Article Text

Abstract
Medial tibial stress syndrome (MTSS) is a common injury in runners and military personnel. There is a lack of agreement on the aetiological factors contributing to MTSS, making treatment challenging and highlighting the importance of preventive efforts. Understanding the risk factors for MTSS is critical for developing preventive measures. The purpose of this systematic review and meta-analysis was to assess what factors put physically active individuals at risk to develop MTSS. Selected electronic databases were searched. Studies were included if they contained original research that investigated risk factors associated with MTSS, compared physically active individuals with MTSS and physically active individuals without MTSS, were in the English language and were full papers in peer-reviewed journals. Data on research design, study duration, participant selection, population, groups, MTSS diagnosis, investigated risk factors and risk factor definitions were extracted. The methodological quality of the studies was assessed. When the means and SDs of a particular risk factor were reported three or more times, that risk factor was included in the meta-analysis. There were 21 studies included in the systematic review and nine risk factors qualified for inclusion in the meta-analysis. Increased BMI (weighted mean difference (MD)=0.79, 95% CI 0.38 to 1.20, p<0.001), navicular drop (MD=1.19 mm, 95% CI 0.54 to 1.84, p<0.001), ankle plantarflexion range of motion (ROM; MD=5.94°, 95% CI 3.65 to 8.24, p<0.001) and hip external rotation ROM (MD=3.95°, 95% CI 1.78 to 6.13, p<0.001) were risk factors for MTSS. Dorsiflexion and quadriceps-angle were clearly not risk factors for MTSS. There is a need for high-quality, prospective studies using consistent methodology evaluating MTSS risk factors. Our findings suggest that interventions focused on addressing increased BMI, navicular drop, ankle plantarflexion ROM and hip external rotation ROM may be a good starting point for preventing and treating MTSS in physically active individuals such as runners and military personnel.
- Lowever extremity
- Running
- Injury
Statistics from Altmetric.com
Introduction
Medial tibial stress syndrome (MTSS) is one of the most frequently reported injuries in physically active populations. A recent systematic review of three prospective studies reported an incidence rate ranging from 13.6% to 20% in runners.1 MTSS is also common in military personnel with a reported incidence ranging from 7.2% to 35%.2–4 Although a frequently reported injury, the treatment of this condition is challenging due to a lack of consensus on aetiological factors.5
Without a full understanding of aetiological factors, an emphasis on preventive efforts is particularly important. Understanding MTSS risk factors is critical for developing preventive measures.6 Risk factors for MTSS have been studied in numerous individual studies. Researchers have examined many variables as potential risk factors for MTSS such as body mass index (BMI),4 ,7–9 bone geometry,10 gait kinematics,[11–14 leg length differences,12 navicular drop,9 ,15–20 range of motion (ROM),4 ,8 ,9 ,11 ,12 ,14 ,16 ,18 ,21 training history4 ,18 ,19 ,22 and others. Although the results of these individual studies can inform clinical practice, the reported findings are often based on small sample sizes with conflicting results. Studying the potential risk factors in a systematic fashion can reduce bias and increase confidence through the analysis of pooled data. The purpose of this systematic review and meta-analysis was to assess what factors put physically active individuals at risk to develop MTSS.
Methods
Inclusion and exclusion criteria
For inclusion in this systematic review, studies were original research that investigated risk factors associated with MTSS, compared physically active individuals with MTSS to physically active individuals without MTSS, were in the English language and were accessible full papers in peer-reviewed journals.
Search strategy and study selection
The Database of Abstracts of Reviews of Effects (DARE) and the Cochrane Database of Systematic Reviews (CDSR) were searched for systematic reviews about risk factors associated with MTSS. The Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (OVID SP), EMBASE and CINAHL were searched to identify studies that met the inclusion criteria. Reference lists of included or other relevant articles (e.g., recent reviews) were scanned and/or hand searched for additional references. Reference lists of articles that were identified via a hand search were also searched for additional references.
The initial search was carried out from the earliest date to January 2012 using key words (MeSH and/or text words) within three groups: group 1 terms pertained to injury, group 2 terms pertained to risk factors and group 3 terms pertained to population. The key words for each group were: group 1—medial tibial stress syndrome, mtss, medial tibial stress, shin splint$, shin pain; group 2—risk factor$, risk, vulnerability factor$, risk indicator$, risk characteristic$, predictor$, disorder predictor$; group 3—run$, physically active, athlete$, exercise, conditioning, military, militaries, military personnel, recruit, armed forces. The terms within each group were linked with ‘OR’ and the individual group searches were combined using ‘AND.’ Owing to the time that elapsed between the initial search and completion of our analysis, additional searches of CINAHL and MEDLINE (OVID SP) were performed in September 2012 and July 2013 to ensure that papers published from January 2012 to July 2013 were included in the systematic review.
