Article Text

Abstract
Background Return to sport and to pre-injury level represents an important outcome after both primary and revision anterior cruciate ligament (ACL) reconstructions.
Purpose The aim of the present meta-analysis was to determine the return to sport rate after revision ACL reconstruction.
Material and methods A systematic search was performed of the MEDLINE, Embase and the Cochrane Central Register of Controlled Trials Databases. All the studies that reported return to sport, return to pre-injury sport level and return to high level/competitive sport was considered for the meta-analysis. The overall pooled mean of post-operative knee laxity and pooled rate of positive pivot-shift and objective International Knee Documentation Committee (IKDC) categories was calculated as well.
Results Overall, 472 abstracts were identified and screened for inclusion and only 16 studies reported the rate of return to any level of sport activity at the final follow-up of 4.7 years (range 1.0–13.2 years), showing a pooled rate of 85.3% (CI 79.7 to 90.2). The return to pre-injury sport level was achieved in 53.4% (CI 37.8 to 68.7) of cases. Normal or quasi-normal objective IKDC, less than 5 mm of side-to-side difference at arthrometric evaluations and grade I-II pivot-shift test were reported in 84%, 88% and 93% patients, respectively.
Conclusions In spite of almost 8 patients out of 10 returning to sport after revision ACL reconstruction and showing good stability, only half of the patients returned to the same pre-injury sport level.
- ACL
- Knee
- Sport
- Review
Statistics from Altmetric.com
Introduction
Return to sport and especially to pre-injury levels represents for patients one of the most important clinical outcomes after ACL reconstruction. Despite clinical satisfaction and adequate knee range of motion (ROM), stability and muscle strength, the ability to perform sports activity is believed to represent a good indicator of overall knee health and of the ability of the joint to sustain external load and stress, particularly in high-level, competitive and pivoting activities.1 However, in certain circumstances, the normalised objective knee status and recovered muscle strength do not correspond to the ability to perform sport, especially when psychological recovery is not reached.2–5
With regard to this, the outcomes of return to sport after primary ACL reconstruction have been extensively investigated through high-level clinical studies and well-conducted meta-analyses.1 ,6 ,7 In contrast, the outcomes of revision ACL reconstruction derive mostly from level IV retrospective studies.8 A recent meta-analysis of 21 studies investigated the main clinical outcomes of revision ACL reconstruction, reporting a return to unrestricted activities or to the previous levels of activity in 54%, but without clearly defining a precise return to sport activity definition.8 Moreover, since then, clinical studies reporting the results after revision ACL have almost doubled, underlining the increasing interest in this surgical procedure. If the increased number of ACL lesions, estimated at around 36.9/100 000 person-year,9 and the failure rate of primary ACL reconstruction of 7–10%10 are considered, it is not difficult to understand the burden of the revision ACL reconstruction procedure and its importance in the field of sports medicine and traumatology.
Nowadays ACL revision surgery, once considered but a salvage procedure, is increasingly obtaining results which are more and more similar to primary reconstruction mainly regarding clinical outcomes and knee stability,8 ,11 owing to technical surgical advances. However, the ability to perform sports activity after revision ACL reconstruction remains a not adequately investigated issue, as single studies reported the return to pre-injury sport level ranging from 0% to 100%.12 ,13
The primary aim of the present meta-analysis was to synthesise the current evidence related to sports activity after revision ACL reconstruction, and to determine the overall average postoperative return-to-sports and return to pre-injury sport level rates. The secondary aim was to summarise key objective knee function measures, including the International Knee Documentation Committee (IKDC) score, the anteroposterior knee laxity and pivot shift test.
Material and methods
Study design
A meta-analysis was performed in accordance with the PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses.14 No protocol exists for this study, which was exempt from review by Ethical Committee approval for only those studies that involved human participants, as no patients were enrolled in the study and nor were medical or surgical treatments directly administered. No external funding supported the present study.
