Article Text

Abstract
Aims (1) To assess the 1-year and 6-year courses of non-traumatic knee symptoms in adolescents and young adults presenting in general practice. (2) To identify prognostic factors for persistent knee symptoms at 1-year follow-up.
Methods Adolescents and young adults (12–35 years; n=172) with non-traumatic knee symptoms were included in the cohort study by their general practitioner (GP) and followed for 6 years. Multivariable logistic regression analysis was used to identify prognostic factors for persistent knee symptoms at 1-year follow-up and the area under the receiver operating curve (AUC) was calculated.
Results Persistent knee symptoms in patients receiving a GP diagnosis of unspecified knee symptoms were reported by 41% of the patients at 1-year follow-up and by 19% of the available patients at 6-year follow-up. Patients receiving a GP diagnosis of patellofemoral pain syndrome had the worse prognosis, with 40% reporting persistent knee symptoms at 6-year follow-up.
Prognostic factors associated with persistent knee symptoms at 1-year follow-up were BMI >25, low/middle education level, bilateral symptoms and self-reported absence of crepitus of the knee (AUC 0.80) for patients receiving a GP diagnosis of unspecified knee symptoms. For patients receiving a GP diagnosis of patellofemoral pain syndrome, prognostic factors were low/middle education level, poor health, having bilateral symptoms and self-report of a swollen knee (AUC 0.76).
Conclusions The prognosis of non-traumatic knee symptoms in adolescents and young adults in general practice is not as good as was previously assumed. Several prognostic factors collected at baseline were associated with persistent knee symptoms at follow-up. However, the results should be replicated in another larger study.
- Knee
Statistics from Altmetric.com
Introduction
General practitioners (GPs) are frequently consulted by patients with non-traumatic knee symptoms. Non-traumatic knee symptoms in adolescents and young adults account for 20% of all non-traumatic knee symptoms in general practice and include patellofemoral pain syndrome,1 jumper's knee (knee extensor tendinopathy), Osgood-Schlatter disease, bursitis, iliotibial tract friction syndrome and popliteal cysts.2 The incidence of these types of symptoms in adolescents and young adults reported in general practice is about 19/1000 patients per year.2
In comparison with sports medicine, the patellofemoral pain syndrome accounts for up to 25% of all presented knee symptoms.3 ,4 To the best of our knowledge, no studies have examined the short-term and long-term follow-up and prognosis of these symptoms in adolescents and young adults in general practice.5
Therefore, this prospective cohort study was performed in general practice to assess the 1-year and 6-year courses of non-traumatic knee symptoms in adolescents and young adults, and to identify prognostic factors for persistent knee symptoms at 1-year follow-up.
Methods
Design
The present study took place within the research network HONEUR (40 GPs) established by the department of General Practice of Erasmus MC University Medical Centre. It is part of a prospective, observational cohort study (n=1068) in which consecutive patients visiting their GP with a new episode of knee symptoms were enrolled and initially followed for 1 year.6 Owing to the high percentage of persistent knee symptoms at 1-year follow-up, the follow-up period was extended to 6 years.
At baseline, new knee symptoms were defined as episodes of knee pain presented to the GP for the first time. Recurrent symptoms for which the GP was not consulted within the past 3 months were also considered to be new symptoms. Traumatic knee symptoms were defined as knee symptoms caused by a sudden impact or unexpected movement within 1 year before consulting the GP. All other knee symptoms were considered to be non-traumatic knee symptoms.
Patients were eligible for this study if they were aged 12–35 years and had consulted their GP for non-traumatic knee symptoms (unspecified knee symptoms (ICPC L15) and patellofemoral pain syndrome (ICPC L99.07). Exclusion criteria were knee symptoms that required urgent medical attention (eg, fractures, infection), patients with malignancies, neurological disorders or musculoskeletal diseases (eg, Parkinson's disease, rheumatoid arthritis, amyotrophic lateral sclerosis), as well as patients incapable of understanding the ramifications of study participation. The study protocol was approved by the Medical Ethics committee of the Erasmus MC University Medical Centre.
Data collection
Patients filled out a self-report questionnaire at baseline, at the 3, 6 and 9 months follow-up, and at the 1-year and 6-year follow-up.