The two reviewers (KCHB and KLH-W) independently screened titles and/or abstracts of studies identified using the search strategy noted above. If it was clear that the study did not meet the inclusion criteria, it was eliminated from the analysis. The reviewers documented a decision for each article and noted why citations were rejected: clearly not relevant or addressed the topic but failed to meet one or more inclusion criteria (recording what inclusion criteria it failed to meet). When no abstract was available or if it was unclear if the study should be a part of the systematic review, full-text articles were retrieved and independently reviewed to determine inclusion or exclusion. Any disagreement between the reviewers was discussed and resolved by consensus.
Data extraction
Data on research design, study duration, participant selection, population, groups, MTSS diagnosis, investigated risk factors, risk factor definitions, means, SDs, CIs, effect sizes, ORs and any other data the reviewers deemed relevant were extracted and summarised in Excel from all included studies. If continuous data were not reported by the authors, the reviewers contacted the authors requesting the data. Authors were contacted a minimum of two times via email and/or phone requesting data. If the authors did not respond, their manuscript was not included in the meta-analysis. Each reviewer independently extracted the data, checked their extraction for accuracy and completeness and then compared their findings with one another. When authors reported SEs, the reviewers converted them to SDs. For goniometry measurements that were reported from 180°, reviewers converted the measure so that all goniometry measures began at 0°. Any disagreements between the reviewers were discussed and resolved by consensus.
Quality assessment
The methodological quality of included studies was assessed to determine bias using an adapted23 ,24 checklist by van der Worp et al25 (table 1). This checklist was selected because it contains items for multiple study designs (cross-sectional, case–control and prospective cohort studies) and assessed risk factors for an injury similar to that reported in the current study. The checklist contains five categories: study objective, study population, outcome measurements, assessment of the outcome, and analysis and data presentation. Every item was scored as positive (+), indicating that the criterion was met, or negative (−) when the criterion was not met. Two reviewers (KCHB and KLH-W) independently evaluated the included studies using this checklist and compared the findings. Any disagreements between the reviewers were discussed and resolved by consensus. The total quality score of each study was calculated by counting the number of positive scores on items 3–16, which addressed validity/precision.
Checklist for the assessment of methodological quality of cross-sectional studies, case–control studies and prospective cohort studies
Data analysis
After data extraction, the reviewers categorised common variables into the following risk factor categories: arch height or angle, BMI, bone parameters, calcaneus and rearfoot position and displacement, calf girth, demographics, flexibility/ROM, foot posture index,26 forefoot position, gait variables, leg angle and tibia angle,18 ,19 medical history and symptoms, Ober's test,27 strength, structure/alignment, and training variables/fitness level. When the means and SDs of a particular risk factor were reported three or more times, that risk factor was included in the meta-analysis. While meta-analytic statistical indices can be calculated with as few as two studies, the stability and interpretability of estimates based on so few data points are problematic. A cut-off of three studies was chosen so that the review could be as comprehensive as possible, and the results still reasonably reliable. For the meta-analysis, weighted mean differences (MDs) and 95% CI were calculated. MD is a measure of the difference between individuals with MTSS and those without MTSS for the specific risk factor being analysed. The weighted MD pools results of studies that used the same outcome measure in a manner that weights the results of each study using the inverse variance method, i.e., the variance reported for a study is assumed to be inversely proportional to its importance.28 Heterogeneity was assessed using I2, which measures the degree of inconsistency across studies in a meta-analysis.29 A value of 25%, 50% and 75% indicates low, moderate and high levels, respectively, of heterogeneity in a sample.29 Fixed effects models were used for analyses in which I2 was less than 20% (low); random effects models for I2 greater than or equal to 20%. MIX V.2.0 (Bax L: MIX V.2.0. Professional software for meta-analysis in Excel. V.2.0.1.4. BiostatXL, 2011; http://www.meta-analysis-made-easy.com) was used to calculate MDs and I2.