Search strategy
An electronic search was performed on 31 September 2014 of the MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials databases. The search terms used were “Anterior cruciate ligament” and “ACL” combined with the terms “revision”, “reoperation” and “failure”. Filters were utilised to access only those studies that investigated participants and were reported in English. No limitations were imposed on the date of publication. The reference section of each full-text obtained was scanned and hand-searched for other possible inclusions to this study, which were not identified in the electronic database search.
Eligibility criteria
Studies were included if they met the following criteria: (1) randomised controlled trial (RCT), prospective or retrospective study, (2) the study reported the outcomes of both first or multiple revision ACL reconstruction, (3) the study reported at least one of: the return to any kind of sport rate, return to pre-injury sport level. When “return to pre-injury activity” was used as the outcome without mentioning the nature of the activity, the definition was considered too vague and therefore the study was excluded. The authors of the studies that met some but not all of the criteria were contacted for further information and to clarify whether the study was eligible or not.
Study selection
Two authors (AG and GMMM) independently reviewed the studies found during the database search. Articles were screened for eligibility based on a review of the title and abstract only. Any potential disagreement was resolved via consensus discussion between two independent reviewers, with a third reviewer (SZ) being consulted if the disagreement could not be resolved. When the eligibility was unclear from the title and abstract, the full text was obtained and assessed and again evaluated for eligibility.
Data collection and analysis
All the data regarding the names of authors, year of publication, number of patients treated, final follow-up duration and graft used for revision procedure were obtained and tabulated in an Excel extraction form to systematically extract the data. Regarding the sport-specific outcomes, details of all the patients who were still practising any kind of sport at final follow-up, and of all the patients who at final follow-up returned to the same level practised before the first ACL injury, were accurately extracted from each study and evaluated as primary outcomes. When possible, the subgroups of patients who returned to high level and competitive sport activity—according to clinical scores and definitions provided in each study—were also extracted.
The secondary outcomes relative to the final follow-up were the objective IKDC15 ,16 classification, knee laxity measured as side-to-side difference at the manual maximum displacement test measured in mm with KT-1000 or KT-2000 and results of the pivot-shift test. The percentage of participants with knee classified as category A (normal knee), B (nearly normal knee), C (abnormal knee) or D (severely abnormal knee) according to the IKDC form was calculated. Arithmetic averages of knee laxity and percentages of patients with a <3, 3–5 or >5 mm side to side difference at the manual maximum displacement test were calculated as well. The total number of patients with a pivot-shift test graded as normal (equal to the contralateral side), grade I (or glide, in case defined as a small and gentle sliding reduction), grade II (or clunk, in case of reduction movement easily appreciated) and grade III (gross, in case of an abnormal movement with a pronounced clunk)17 ,18 was calculated and expressed as a percentage for each groups. As for multiple revisions, the data regarding first revision were collected when available; otherwise, only data of the last revision were used for analysis.
Quality assessment
The studies included were assessed using a six-item checklist developed by Ardern et al1 for the evaluation of return to sport outcomes after primary ACL reconstruction. The six items assessed were: selection criteria described, representative population selected, participants’ pre-injury sports participation level reported, data collected prospectively, demographic data reported and postoperative sports participation level compared with pre-injury level. Items were scored as follows: one point for satisfaction of the criterion, no points for not satisfying the criterion. A score of zero was given if it was unclear whether the criterion had been satisfied or not. All articles were assessed independently by two assessors, disagreements being resolved by consensus, and third reviewer intervention in case of disagreement not being resolved. κ Coefficient for inter-rater agreement was calculated as well. The purpose of the quality assessment in this meta-analysis was to identify characteristics of study quality and design common to all included studies, and to provide a qualitative description of these characteristics in the meta-analysis.
