Article Text

Abstract
Although there is no consensus as to whether exercise is beneficial during pregnancy, most studies report it poses no risk to either the mother or the fetus, and many suggest it to be beneficial to both. This review, which examines the evidence available, also reveals the many differences in study design followed, the type of exercise undertaken and the variables measured, which make it difficult to compare results. Advances in our understanding of the effects of exercise during pregnancy might best be made by undertaking randomised clinical trials with standardised protocols. However, most of the studies examining the relationship between exercise and pregnancy report no complications on maternal or fetal well-being. This is also in line with recent review studies advising that the pregnant population without obstetric contraindications should be encouraged to exercise during pregnancy. Therefore, the results of the present review stimulate those responsible for the healthcare of the pregnant woman to recommend moderate exercise throughout pregnancy without risk to maternal and fetal health.
- Exercise
- Pregnancy
Statistics from Altmetric.com
Particularities of pregnancy and childbirth
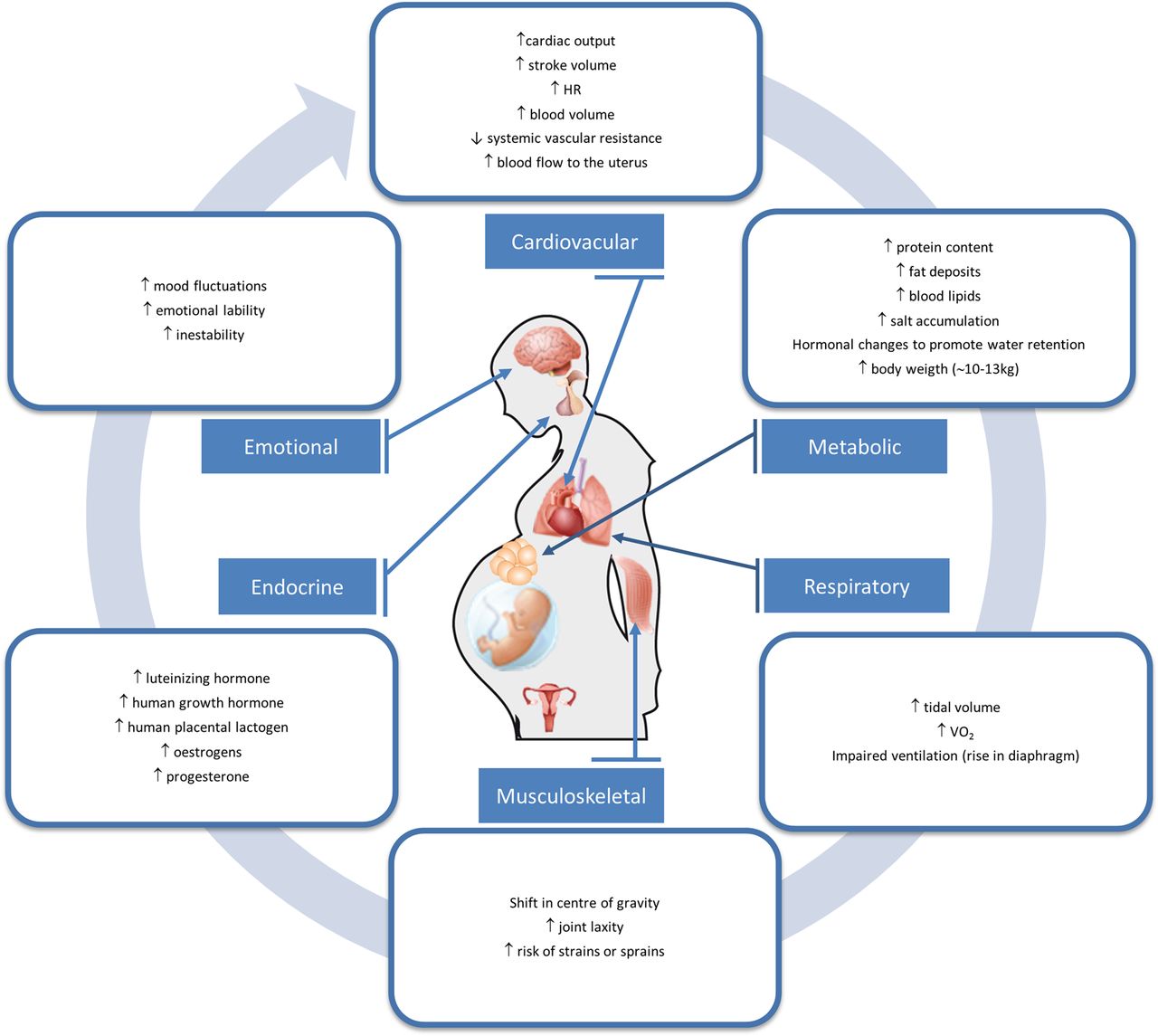
The prenatal period is a unique physiological window during which many adaptations of the mother's body are required to secure the well-being of the fetus (figure 1 for a summary).1 ,2 The success with which these are made can have major consequences for the long-term health of the child.3

Main physiological adaptations of the mother's body during pregnancy (HR, heart rate;VO2, oxygen consumption).