Results
Search results
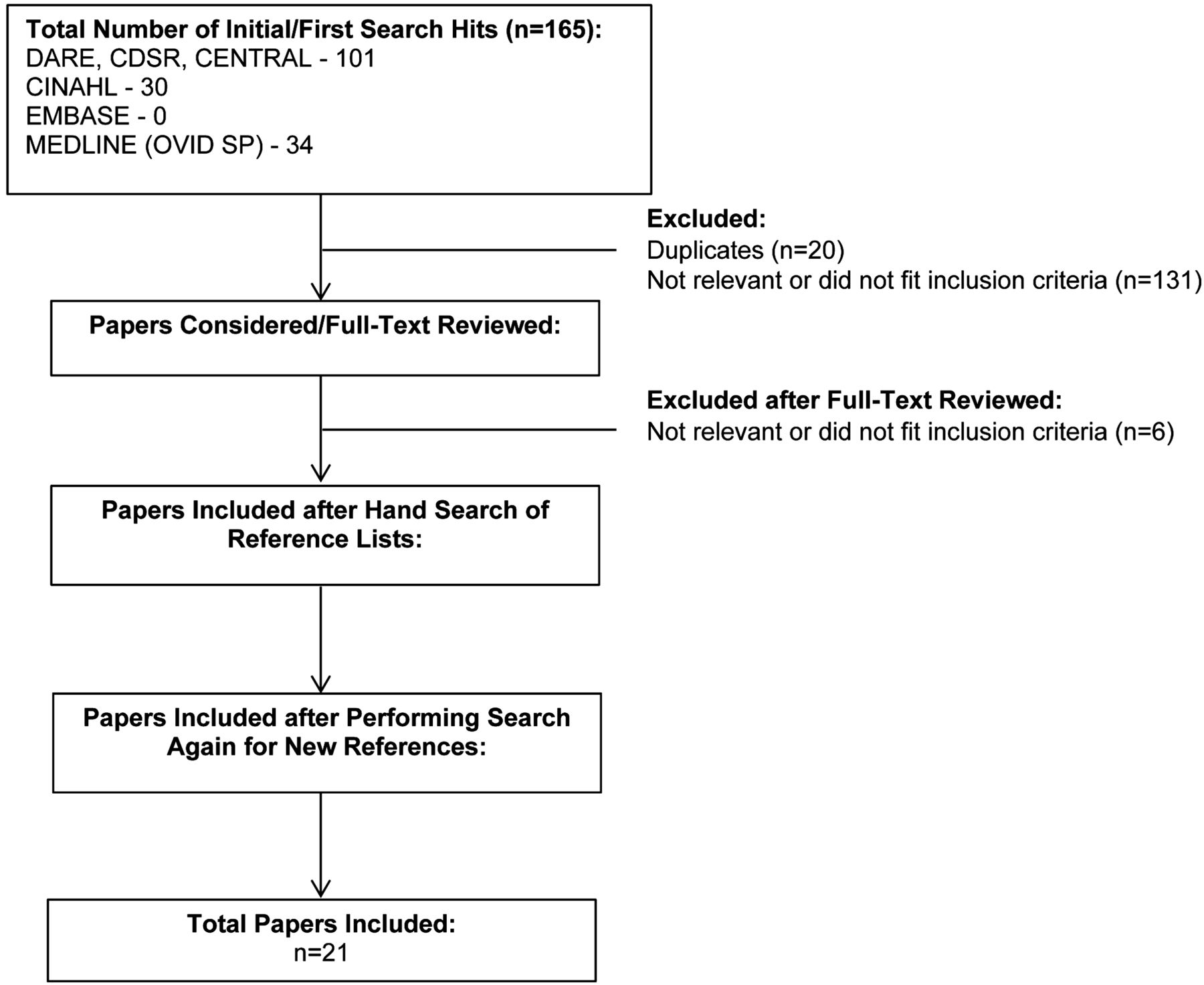
No systematic reviews were found on risk factors for MTSS. A total of 165 papers were found. After removing duplicates, eliminating papers that did not fit the PICOS (patient, intervention, comparison, outcome, study design) question, and hand searching reference lists, a total of 21 original research papers were included in the systematic review (figure 1).

Search process flow chart.
Study characteristics
The 21 included studies consisted of three cross-sectional,10 ,21 ,30 nine case–control7 ,8 ,11–15 ,20 ,31 and nine prospective cohort studies.2–4 ,9 ,16–19 ,22 In seven of the 21 studies, the participants were recreational athletes/physically active.7 ,10 ,11 ,14 ,15 ,20 ,30 In five of the studies, the participants were runners.9 ,12 ,13 ,16 ,22 In five of the studies, the participants were in the military.2–4 ,8 ,31 In two of the studies, the participants were high school or college athletes.18 ,21 Also, in two of the studies, the participants were college students enrolled in a physically active course.17 ,19 Online supplementary appendix 1 lists the 21 studies and the risk factors measured within the studies. Online supplementary appendix 2 provides the characteristics of the 13 studies included in the meta-analysis.4 ,7–12 ,14–20
Quality assessment
The scores of the individual studies on the methodological quality assessment list are presented in table 2. The average score was 48.95±16.48%. Quality assessment scores for the cross-sectional studies ranged between 3 and 7 out of a possible 12 points (25–58%); case–control studies ranged between 2 and 4 out of a possible 8 points (25–50%); and prospective cohort studies ranged between 3 and 7 out of a possible 9 points (25–78%).