Statistical analysis
Statistical evaluation was performed using MedCalc (MedCalc software, Acacialaan 22, Ostend, Belgium). Data regarding return to sport, return to pre-injury sport level and return to high-level/competitive sports were combined via a proportion meta-analysis using a random effects model. I2 index was used to measure the amount of inconsistency in the results of the included studies.19 ,20 A larger I2 index indicates that a greater amount of the variability in the results is due to the heterogeneity rather than to chance.19 ,20 The mean and 95%CI was calculated for return to sport, return to pre-injury sport level and return to high level/competitive sport rates. Studies included in the meta-analyses were weighted according to sample size. Return to sport rate data from the individual studies were presented through forest-plot graphics.
The objective IKDC, KT-1000 or KT-2000 values and pivot-shift results were presented as the number of patients and percentage of patients for each category. The anteroposterior knee laxity measured with KT-1000 or KT-2000 was presented also as mean value expressed in mm.
Results
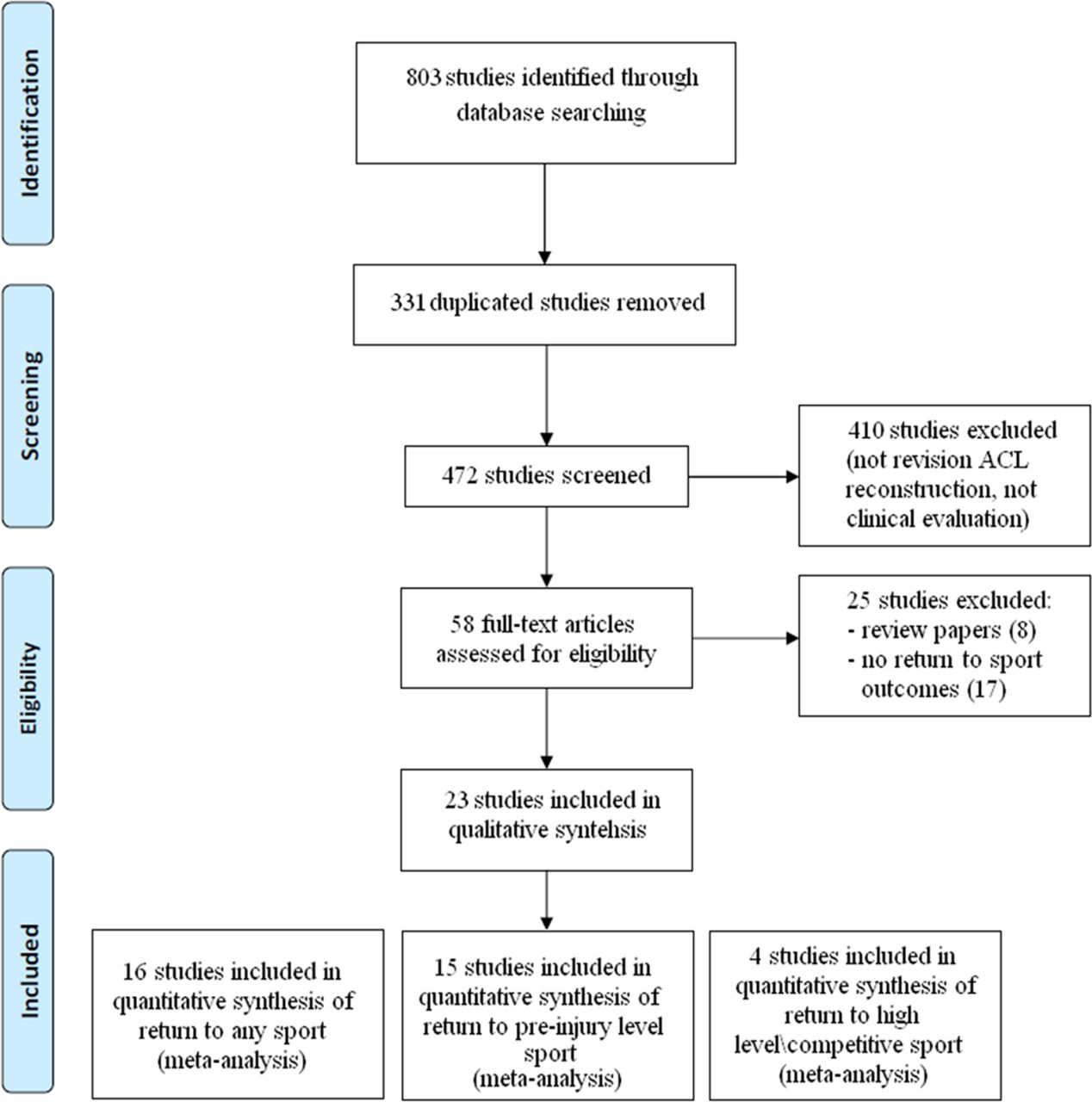
The literature search yielded a total of 803 results. A flow diagram of the selection process is shown in figure 1. After duplicates were removed, 472 studies remained. Of these, 414 were excluded after reviewing title and abstract review, as involving mostly surgical technique descriptions, in-vitro, biomechanics or radiologic studies, or because were studies not related to revision ACL reconstruction. The full text of the remaining 58 studies were obtained and reviewed for eligibility. Thirty-five studies were excluded because they did not report the outcomes requested in the inclusion criteria (24 studies) or because they were narrative or systematic reviews (11 papers). Therefore, 23 studies were included in the final analysis.10–13 ,21–39 A summary of the population examined with clinical outcomes is presented in table 1.
Details of patient populations, follow-up duration, time from primary to revision ACL reconstruction, objective outcomes at final follow-up (objective IKDC, difference of laxity between indexed and healthy knee and pivot-shift test) and return to sport outcomes for each study