The baseline and follow-up questionnaire collected data on age, gender, socioeconomic status, knee history of previous injuries or operations, present symptoms, level of daily activities and sports, hindrance and sick leave from daily activities, health-related quality of life and treatments received. Additionally, the 1-year and 6-year follow-up questionnaire collected data on experienced recovery or worsening of the knee symptoms (ie, outcome).
Functional disability and pain were assessed with the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)7 ,8 (assessed at baseline to 1-year follow-up), the Knee Injury Osteoarthritis Outcome Score (KOOS)9 (assessed at 6-year follow-up), the Medical Outcomes Study Short Form 36 Health Survey (SF-36),10 ,11 the Knee Society Score (KSS) function questions,12 the Lysholm Knee Scoring Scale,8 ,13 the Tampa Scale for Kinesophobia14 (only assessed at baseline) and the primary care cooperative information project/world organization of family doctors charts15 ,16 (only assessed at baseline to 1-year follow-up). The outcome measurement, experienced recovery of knee symptoms, was measured on a seven-point Likert scale. For all scores, except the Lysholm and SF-36, lower scores represent better function/outcome. GPs were asked to note the working diagnosis according to the International Classification of Primary Care (ICPC) in the patient's computerised medical file at first consultation.17
Statistical analysis
Descriptive statistics were used to describe patient characteristics, symptom characteristics, experienced recovery and working diagnosis of the GP. Univariable logistic regression analysis was used to determine which baseline variables from history taking (ie, patient characteristics and symptom characteristics) were associated with persistent knee symptoms at 1-year follow-up, expressed as ORs. The baseline variables chosen for the univariable analysis were based on the literature18 and clinical relevance. To enable easy interpretation of prognostic factors in a clinical setting, we chose to dichotomise most variables.
Imputation of missing data was carried out by multiple imputation, creating a total of five imputed databases.19–21 The variables showing an univariable association with persistent knee symptoms in at least three out of five imputed databases (p≤0.20) were analysed in a multivariable logistic regression model (backward LR method, entry 0.10, removal 0.15). If a variable was selected in at least three out of five imputed databases in the multivariable analysis, it was included in the final model (Enter method) and the area under the receiver operating curve (AUC) was calculated. First, separate models for patient characteristics and symptom characteristics were built. Subsequently, we combined the remaining variables of each domain to build a model of patient and symptom characteristics.
The outcome measurement self-reported perceived recovery was dichotomised into clinical recovery of knee symptoms (‘completely recovered’ and ‘much improved’) versus persistent knee symptoms (‘slightly improved’, ‘no change’, ‘slightly worsened’, ‘much worsened’ and ‘worse than ever’).
The analyses were performed using SPSS V.21.0 (SPSS Inc, Chicago, Illinois, USA).
Results
Study population
A total of 172 patients receiving a GP diagnosis of non-traumatic knee symptoms were included of whom 98 were diagnosed with ‘unspecified knee symptoms’ (ICPC L15) and 74 with patellofemoral pain syndrome (ICPC L99.07).
The mean age of the patients receiving a GP diagnosis of unspecified knee symptoms was 25.1 (SD 7.1) years, and 50.0% were men. In patients with unspecified knee symptoms, a total of 70 patients (71.4%) reported that the duration of their knee symptoms was less than 3 months at the time of consultation, 36 patients (36.7%) had bilateral knee symptoms, and 48 patients (49.0%) reported recurrent knee symptoms.
Regarding the patients receiving a GP diagnosis of patellofemoral pain syndrome, the mean age was 23.7 (SD 7.9) years, 52.7% were men; 38 patients (51.4%) reported that the duration of their knee symptoms was less than 3 months at the time of consultation, 42 patients (56.8%) had bilateral knee symptoms, and 42 patients (56.8%) reported having recurrent knee symptoms.
The patients available at 1-year and 6-year follow-up showed no significant differences compared with the total study population at baseline regarding age, gender, working diagnosis, knee symptoms, pain score (numerical rating scale (NRS)), Lysholm score and WOMAC index.
Also, the patients available at 6-year follow-up showed no significant difference compared with those available at 1-year follow-up regarding their perceived recovery at 1-year follow-up (OR=1.04, 95% CI 0.83 to 1.30). Reasons for no longer participating were: lack of time and/or lack of interest (n=32; 44%), unable to be contacted because of the changed address and/or telephone number (n=33; 45%), and for 8 patients (11%) no reason was available.