Cardiovascular changes begin during the fifth week of gestation and last until about a year after delivery.4–6 Cardiac output increases by about 40% (partly due to an increased stroke volume and partly to an increased heart rate) when there is only a 13% increase in the body mass to be supplied by the maternal blood.7 The blood volume also increases during pregnancy by some 40–50%,8 while the systemic vascular resistance is markedly reduced, the vascular tone falling due to high-plasma progesterone concentrations.9–11 The blood flow to the uterus is thus increased several fold.
During pregnancy, normal metabolic processes are altered to accommodate the needs of the developing fetus.2 The protein content of the maternal body tissues increases, and carbohydrates accumulate in the liver, muscles and placenta. In addition, fat deposits appear under the skin, especially around the breasts and buttocks, and elevated blood lipid and cholesterol levels are common.12 Salts of calcium, phosphorus and potassium, all essential for normal fetal development, also accumulate, and hormonal changes promote water retention.13 Maternal weight gain, normally some 10–13 kg,14 is one of the most obvious changes of pregnancy. The Institute of Medicine recommends weight gains for underweight, normal weight, overweight and obese women of 12.5–18, 11.5–16, 7–11.5 and 5–9 kg, respectively.15–17
Extensive changes occur in the respiratory system during pregnancy, including anatomical and functional alterations; these occur early on under the influence of (mainly) progesterone, even before the growing uterus mechanically impairs ventilation. The diaphragm rises by about 4 cm due to a flaring of the lower ribs.12 This helps produce the slight increase in tidal volume and oxygen consumption (VO2) noted in pregnant women, presumably to help supply the oxygen requirements of the fetus.18
The growing breast, uterus and fetus, along with increased lumbar lordosis, result in a shift in the mother's centre of gravity, which may cause balance problems.19 During pregnancy, hormonal changes are thought to induce a greater laxity of the joints, helping to soften the pubic symphysis and thus accommodate delivery. Increased joint laxity can, however, increase the risk of suffering strains or sprains.20
The hormonal changes that occur during pregnancy, modulated in part by the corpus luteum at the beginning of pregnancy, and later on by the fetoplacental unit and maternal endocrine glands,21 are responsible for many cardiovascular, respiratory and psychological changes.22 Increased levels of luteinising hormone, human growth hormone, human placental lactogen, oestrogen and progesterone are all seen during pregnancy.23
Pregnancy and childbirth have long been considered as risk factors in the genesis of pelvic floor dysfunction.24 ,25 The intra-abdominal pressure generated by the growing uterus, as well as the mechanical strain imposed by the delivery process, may cause partial denervation of the pelvic floor and injury to the muscle and connective tissue.26 ,27 Several factors such as excessive maternal weight gain, fetal macrosomia, instrumental delivery or prolonged labour have traditionally been considered predisposing factors for pelvic floor injury,24 ,28 with the most common pelvis floor disorder being urinary incontinence.28
Pregnancy can also be a time of major emotional change. Many women suffer alterations in mood and even prenatal depression.29 According to the WHO (2002), 22% of women of childbearing age have suffered depression at some point in their lives, with pregnancy making them more vulnerable compared with other times.30 In fact, recent studies have estimated the prevalence of depression during pregnancy to be between 10% and 30%,31 higher than that recorded during the postpartum period.32
Exercise and pregnancy
Physical exercise has become more popular among women of fertile age, and many now seek medical advice on whether they can continue exercising during pregnancy.33 The answer to their question demands that the influence of exercise on the mother and the fetus be properly understood.34 Recommendations regarding exercise during pregnancy have long been based more on social and cultural notions or ‘common sense’ than any hard scientific evidence.22 Indeed, the evidence on which they might be based is not particularly clear: studies on the effects of exercise on maternal and fetal health have been around for 30 years, yet controversy still surrounds how it affects many pregnancy outcomes, including gestational age at birth, the type of delivery, maternal weight gain or birth weight, among other outcomes.35 The reason for this lies partly in that observational studies have made much use of questionnaires—which are now known not to be very reliable in the assessment of physical activity—while experimental studies have involved such a range of type, duration and intensity of exercise that comparisons between them have been difficult.36