PRISMA flow diagram of the selection process.
Demographic data
The 23 reviewed studies presented the results of 1090 patients at a mean follow-up of 5.3 years (range 1.0–13.2 years). When gender was reported,10 ,11 ,13 ,24 ,26 ,28 ,29 ,33 ,37 ,38 revision ACL reconstruction was performed in 318 males (63%) and 187 females (27%). The mean age at revision surgery was 27.7 years (range 13–60 years), while the mean time from primary reconstruction and revision surgery, reported in 13 studies,10–12 ,22–24 ,27 ,28 ,30 ,31 ,33 ,34 ,37 was 43.8 months (range 1–276 months). Most of the studies reported the results of a first revision procedure, while only four studies12 ,29 ,34 ,38 reported at least one second-revision/third-revision procedure. Concerning the primary ACL lesions, 8% sustained ACL repair and 3% underwent an extra-articular procedure; when ACL reconstruction was instead performed, the primary graft to be used was bone patellar-tendon bone (BPTB) autograft in 57%, hamstrings autograft in 16%, other autografts in 2%, synthetic grafts in 7%, BPTB allograft in 2% and other allografts in 7%.
Regarding the revision procedure, eight studies reported the results of one single specific graft, another eight used a combination of different autografts (6 studies) or allografts (2 studies), while the remaining seven reported the use of a heterogenous combination of allografts and autografts. Specifically, a BPTB autograft was used in 554 patients (50%), a hamstrings autograft in 326 (29%), a quadriceps tendon autograft in 71 (6%), a BPTB allograft in 98 (9%), an Achilles tendon allograft in 28 (3%) and other allografts in 38 (3%).
Quality assessment
Sixteen studies (69%) were prospective case series, 4 (17%) were retrospective case series while the remaining 3 (14%) were comparative studies between primary and revision reconstruction or between different populations.
Regarding quality assessment, only 5 studies (22%) fulfilled all the 6 items, while 9 (39%) fulfilled 5 items. Three studies (13%) fulfilled 4 items and 6 (26%) fulfilled 3 items (table 2).