Course and prognosis
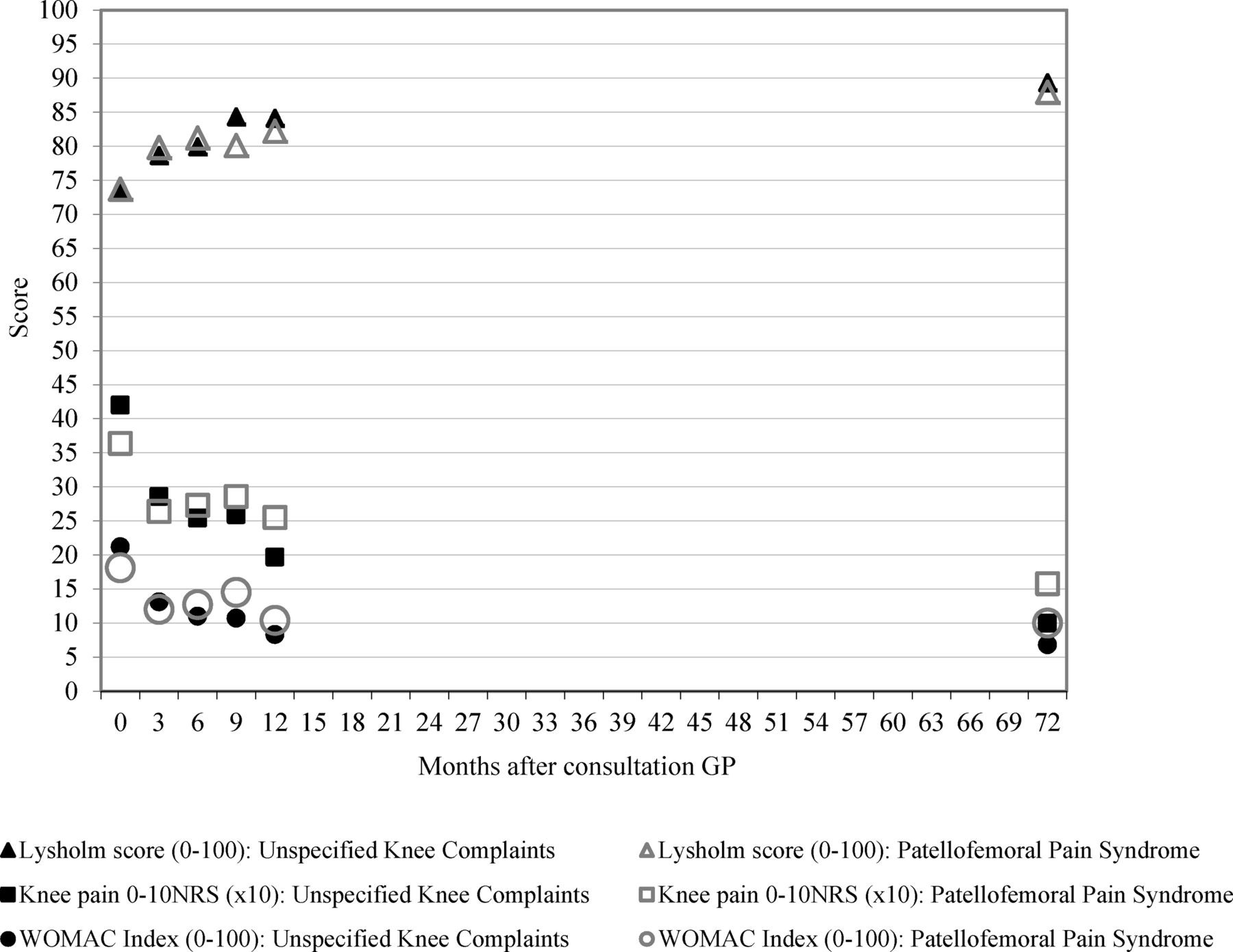
Figure 1 presents the 6-year course of the patients receiving a GP diagnosis of unspecified knee symptoms and the patients receiving a GP diagnosis of patellofemoral pain syndrome regarding mean knee pain severity (measured on an NRS), mean Lysholm knee score and mean WOMAC index. In both groups, the mean pain score, mean Lysholm knee score and mean WOMAC index showed the largest improvement in the first 3 months following consultation with the GP.