Effects of exercise during pregnancy on maternal and fetal well-being
Hormonal and metabolic
The growing fetus requires an adequate supply of nutrients,13 yet even the mildest form of acute exercise requires an increase in glucose uptake to the muscles. It is reported that acute exercise (as opposed to exercise training) in pregnant women is associated with increased sympathoadrenal and neurohumoral activity, resulting in reduced plasma insulin and increased norepinephrine, epinephrine, cortisol, glucagon and growth hormone concentrations.12 ,37 Soultanakis et al38 compared the effect of 60 min of moderate-intensity exercise on glucose homeostasis in non-pregnant and pregnant women in their third trimester, measuring the rate at which, and the extent to which, blood glucose decreased, along with changes in lactate, β-hydroxybutyrate, free fatty acids (FFA) and insulin (all of which affect glucose homeostasis). Compared with the non-pregnant women, the blood glucose levels of the pregnant women were seen to decrease at a faster rate and to a significantly lower level post-exercise. Their insulin levels also decreased to a significantly lower level post-exercise, as did their lactate levels (but only for 15 min). No difference was seen between the two groups in terms of their β-hydroxybutyrate levels. In a randomised clinical trial (RCT) involving 83 healthy pregnant women, Barakat et al39 examined the influence of a moderate-intensity exercise intervention over the entire pregnancy period on maternal glucose tolerance. The exercise group returned better maternal glucose screen results (103.8±20.4 mg/dL) than the control group (126.9±29.5 mg/dL). Bessinger et al40 examined substrate utilisation and hormonal responses to moderate-intensity exercise in a group of 12 women over gestation, measuring glucose, triglyceride, insulin, glucagon, cortisol, growth hormone and blood urea levels, as well as heart rate, VO2 and the respiratory exchange ratio at rest and after exercise. Urine urea, urine volume and creatinine levels were also measured 24 h before and after exercise. Pregnancy was associated with elevated resting triglyceride levels but a lower plasma glucose level. No significant differences were seen before and after exercise for most of the variables studied. It was concluded that substrate and hormonal responses to exercise are altered as pregnancy progresses, and that the reduced blood glucose level associated with exercise might be due more to impaired gluconeogenesis and glycogenolysis than any increase in glucose utilisation caused by exercise.
Fetal growth and development
Hopkins et al41 examined whether aerobic exercise training in the second half of pregnancy might be associated with reduced fetal size via changes in the maternal insulin-like growth factor (IGF) axis (which involves placental growth hormone), or via alterations in the plasma leptin or FFA concentrations. Training appeared to have no impact on the IGF axis, but the women in the exercise group experienced a 29% increase in plasma leptin concentration during late gestation and showed a trend towards lower FFA levels. The authors concluded that this increase in leptin might reflect subtle changes within the placenta in response to regular exercise, and that this might have contributed to the reduction seen in the size and birth weight of the children they bore.
Studies on the effect of physical exercise on fetal growth and development have reported varying results, perhaps again because of the variety of designs used and the different interventions followed (type, intensity, duration and frequency of maternal exercise). Some studies report poorer growth in infants of physically active mothers,42–45 while others report the opposite,46 and yet others report no difference at all.47 ,48 In an RCT to determine the effects of aerobic exercise training during the second half of pregnancy on maternal insulin sensitivity and neonatal outcomes, Hopkins et al44 observed lower birth weights and body mass indices at birth for the offspring of mothers who exercised. Clapp et al49 ,50 reported a positive association between early and regular physical exercise during normal pregnancy and improved fetoplacental growth. Some authors suggest that maternal exercise during pregnancy has no adverse effects on infants during their first year of life,51 nor does it affect children's subcutaneous fat mass 5 years after delivery.52 In a cohort study with follow-up at 1 year, Edwards43 found exercise during pregnancy to have no influence on morphometric variables or cognitive performance as measured with the Bayley mental scale.