Details of study design, quality assessment, mixed or athletic population included in each study and the definition of return to sport extracted from the text of each study, with the scale to measure activity level (when used)
The item “selection criteria described” was fulfilled by all 23 studies (100%), such as the “demographic data reported item”. The “representative population selected” item was fulfilled by six studies (26%) and the “data collected prospectively” item was fulfilled by 19 studies (83%). Finally, the item “participants’ pre-injury sports participation level reported” was fulfilled by 19 studies (83%), while the “postoperative sports participation level compared with pre-injury level” was fulfilled by 15 studies (65%).
The inter-rater agreement between the two reviewers regarding quality assessment was k=0.92 (95% CI 0.88 to 0.94).
The definitions of the parameter used to assess the return to sport and pre-injury sport level were not consistent between all the studies and are described in table 2.
Only six studies reported the outcomes of athletic populations, with inconsistent description of the practised sports; the other studies involved mixed populations of both athletic and non-athletic patients, or did not provide information regarding the populations studied.
Return to sport outcomes
Overall, 16 studies12 ,21–25 ,27–29 ,31 ,32 ,34–38 involving 543 patients reported a rate of return to sport activity at any level at the final follow-up; the pooled rate was 84% (CI 78 to 89) (figure 2), I2=65% (p=0.0001).

Forest-plot graphic of return to sport outcome; %, mean percentage; CI, 95% CIs.
Fifteen studies,10 ,11 ,13 ,24 ,26–28 ,32–39 involving 790 patients, reported a rate of return to the same pre-injury sport level; the pooled rate was 52% (CI 36 to 67) (figure 3), I2=95% (p=0.0001).

Forest-plot graphic of return to pre-injury sport level; %, mean percentage; CI, 95% CIs.
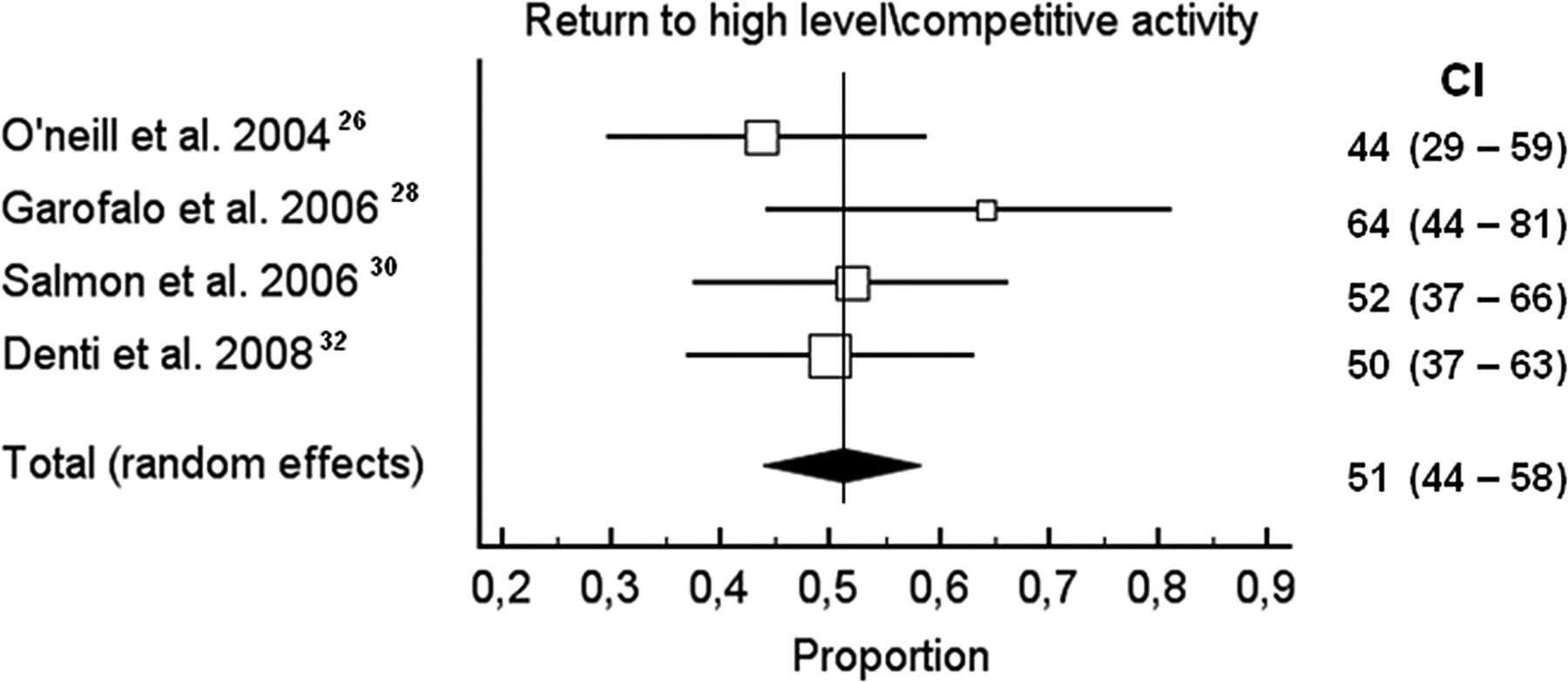
Four studies,26 ,28 ,30 ,32 involving 186 patients, reported a rate of return to high-level/competitive sport; the pooled rate was 51% (CI 44 to 58) (figure 4), I2=0% (p=0.3921).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest-plot graphic of return to high–level/competitive sport; %, mean percentage; CI, 95% CIs.