Scores on the items of the quality assessment list (see table 1), with the total quality score for all positive (+) items (#3–16) and the percentage of the maximum attainable score (%)
Risk factors for MTSS
Continuous data for the following risk factors were reported three or more times and included in the meta-analysis: BMI, navicular drop, ankle plantarflexion ROM, hip external rotation ROM, ankle dorsiflexion ROM, quadriceps-angle (Q-angle), hip internal ROM, ankle inversion ROM and ankle eversion ROM. Over 100 other risk factors were reported within the 21 studies; however, none were measured consistently in more than two studies with the majority of the risk factors reported by one author. Owing to the heterogeneity of the remaining risk factors, no moderate to strong evidence exists that the risk factors not included in the meta-analysis contribute to MTSS.
Body Mass Index
Individuals with MTSS had a significantly greater BMI compared with controls (MD=0.79, 95% CI 0.38 to 1.20, p<0.001, I2=0.00%; figure 2). The meta-analysis included a total of 451 participants (187 MTSS, 264 control). There were four studies that evaluated BMI as a risk factor for MTSS; on average, these studies reached 59% of the maximal attainable score on the quality assessment (table 2).4 ,7–9 Yagi et al9 reported BMI for males and females separately, so males and females were treated as discrete data sets for a total of five data sets in the meta-analysis. One study did not report control group SDs.4 After multiple attempts to reach the authors to obtain these data, the SD of the MTSS group was used for the control group. This approach was taken because Yates and White4 assessed group differences using t tests, which assume equal variances in groups. Owing to the low heterogeneity of the sample, sexes were pooled when conducting the meta-analysis. In two of the five data sets, greater BMI increased the risk for MTSS; one study reported an effect in high school female runners (adjusted OR=0.51, 95% CI 0.31 to 0.86, p=0.01)9 and the other reported one in male soldiers (MTSS: 23.8±2, control: 22.5±1.6, p=0.04).8 In the other data sets, BMI was generally greater but not significantly different between the MTSS and control groups in adult patients,7 naval recruits4 and high school male runners.9

Effects of body mass index on medial tibial stress syndrome (MTSS).
Navicular drop
Individuals with MTSS had a significantly greater navicular drop compared with controls (MD=1.19 mm, 95% CI 0.54 to 1.84, p<0.001, I2=40.19%; figure 3). The meta-analysis included a total of 564 participants (198 MTSS, 366 control). Six studies measured navicular drop as a risk factor for MTSS.9 ,15 ,16 ,18–20 Studies with male and female groups were treated as separate and unique data sets, while studies with both limbs19 and multiple measurement types (dynamic/static)20 only included right limb and static measures, respectively. There was a total of seven data sets for the meta-analysis. In three of these data sets, the authors reported navicular drop to be the risk factor for MTSS in recreational athletes,15] high school cross-country runners16 and recreational runners.19 In the other four data sets, navicular drop was generally greater but not significantly different in the MTSS versus control groups in high school runners,9 collegiate athletes18 and recreationally active individuals.20

Effects of navicular drop on medial tibial stress syndrome (MTSS).