{kind=link}
Course of knee symptoms (mean scores) of the patients receiving a diagnosis of unspecified knee symptoms (n=98; closed markers) or patellofemoral pain syndrome (n=74; open markers). GP, general practitioner; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Table 1 shows the number of patients with persistent knee symptoms at 1-year and 6-year follow-up for the patients receiving a GP diagnosis of unspecified knee symptoms.
Characteristics of patients receiving a GP diagnosis of unspecified knee symptoms at baseline and at 1-year and 6-year follow-up
Of the 85 patients available at 1-year follow-up, 35 patients (41%) reported persistent knee symptoms. Their mean knee pain severity, measured with an NRS, was 3.6 (SD 2.2); their mean Lysholm knee score was 71.6 (SD 17.4) and their mean WOMAC index was 16.1 (SD 16.9). At 6-year follow-up, of the 54 patients, 10 (19%) reported persistent knee symptoms. Compared with baseline, four patients (40%) reported the same knee symptoms and one patient had another kind of symptom in the same knee.
The outcomes at 1-year and 6-year follow-up regarding the patients receiving a GP diagnosis of patellofemoral pain syndrome are presented in table 2.
Characteristics of patients receiving a GP diagnosis of patellofemoral pain syndrome at baseline and at 1-year and 6-year follow-up
Of the 65 patients available at 1-year follow-up, 37 (57%) reported persistent knee symptoms. Their mean knee pain severity, measured with an NRS, was 3.7 (SD 2.3); their mean Lysholm knee score was 75.3 (SD 15.4) and their mean WOMAC index was 16.2 (SD 15.4). At 6-year follow-up, of the remaining 44 patients, 18 (40%) reported persistent knee symptoms. Compared with baseline, the kind of knee symptoms had changed to another kind of symptom in the same knee in 3 patients (17%) and 14 patients (78%) reported the same knee symptoms.
Prognostic factors
Table 3 presents the univariable and multivariable associations between baseline characteristics and persistent knee symptoms at 1-year follow-up of the patients receiving a GP diagnosis of unspecified knee symptoms.
Univariable and multivariable association between baseline characteristics and persistent knee symptoms at 1-year follow-up of the patients receiving a GP diagnosis of unspecified knee symptoms
At 1-year follow-up, in the univariable analysis, the patient characteristics gender, body mass index (BMI) >25 and low/middle education level at baseline were associated with persistent knee symptoms. Of the symptom characteristics, having bilateral symptoms and self-reported absence of crepitus of the knee were associated with persistent knee symptoms at 1-year follow-up.
In the multivariate analysis patients’ characteristics, BMI >25 and low/middle education level showed an independent association with persistent knee symptoms at 1-year follow-up, with an AUC of 0.75. From the symptom characteristics, bilateral symptoms and self-reported absence of crepitus of the knee were independently associated with persistent knee symptoms, with an AUC of 0.64. Adding the symptom characteristics to the patient characteristics, the AUC increased to 0.80.
The univariable and multivariable associations between baseline characteristics and persistent knee symptoms at 1-year follow-up of the patients receiving a GP diagnosis of patellofemoral pain syndrome are presented in table 4.
Univariable and multivariable association between baseline characteristics and persistent knee symptoms at 1-year follow-up of the patients receiving a GP diagnosis of patellofemoral pain syndrome
At 1-year follow-up, in the univariable analysis, the patient characteristics BMI >25, low/middle education level at baseline, non-skeletal comorbidity, poor health and participating sports were associated with persistent patellofemoral symptoms. Of the symptom characteristics, having bilateral symptoms, self-report of a swollen knee and locking of the knee were associated with persistent patellofemoral symptoms at 1-year follow-up.
In the multivariate analysis patients’ characteristics, low/middle education level at baseline, non-skeletal comorbidity and reporting poor health showed an independent association with persistent knee symptoms at 1-year follow-up, with an AUC of 0.70. From the symptom characteristics, having bilateral symptoms, self-report of a swollen knee and locking of the knee were independently associated with persistent knee symptoms, with an AUC of 0.70. Adding the symptom characteristics to the patient characteristics, the AUC increased to 0.76.