Only one study,12 involving 11 multiple revisions performed with reharvested ipsilateral or contralalateral BPTB, reported the time to return to sport. Return to light sport was achieved after 5.1±2.2 weeks after revision, while return to full sport was achieved after 5.4±1.5 months.
Only three studies,21 ,28 ,31 involving 174 patients, reported the main reason for not returning to sport after ACL revision surgery: 31 patients (69%) were not able to return to sport because of knee-related problems, 10 (22%) because of the fear of re-injury while 4 (9%) were unable to do so for other reasons.
Secondary outcomes
Twelve studies10 ,13 ,26–30 ,32–34 ,37 ,38 reported the IKDC results in 392 patients. At final follow-up, 177 patients (45%) had knee function rated as normal (A), 160 (41%) as nearly normal (B), 48 (12%) as abnormal (C) and 7 (2%) as severely abnormal (D).
Twenty-two studies10–13 ,21–35 ,37–39 reported laxity evaluation at the final follow-up of 1069 patients, reporting a mean final value of 2.6 mm (range −4–6 mm). When reported, 325 patients (58%) presented a value of side-to-side difference at manual maximum displacement test<3 mm, 169 (30%) between 3 and 5 mm, and 69 (12%) >5 mm.
Sixteen studies10 ,11 ,13 ,21 ,22 ,24 ,26–30 ,33 ,35–38 reported the results of the postoperative Pivot-Shift test in 515 patients. The test was considered negative in 338 patients (67%), while it was graded as grade I in 140 (26%), grade II in 29 (5%) and grade III in 8 (2%).
Therefore, 337/392 (86%) patients presented a normal or nearly normal knee (group A and B according to objective IKDC), 494/563 (88%) had normal values of static anteroposterior laxity (side to side difference <5 mm at KT-1000/2000) and 478/515 (93%) had a normal or nearly normal rotatory laxity (normal or grade I pivot-shift test).
Discussion
The main findings of this meta-analysis are that 84% of patients returned to sport after revision ACL reconstruction, while 52% returned to the same pre-injury sport level and 51% returned to high-level/competitive sports.