Ankle plantarflexion ROM
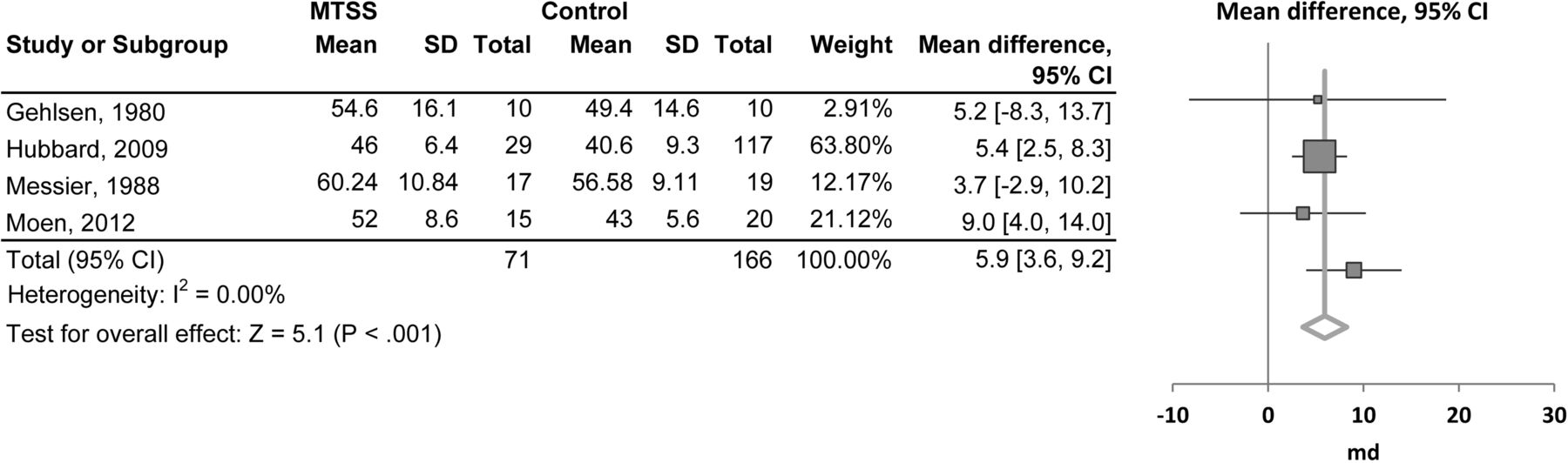
Individuals with MTSS had a significantly greater plantarflexion ROM compared with controls (MD=5.94°, 95% CI 3.65 to 8.24, p<0.001, I2=0.00%; figure 4). The meta-analysis included a total of 237 participants (71 MTSS, 166 control). Four studies measured plantarflexion as a potential risk factor for MTSS.8 ,11 ,12 ,18 Gehlsen and Seger11 reported right and left limbs separately; only right limb data were used, providing a total of four data sets for the meta-analysis.8 ,11 ,12 ,18 Sex, type of ROM (passive or active) and testing position of the participants (knees extended or flexed) were inconsistently reported in these studies, but owing to the low heterogeneity of the sample, sex, type of ROM and testing positions were pooled when conducting the meta-analysis. In a group of collegiate athletes from various division one and two teams, those with MTSS had significantly more plantarflexion compared with the healthy control group (MTSS: 46.0±6.0, 95% CI 43.5 to 48.4; control: 40.6±9.3, 95% CI 38.8 to 42.2).18 Increased plantarflexion was also significantly associated with MTSS in male soldiers (MTSS: 52±8.6, control: 43±5.6, p=0.001; multivariate regression 95% with a 95% CI of 0.5–0.9).8 In recreational and competitive runners, plantarflexion ROM was greater but not significantly different between the MTSS and control groups (MTSS: 60.24±2.63, control: 56.58±2.09).12 Similarly, although not statistically significant, female athletes with MTSS had greater plantarflexion than female athletes without MTSS (MTSS—right limb: 54.6±16.1, left limb: 52.1±18.5; control—right limb: 49.4±14.6, left limb: 46.8±14.3).11

Effects of plantarflexion range of motion on medial tibial stress syndrome (MTSS).
Hip external rotation ROM
Individuals with MTSS had a significantly greater hip external rotation ROM compared with controls (MD=3.95°, 95% CI 1.78 to 6.13, p<0.001, I2=0.00%; figure 5). The meta-analysis included a total of 279 participants (117 MTSS, 162 control).Three studies measured hip external rotation as a potential risk factor for MTSS.8 ,9 ,21 However, one study had incomplete data and was not included in the meta-analysis.21 Yagi et al9 reported male and female results separately; these results were treated as two data sets to provide a total of three data sets for the meta-analysis.8 ,9 Owing to the low heterogeneity of the sample, sexes and testing positions were pooled when conducting the meta-analysis. Moen et al8 measured passive hip external rotation in male soldiers with participants supine and the hip and knee flexed to 90°, while Yagi et al9 measured high school runners seated with the knee flexed to 90°. Yagi et al9 did not explicitly state if the passive or active ROM was measured, but their methodology suggests passive. Neither Moen et al8 nor Yagi et al9 reported significant differences between the MTSS and control groups in hip external rotation; however, mean values for hip external rotation were greater in the MTSS versus control groups for all three data sets.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of hip external rotation range of motion on medial tibial stress syndrome (MTSS).