Respiratory
The respiratory response to maternal exercise is particularly related to hormonal factors. In theory, changes in the endocrine system during pregnancy could lead to changes in breathing responses, perhaps even limiting exercise capacity.53 It has been suggested that hormonal changes and respiratory responses to exercise may also be partly responsible for pregnant women's perception of having to make an increased effort during exercise.54 However, Jensen et al53 report pregnancy and advancing gestation not to be associated with increased exertional respiratory discomfort, nor any reduction in aerobic work capacity, and indicate that mechanical adaptations during pregnancy help pregnant women achieve a peak oxygen consumption (VO2peak) similar to that of non-pregnant women. Jensen et al55 also studied the physiological mechanisms of exertional breathlessness in responses to incremental cycle exercise in 15 young, healthy women 34–38 weeks into gestation, and again 4–5 months into the postpartum period. Pregnancy-induced increases in exertional breathlessness were found to reflect an increased ventilation and respiratory muscle effort, and dynamic mechanical ventilatory constraints contributed to respiratory discomfort near the limits of tolerance in late gestation. In an experimental study in 28 previously sedentary pregnant women, McAuley et al56 examined the effects of aerobic conditioning during the second and third trimesters on ventilatory responses. The results showed that regular maternal exercise had no significant effect on pregnancy-induced changes in ventilation or alveolar gas exchange at rest or during standard submaximal exercise. In the authors’ opinion, prenatal fitness programmes improve the workload capacity, as shown by the improvement in ventilation and peak oxygen pulse values. Wolfe et al57 reported similar results. In a study designed to examine the size of the increased ventilatory response to exercise in pregnancy, Jensen et al58 reported the variation in this variable, as well as the perceived breathlessness among healthy pregnant women, to be explained by interindividual variation in the ventilatory recruitment threshold for CO2.
Cardiovascular
Pivarnik et al59 found that the cardiorespiratory response to acute exercise in pregnant women who were physically active throughout pregnancy was better than in women who remained inactive during gestation. Veille et al60 studied left ventricular diastolic filling in response to exercise (stationary bicycle exercise) by transmitral pulsed Doppler echocardiography in 10 healthy pregnant women during each trimester of pregnancy, and again at 12 weeks after delivery. Measurements were made at rest and during exercise at each workload. Pregnancy increased the early and atrial peak flow velocities and reduced the P-R interval, the early deceleration time and the isovolumetric relaxation time. The authors concluded that the responders experienced an increase in left ventricular chamber stiffness during maximum intensity exercise. Morrow et al61 studied maternal heart rate and blood pressure (BP), and the uteroplacental/umbilical circulation (by Doppler ultrasound) in 15 healthy, pregnant women who undertook a 5 min exercise period in late pregnancy. Maternal heart rate and BP were increased by the exercise, as was the ratio of the systolic/diastolic velocity in the uterine artery. This suggests an increase in uteroplacental vascular resistance. The fetal heart rate was also increased by the exercise, but the systolic/diastolic velocity ratio in the umbilical artery remained unaltered. These authors concluded that exercise generates resistance to blood flow in the uterine circulation. In a recent longitudinal study involving 27 healthy, nulliparous, pregnant women, Ferreira et al62 examined whether maternal heart rate and BP changed in response to pelvic floor muscle training during pregnancy. Systolic and diastolic BP were measured before and after each training session and maternal heart rate was measured during each session. The intervention programme followed involved individual supervised pelvic floor muscle training between gestational weeks 20–36. The authors reported that this had no effect on BP but significantly increased the heart rate during the exercise session, with no negative long-term effect on either of these variables. In a prospective study involving 22 sedentary normal weight, overweight and obese pregnant women, Stutzman et al63 investigated the effect of an exercise programme on BP and cardiac autonomic function as determined by heart rate variability (heart rate) and baroreflex sensitivity (BRS). The exercise programme consisted of walking (low-intensity exercise) for 16 weeks (from week 20 of pregnancy onwards). The BP, heart rate and BRS were measured at rest and at the beginning of exercise both at the beginning and end of the experimental period. Increases were seen in BP, heart rate and BRS, particularly in the overweight women. It was suggested that exercise training might attenuate the increase in BP and the loss of parasympathetic tone associated with pregnancy, especially in overweight women.
Psychological
Pregnancy is a time during which emotional balance and psychological stability can be at risk. Depression can be difficult to treat in pregnant women given the need to avoid possible adverse effects such as impaired fetal brain development,64–66 preterm delivery or intrauterine growth restriction,67–69 postpartum depression and its related complications, mother–infant bonding difficulties,70 infant feeding difficulties and childhood overweight problems,71 low birth weight or longer hospital stays.70 Theoretically, improvements in mood and self-esteem generated by exercise might mitigate this problem and improve body satisfaction.72 Certainly, this association has been shown in some studies.73 ,74 Other studies have shown that exercise during pregnancy improves depression-related symptoms.75–77 In a recent RCT, Perales et al78 found that a programme of physical exercise throughout pregnancy attenuated such symptoms in otherwise healthy, pregnant women.