The return to sport after both primary and revision ACL reconstruction represents a complex outcome to evaluate. First of all, a great inconsistency in reporting the results was found in most of the studies, as a clear and unequivocal definition of return to sport was not provided. For example, the concept of “return to pre-injury sport level” presented a not unequivocal interpretation in most of the studies, especially regarding the kind of sport and its level (amateur, competitive, elite), possibly contributing to the production of high variability of the results reported in this meta-analysis. In fact, the latter outcome was mostly assessed with the sentence “patients returned to the same pre-injury sport activity” or “were able to perform sport equal to pre-injury level”, without mentioning the type of sport, level and intensity. Moreover, only a few studies reported the specific sport performed by each of the patients, thus possibly creating a bias because it could be speculated that patients who perform less demanding activities like tennis or running could hypothetically return to sport easier than patients performing pivoting sports like soccer, basketball and handball.
With the available data obtained from this meta-analysis, the return to any sport outcome was similar to what was reported after primary ACL reconstruction;1 while the return to pre-injury sport level resulted lower compared to primary ACL reconstruction. This could also be due to the higher age at revision ACL reconstruction. In fact, the revision ACL reconstruction could be performed in patients near to 40 years of age. Therefore it could be difficult for them to return to perform the same activity of long time before, when they had the primary ACL injury, and this is not always necessarily due to reasons related to knee performance. Moreover it should be noted that the activity before a primary ACL lesion was used as a landmark in most of the studies. Conversely, the unreported activity level prior to primary ACL reconstruction failure would have probably pointed out the real impact of revision procedure on sport activity, or at least provided adjunctive information regarding the changes of sport practice along the whole follow-up from the very first injury to final evaluation.
Regarding the impact of graft type in the return to sport outcomes, the analysis of the data from the current literature produced inconsistent results. This is mostly due to the lack of well-designed RCTs and to the high heterogeneity in graft choice, between and within each single study. This situation reflects the complexity of revision surgery, such as graft availability derived from previous reconstructions, the status of the contralateral knee, the availability of allograft tissue or the need for a graft with bone stock, which often make the graft choice a necessity rather than a preference. Most of authors used the unharvested BPTB or hamstrings as first choice, while reserving quadriceps tendon autograft, contralateral grafts or various allografts only in case of repeated revision, combined posterior cruciate ligament or posterolateral corner reconstruction, previous multiligament reconstruction or other particular extraordinary circumstances. Therefore only a few studies included revision ACL reconstruction with a single specific graft, making it impossible to compare sport-specific outcomes based on graft choice.
A wide discrepancy is noted between successful results of revision ACL reconstruction based on objective evaluation and sport-related outcomes; normal or nearly normal results were reported in 86%, 88% and 93% for objective IKDC, anteroposterior knee laxity and Pivot-Shift test, respectively, against a rate of 52% of return to pre-injury sport level. The measurement of sport participation represents a relevant issue, especially in athletes and high-level patients, probably superior to objective tools such as knee stability, ROM and muscle strength, because sport participation is more meaningful for them in their daily lives. The reasons for the discrepancy between objective and sport-related outcomes should be evaluated and addressed, as probably in not all cases the inability to return to the same pre-injury sport level was due to the indexed knee problems. In contrast, fear of re-injury, priorities and personality could influence the decision to return to sport.3 ,40 It has in fact been previously demonstrated that issues unrelated to surgical outcomes, such as lack of motivations, reduced confidence, fear of sport incompetence or lower priority on sport due to family/work-related reasons, have negative effects on the return to pre-injury sport level.3 Such evidence, besides representing another potential contributing factor to the high variability of results, could point out the necessity of psychological interventions integrated in the postoperative rehabilitation process to possibly try to improve the outcomes of revision ACL reconstruction, as already suggested for primary ACL reconstruction.41 Moreover, poor surgery, inadequate rehabilitation and impairment of muscle performance, isokinetic strength and functional tests could also affect the ability to return to sport.4 ,5
This meta-analysis presents some strong limitations. First of all, it ought to be mentioned that the return to sport rate considered in this study actually represents the number of patients who are still able to perform sports at the final follow-up. It is plausible that, during the considered follow-up, some patients were able to return to sport after revision ACL reconstruction and rehabilitation, but that several reasons caused them to eventually abandon the practice shortly afterwards. The actual return to sports rate would thus include all patients/athletes being able to resume sports at any time after ACL revision surgery, irrespective of whether they were still active or not at the time of follow-up. However, the ‘return to sports rate’ and the ‘still active at follow-up rate’ were not reported separately in the included studies, thus making an adequate analysis impossible as well as potentially generating misinterpretation of the results. Therefore, the reader should be aware of this major issue and take a conservative approach when drawing conclusions from this meta-analysis.