Ankle dorsiflexion ROM
Dorsiflexion ROM was not significantly different between individuals with MTSS and controls (MD=−0.01°, 95% CI −0.96 to 0.93, p=0.98, I2=17.89%). The meta-analysis included a total of 481 participants (173 MTSS, 308 control). Eight studies measured dorsiflexion as a potential risk factor for MTSS.4 ,8 ,9 ,11 ,12 ,16 ,18 ,21 Several data sets from these studies were not included in the meta-analysis for the following reasons: Lilletvedt et al21 had incomplete data, so they were not used; Gehlsen and Seger11 reported right and left limbs separately, so only right limb data were used; Bennett et al16 and Yates and White4 reported limbs without identifying right and left limbs, so no data were included; Yagi et al9 reported dorsiflexion in two different positions, so only dorsiflexion measures taken with the knee extended were used. A total of six full data sets were used for the meta-analysis. Owing to the low heterogeneity of the sample, sexes and type of ROM (passive and active) were pooled when conducting the meta-analysis. None of the results within the individual studies supported dorsiflexion ROM as a risk factor for MTSS.4 ,8 ,9 ,11 ,12 ,16 ,18 ,21
Q-angle
Individuals with MTSS did not have significantly different Q-angles compared with controls (MD=−0.22°, 95% CI −0.95 to 0.50, p=0.54, I2=5.23%). The meta-analysis included a total of 346 participants (132 MTSS, 214 control). Three studies reported Q-angle as a potential risk factor for MTSS.9 ,12 ,19 Yagi et al9 reported male and female data separately and Raissi et al19 reported data from right and left limbs; only right limb data were included,9 providing four distinct data sets for the meta-analysis. None of the three individual studies reported Q-angle as a risk factor for MTSS.
Hip internal rotation ROM
Hip internal rotation ROM was not significantly different between individuals with MTSS and controls (MD=0.18°, 95% CI −5.37 to 5.73, p=0.95, I2=83.74%). The meta-analysis included a total of 279 participants (117 MTSS, 162 control). Three studies measured hip internal rotation as a potential risk factor for MTSS.8 ,9 ,21 One study had incomplete data and was not included in the meta-analysis.21 Yagi et al9 reported male and female results separately; these results were treated as two data sets to provide a total of three data sets for the meta-analysis.8 ,9 Moen et al8 measured passive hip internal rotation with participants supine and the hip and knee flexed to 90° and found that decreased hip internal rotation was significantly associated with MTSS in male soldiers (MTSS: 40±9.3, control: 47±8.7, p=0.087; multivariate regression 95% 1.2 (1.0 to 1.4)).8 Yagi et al9 measured participants seated with the knee flexed to 90° in high school runners. Yagi et al9 did not explicitly state if passive or active ROM was measured, but their methodology suggests passive. They state in their manuscript that decreased hip internal rotation increased the risk for MTSS in females.9 However, their data suggest that female high school runners with MTSS actually had an increased hip ROM compared with a control group (MTSS females: 31.1±9.9, control females: 25.5±9.5; p<0.05).9 More studies using similar methodology are needed to more accurately evaluate the role of hip internal rotation in MTSS.
Ankle eversion ROM
Ankle eversion ROM was not significantly different between individuals with MTSS and controls (MD=1.17°, 95% CI −0.02 to 2.36, p=0.06, I2=31.58%). The meta-analysis included a total of 281 participants (108 MTSS, 173 control). Five studies measured eversion as a potential risk factor for MTSS.8 ,11 ,14 ,18 ,21 One study had incomplete data and was not included in the meta-analysis.21 Gehlsen and Seger11 analysed right and left limb ROM separately; only right limb data were used, providing a total of four data sets for the meta-analysis. Viitasalo and Kvist14 found an increased eversion ROM in the MTSS compared with the control group (MTSS: 10.7±4.4, control: 8.3±3.2; p<0.05). No other studies within the meta-analysis reported eversion as a risk factor for MTSS. More studies utilising a similar methodology and populations are needed to determine if ankle eversion is a risk factor for MTSS.
Ankle inversion ROM
Ankle inversion ROM was not significantly different between individuals with MTSS and controls (MD=0.98°, 95% CI −3.11 to 5.07, p=0.64, I2=71.58%). The analysis included a total of 249 participants (89 MTSS, 160 control). Five studies measured inversion as a potential risk factor for MTSS.8 ,11 ,14 ,18 ,21 One study had incomplete data and was not included in the meta-analysis.21 Gehlsen and Seger11 measured right and left limb ROM; only right limb data were used, providing a total of four data sets for the meta-analysis. Neither the type of ROM (passive or active) nor the position of the participants being measured was consistently reported in these studies. Additionally, within the individual studies, there were conflicting results. Inversion ROM was not a risk factor for MTSS in collegiate athletes (MTSS: 31.9±6.8, control: 30.6±8.1; p=0.45)18 or male army recruits (MTSS: 30±5.4, control: 30±5; p=0.17).8 However, Gehlsen and Seger11 reported significantly increased right inversion in the control versus MTSS group (MTSS: 28.6±17.4, control: 45±16; p<0.05) while Viitasalo and Kvist et al14 found greater inversion ROM in the MTSS compared with the control group (MTSS: 19.5±8.6, control: 14±4.8; p<0.01). Owing to the heterogeneity of the sample and conflicting results, it is difficult to conclude the role of ankle inversion in MTSS risk.
