 the participants did not perform the prescribed number of sessions. Above all, studies were not adjusted for compliance, meaning that the estimates are suggested to represent the intentions’ effectiveness, and the efficacy of these interventions, at present, remains unknown.
An important limitation is that groin injury was not specifically defined in any of the included studies, and none of them reported the use of a standardised diagnostic protocol. Groin injury diagnosis is extremely challenging due to the possible multiple pathologies and overlapping symptoms.12 ,63 It is known that the lack of consensus regarding injury definitions, diagnostic and standardised data collection procedures could influence the reported incidence of sports injuries.64 Importantly, in six of the seven included studies, a time-loss definition was used.39–41 ,43–45 When this definition is used one must take into account that minor injuries and/or especially overuse problems will not always be recorded. This will cause an underestimation of the total number of injuries. To avoid this problem, the use of questionnaires aimed at pain, function and sporting activity has been suggested for more detailed groin injury registration.65 The Copenhagen Hip and Groin Outcome Score (HAGOS)66 ,67 has previously been validated in athletes with and without hip and/or groin pain and should be considered in future evaluations of preventive interventions for sports-related groin injuries.
Conclusion
Meta-analysis revealed a potential clinically meaningful groin injury reduction of 19%, even though no statistical significant reduction in sport-related groin injuries could be documented. Insufficient statistical power from the included studies makes it difficult to provide firm conclusions on the effect of groin injury prevention.
What are the new findings?
-
No statistical significant reduction in sport-related groin injuries could be documented.
-
Estimates of groin injury reduction of 19–52% after implementing active groin injury prevention programmes, including specific exercise programmes, suggest that such an approach may be of clinical relevance and potentially worthwhile to consider in football players.
-
Estimates concerning the efficacy of groin injury programmes in football are unknown as compliance and compliance reporting have been inadequately addressed in existing trials.
Acknowledgments
The authors would like to thank Mr Jordi Vicens Bordas for his assistance in completing this systematic review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Twitter Follow Ernest Esteve at @EsteveErnest
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.