Another major limitation was the high heterogeneity of the studies included, particularly regarding patients’ characteristics and surgical treatment, which did not allow an analysis of subgroups regarding sport participation and objective outcomes. This is true also for first or second or third revision ACL reconstruction, as only two studies exclusively evaluated this population, making further analysis impossible. Furthermore, the dishomogeneous and equivocal definition of return to sport and return to pre-injury sport level could have created a bias when interpreting the results. Also, owing to the lack of studies with a follow-up of less than 2 years, it was impossible to compare the short-term results of revision ACL reconstruction with the medium-term and long-term results, as already performed by Ardern et al1 when evaluating primary ACL reconstruction. This made it impossible to monitor the sport practice from short-term to long-term follow-up, and to detect potential decreases of sport activity with the passage of time. Finally, the evaluation of subjectively measured parameters, such as Pivot-shift test and IKDC score, could have produced a concrete bias regardless of whether independent examiners were involved in the patient's evaluation, because these objective measures could lack sensitivity to detect subtle differences in function after revision ACL reconstruction. Unfortunately, this issue could not have been investigated adequately due to the great inconsistency in reporting the details regarding the examiner(s) in each study. On the other hand, the evaluation of an objective parameter such as knee laxity determined with KT-1000/2000, despite the lack of inter-rater reliability across different studies, could provide a concrete measure of postoperative outcomes.
Future high-quality RCTs or prospective case series with homogeneous populations, especially regarding graft choice and surgical techniques, could improve the knowledge and understanding of revision ACL reconstruction outcomes. Moreover, the use of a clear definition of sport-related outcomes, such as return to pre-injury sport level, return to training or competitive sport, explicit presentation of the type of sport and level practised before ACL injury, at the end of rehabilitation, and at the final follow-up, could avoid a misleading interpretation of revision ACL reconstruction outcomes and better understanding of the effective ability to perform sport activity after this kind of surgical procedure.
Conclusions
On the basis of the data of the present meta-analysis, 84% of patients returned to sport after revision ACL reconstruction, while 52% returned to the same pre-injury sport level. Normal, or nearly normal, objective results were reported in 86%, 88% and 93% for objective IKDC, anteroposterior knee laxity and Pivot-Shift test, respectively. The high heterogeneity of patient populations and sport-related outcome definitions represent the major biases when evaluating return to sport outcomes after ACL reconstruction outcomes.
What is known about the topic?
Revision ACL reconstruction is an increasingly performed procedure due to the high number of primary ACL reconstructions and failures.
Revision ACL reconstruction is able to restore knee stability and improve knee function.
Return to sport after revision ACL reconstruction has not been deeply investigated.
Wide ranges of return to sport are present in the current literature.
What are the new findings?
84% of patients who had revision ACL reconstruction returned to any kind of sport activity.
52% of patients returned to their pre-injury sport level.
There was a higher percentage of patients with normal or nearly normal knees at final follow-up, compared to the proportion who returned to sport.
A homogeneous definition of return to sport when dealing with revision ACL reconstruction needs to be clarified in future studies.
References
Footnotes
Contributors AG, GMMM and SZ performed a database search and review of articles. MPN and SDV performed data collection and an analysis of the results. MM wrote the paper and critically evaluated the results.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.