Discussion
The purpose of this systematic review and meta-analysis was to assess factors that place physically active individuals at risk to develop MTSS. There were 21 studies included in the systematic review. Over 100 risk factors were analysed in the 21 studies; however, only nine risk factors included the minimum data required for the meta-analysis. Of the nine risk factors analysed, individuals with increased BMI, navicular drop, plantarflexion or hip external rotation compared with their non-injured counterparts were more likely to incur MTSS. Dorsiflexion and Q-angle were most clearly not risk factors for MTSS.
When considering BMI as a risk factor for MTSS, it is important to note that research suggests BMI is a poor indication of body fat in certain populations such as athletes and military personnel.32 ,33 Within the physically active populations studied in this systematic review, BMI is not a direct measure of body fat. Rather, it suggests that those with an increased mass relative to their squared height are at greater risk for MTSS, but the increased mass could be due to lean mass or fat mass. One explanation for BMI as a risk factor for MTSS is related to the response of bone to loading, specifically tibial bowing or bending, which produces hyperstimulated periosteal activation.34 ,35 Repeated bending/microdamage causes an adaptation to the bone, strengthening it to prevent bony overload; in fact, dynamic forces, such as those produced by muscles on bone, appear to provide the greatest stimuli for osteogenesis.36 However, when loads exceed the bone's microdamage threshold, injury can occur. Males with MTSS have been found to have a smaller tibial cortical bone area and shape and females with MTSS to have a smaller tibial cortical bone shape compared with controls, but it is not known if this is a cause or an effect of the injury.10 Perhaps with an increased mass relative to height, the mechanical load on the tibia changes during physical activity. Since bone is an adaptable organism, it seems reasonable to believe that slow, steady and progressive increases in exercise would allow for the bone to adapt and those with a higher BMI may need a longer adaptation period than those with a lower BMI.
An increased navicular drop was found to be a risk factor for MTSS in our meta-analysis. Navicular drop is often used as a measure of arch height37 and foot pronation.38 An inverse relationship exists between navicular drop and arch height such that an increased navicular drop leads to lower arch height. If navicular drop is a measure of pronation, because rearfoot eversion is part of pronation,39 it makes sense that there would be a relationship between navicular drop and rearfoot eversion. Although this has been found to be true during walking,40 it does not appear to be true during running. During running, navicular drop and arch height have been found to be related to tibial internal rotation and not rearfoot eversion.41 ,42 Specifically, a less navicular drop (higher arch) was related to an increased tibial internal rotation during running.41 ,42 Pronation is thought to be a protective mechanism during running and allows for impact forces to be attenuated.43 Perhaps individuals with an increased navicular drop (lower arch height) are at risk for MTSS because they do not then have as much tibial internal rotation, which may be an important factor in absorbing impact forces, placing greater load on the tibia itself. Since navicular drop has been shown to increase with fatigue of the foot intrinsic muscles,44 foot and arch exercises to increase the rigidity of the arch may have an influence on navicular drop and tibial internal rotation and therefore be beneficial for the prevention and/or treatment of MTSS. This is an area in need of further exploration.
In addition to navicular drop, increased plantarflexion ROM was found to be a risk factor for MTSS. Of the four studies included in the meta-analysis, one measured active ROM,18 one measured passive ROM8 and the other two did not specify which makes it more challenging to understand why greater plantarflexion may be a risk factor for MTSS. Authors have postulated that increased plantarflexion leads to a greater likelihood of individuals landing on their forefoot when running8; this may increase the strain on the posteromedial tibia compared with rearfoot landing.45 Another speculation is that perhaps an increased navicular drop and increased plantarflexion ROM are related. During the first half of the stance phase of running, pronation occurs. Pronation is a combination of ankle dorsiflexion, rearfoot eversion and foot abduction.43 If an individual has an increased navicular drop (lower arch height), symbolic of greater pronation, they may push through their first ray more heavily as their arch moves closer to the floor and foot abducts during the mid-stance of the gait when they are pronating to absorb impact forces. Greater push off could lead to greater active plantarflexion ROM and a potentially increased extensibility of the dorsiflexors. The anterior tibialis is a primary dorsiflexor of the ankle and attaches to the base of the first metatarsal and medial surface of the first cuneiform. In theory, increased extensibility of this muscle, associated with greater plantarflexion ROM, could influence navicular drop due to its pull on the bones adjacent to the navicular. Eccentric exercises for the tibialis anterior to control end range plantarflexion may be an important consideration for the prevention and treatment of MTSS.