Discussion
At 1-year follow-up, a surprisingly high percentage of 41% of patients receiving a GP diagnosis of unspecified knee symptoms reported persistent knee symptoms, and an even higher percentage of persistent knee symptom for patients receiving a GP diagnosis of patellofemoral pain syndrome (57%). At 6-year follow-up, 19% of the patients with unspecified knee symptoms at baseline and 40% of the patients with patellofemoral pain syndrome still reported persistent knee symptoms. In this study, the finding that patients receiving a GP diagnosis of patellofemoral pain syndrome had the worst prognosis is in accordance with the (few) reports available from secondary care.22–27
Regarding the patients receiving a GP diagnosis of unspecified knee symptoms at baseline, prognostic factors associated with persistent knee symptoms at 1-year follow-up were BMI >25, low/middle education level, bilateral symptoms and self-reported absence of crepitus of the knee. Regarding the patients receiving a GP diagnosis of patellofemoral pain syndrome at baseline, associated with persistent knee symptoms at 1-year follow-up were low/middle education level, poor health, having bilateral symptoms and self-report of a swollen knee. Findings from a physical examination were not included in the analyses and could reveal other risk factors for persistent knee symptoms.28
Our study is the first to report on prognostic factors in adolescents and young adults with non-traumatic knee symptoms in general practice.
Most of the prognostic factors revealed in this study (especially the patient and symptom characteristics) are also reported in other studies on prognostic factors in adults with knee pain,29–32 in patients with other musculoskeletal disorders18 ,33 or in patients with patellofemoral pain syndrome.24 ,34
Limitations
One limitation of this study is that a relatively large percentage was lost to follow-up, especially at 6-year follow-up (42%). For example, some people changed addresses and some lost interest in the study. However, the patients available at 1-year and 6-year follow-up showed no major differences in characteristics observed at baseline.
We decided to perform univariable regression analysis with a relatively large p value of 0.20 to determine which factors to test in multivariable analysis; this was due to the difficulty in choosing possible prognostic factors in view of the lack of research in this field. Consequently, in a relative small patient sample, we tested a large number of prognostic factors in the univariable analysis. Therefore, it is important that our findings should be replicated in other larger patient samples and that for now the results should be interpreted with caution. Also, in this study, there is a lack of information on treatment during the follow-up period which could have influenced the outcome. However, the number of patients receiving surgery was low (n=7) at 6-year follow-up.
Implications for clinical practice and future research
For adolescents and young adults with non-traumatic knee symptoms, GPs should consider those with patellofemoral pain syndrome as a separate group, because their prognosis is worse than that for the unspecified knee symptoms.1 In particular, we need to elucidate the mechanisms behind patellofemoral pain syndrome.35–38
Conclusions
The prognosis of non-traumatic knee symptoms in adolescents and young adults in general practice is not good. Various baseline prognostic factors seem to be associated with persistent knee symptoms at 1-year follow-up but should be replicated in another larger study.
The prognosis of patients receiving a GP diagnosis of patellofemoral pain syndrome seemed worse than that for patients receiving a GP diagnosis of unspecified knee symptoms, with 40% of the former reporting persistent symptoms at 6-year follow-up.
What are the new findings?
-
The prognosis for patients who present in general practice with non-traumatic knee symptoms in adolescents and young adults is not as good as was previously assumed.
How might it impact on clinical practice in the near future?
-
General practitioners should consider patients with patellofemoral pain syndrome as a separate group, because their prognosis is worse than that of patients with unspecified knee symptoms.
-
Clinicians should remain alert to discoveries relating to the mechanisms behind patellofemoral pain syndrome (fast knowledge translation).
References
Footnotes
-
Contributors JANV, BWK and SMAB-Z contributed substantially to the conception and design of the study. MK and EMH were involved in the acquisition of data. MK, PAJL, MvM and SMAB-Z were involved in the analysis and interpretation of data and in drafting the manuscript. All authors revised the draft manuscript critically and have read and approved the final manuscript.
-
Funding The research network Honeur was financially supported by the health insurance companies TRIAS, Zilveren Kruis Achmea and OZ, and partly funded by a programme grant of the Dutch Arthritis Foundation.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics Committee Erasmus MC, Rotterdam, Netherlands.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The data are anonymised and the risk of identification is low. Data from the trial may be available from the corresponding author at p.luijsterburg@erasmusmc.nl subject to agreement about the use of the data.