Pelvic Floor
Some studies have reported a beneficial effect of programmes aiming at strengthening the pelvic floor muscles during pregnancy in symptoms of urinary incontinence.79–83 Further, a systematic review by Mørkved and Bø84 showed a positive effect of specific pelvic floor muscle training during pregnancy in the prevention and treatment of urinary incontinence. Yet such types of training programmes would not be as effective if they are simply included within general fitness classes for pregnant women with no individual instructions and specifications regarding the correct contraction of pelvic floor muscles.85 In a recent study on complications to the opening of the pelvic floor during labour (levator hiatus muscle action), Bø et al86 reported no differences in women exercising regularly before or during pregnancy compared with their non-exercising referents.
Figure 2 shows a summary of the main effects of exercise during pregnancy on maternal and fetal well-being.

{kind=link}
{kind=link}
Main effects of exercise during pregnancy on maternal and fetal well-being (BP, blood pressure; HR, heart rate; O2, oxygen).
Effects of exercise on maternal outcomes of pregnancy
Examining pregnancy outcomes is the most reliable way of determining whether pregnancy and childbirth have been successful. The most important maternal outcomes are discussed below.
Maternal weight gain
This varies widely among pregnant women,87 but a very high-percentage gain excessive weight.88 ,89 Unfortunately, this is associated with hypertension, gestational diabetes and fetal macrosomia.88 ,90–92 Exercise may help in the control of maternal weight gain,93–95 and may help in its treatment in overweight and obese pregnant women.96
Gestational age at delivery
Sufficient time is required for the organs and systems of the fetus to reach maturity.97 It has traditionally been thought that exercise, especially high-intensity exercise, might lead to earlier parturition, mainly due to hormonal factors.12 ,98 However, several recent studies suggest that moderate-intensity exercise does not lead to earlier births in healthy pregnant women.36 ,99–101
Type of delivery
The mode of delivery can affect the well-being of the mother and the newborn. Instrumental delivery or Caesarean section can have many sequelae that condition postpartum recovery. While earlier studies found no influence of exercise on type of delivery,102 ,103 more recent studies suggest that an association exists between exercise during pregnancy and a reduced need for Caesarean section.104 ,105
Duration of labour
The duration of childbirth can affect the well-being of both the mother and the newborn.106 Prolonged labour is associated with increased maternal and perinatal morbidity and mortality.107–109 Identified maternal morbidities include maternal exhaustion, electrolyte imbalance, hypoglycaemia, obstructed labour and its sequelae (such as uterine rupture, primary postpartum haemorrhage) and obstetric fistula. Prolonged labour can also cause fetal distress, perinatal asphyxia, the need for neonatal resuscitation and admission into a neonatal intensive care unit, hypoxic ischaemic encephalopathy and cerebral palsy.110 In theory, physical fitness could positively influence the course of labour by reducing excessive weight gain and inducing metabolic and hormonal changes that may impact uterine contractility and endurance.111 Ruiz et al95 found no effect of light-intensity to moderate-intensity aerobic and resistance exercise on duration of labour in 481 pregnant women who exercised from the ninth week of pregnancy compared with their counterparts (n=481) who did not exercise.
Future perspectives
Much controversy remains regarding the effects of exercise during pregnancy. It is important that studies be performed using standardised protocols that would allow later comparisons of the results obtained by different authors. The undertaking of such studies, especially RCTs, might afford more reliable answers. Currently, it would appear that moderate exercise performed throughout pregnancy is beneficial to the mother while having no adverse effects on the growing fetus.
What are the new findings?
In the absence of obstetric complications, the healthy pregnant body is able to cope with the physiological demands imposed by moderate exercise.
Moderate exercise is not a risk factor for fetal and maternal pregnancy outcomes.
A supervised programme of moderate exercise throughout pregnancy may be recommended by health professionals to attenuate the risk of pregnancy alterations.
References
Footnotes
Funding This study was partially supported by the Spanish Ministry of Economy and Competitiveness (RYC-2010-05957) and Technical University of Madrid (AL15-PID-06). Research in the field of exercise and health by Alejandro Lucia is funded by the Fondo de Investigaciones Sanitarias (FIS, grant number PI12/00914) and fondos FEDER.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.