It is not clear how an increased hip external rotation ROM may put an individual at risk for MTSS as indicated in our meta-analysis. Two of the three studies in our meta-analysis reported passive ROM measures8 ,9 and the other study did not specify if passive or active ROM was measured.21 Passive hip ROM and its relationship to lower leg pain has been studied primarily in the military population. In male soldiers, decreased passive hip internal rotation has been found as a risk factor for MTSS.8 In male recruits, greater passive internal and external rotation ranges of motion were related to exertional medial tibial pain.46 Also, in male recruits, those with excessive external rotation of the hip (active or passive not specified) had higher incidences of tibia stress fractures.47 As suggested by Moen et al8 perhaps both increased and decreased ranges of motion at the hip put an individual at risk for excessive medial tibia loading. The mechanisms behind why hip ROM may be related to tibia injury are unknown. It may be that the femoral neck angle sits in an anteverted or retroverted posture,48 which changes the orientation of the femur on the tibia. Or perhaps balance between the amount of internal and external rotation and the amount of total hip ROM are key factors influencing lower leg loading. Hip ranges of motion should be a consideration of clinicians in the prevention and treatment of MTSS, but more research is needed to clarify the specific role it has as a risk factor for MTSS.
Dorsiflexion, Q-angle, hip internal rotation, ankle eversion and ankle inversion did not emerge as risk factors for MTSS in the meta-analysis. Of these, dorsiflexion and Q-angle most clearly do not appear to be risk factors for MTSS. Dorsiflexion and Q-angle were evaluated in many individuals (n=481 and 346, respectively) with very low heterogeneity in the data set. Additionally, in all of the individual studies included in the meta-analysis that measured dorsiflexion and Q-angle, none of them reported dorsiflexion or Q-angle as a risk factor for MTSS. Collectively, this strongly suggests that neither one contributes to the risk of obtaining MTSS. Hip internal rotation, ankle inversion and ankle eversion had sample sizes near 300, but had high heterogeneity and conflicting results when looking at the individual studies that measured these variables. More studies are needed using similar methodology to assess hip internal rotation, ankle inversion and ankle eversion ROM as risk factors for MTSS.
Limitations of this systematic review and meta-analysis include not all risk factors being analysed due to the lack of consistency in the >100 risk factors reported in the 21 studies. Additionally, only 10 of the 21 studies had quality assessment scores >50%. The studies used to analyse three of the four significant risk factors for MTSS (BMI, navicular drop and hip external rotation ROM), on average, scored >50% while the studies used to analyse plantarflexion ROM scored 44%. These things should be considered when reading and applying the information presented. Further research is needed on risk factors of greatest interest utilising consistent methodology and strong research designs to increase the depth of the existing literature and allow for expanded meta-analyses. Additionally, very little research has investigated the role of combined risk factors in MTSS, representing an open and valuable area for exploration.
Conclusion
In a physically active population, the primary factors that appear to put individuals at risk for MTSS are increased BMI, navicular drop, plantarflexion ROM and hip external rotation ROM. Interventions focused on addressing these risk factors may prove valuable in preventing and treating MTSS. There is a need for high-quality, prospective studies using consistent methodology evaluating MTSS risk factors that have already been explored but not in depth. This will allow for further meta-analyses and the exploration of how the presence of combined factors affects MTSS risk.
What is already known on this topic?
-
Medial tibial stress syndrome (MTSS) is a very common injury in the physically active population. Treatment of MTSS is challenging because the aetiology of the condition is unclear. Many risk factors have been studied and hypothesised to contribute to MTSS.
What this study adds?
-
This paper systematically reviews and analyses MTSS risk factors. Studying risk factors in this fashion provides a higher level of evidence than singular studies, allowing for greater confidence in understanding the primary contributors to MTSS. Knowing these primary risk factors can guide healthcare professionals in their prevention and rehabilitation efforts.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
Footnotes
-
Contributors KLH-W and KCHB planned the systematic review, conducted the search and data extraction, and drafted the manuscript. CB conducted the statistical analysis and critically reviewed the manuscript prior to submission.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.