Article Text

Abstract
Objective To determine whether brief interventions promoting physical activity are cost-effective in primary care or community settings.
Design Systematic review of economic evaluations.
Methods and data sources We searched MEDLINE, EMBASE, PsycINFO, CINAHL, EconLit, SPORTDiscus, PEDro, the Cochrane library, National Health Service Economic Evaluation Database and the Cost-Effectiveness Analysis Registry up to 20 August 2014. Web of Knowledge was used for cross-reference search. We included studies investigating the cost-effectiveness of brief interventions, as defined by National Institute for Health and Care Excellence, promoting physical activity in primary care or the community. Methodological quality was assessed using Drummond's checklist for economic evaluations. Data were extracted from individual studies fulfilling selection criteria using a standardised pro forma. Comparisons of cost-effectiveness and cost-utility ratios were made between studies.
Results Of 1840 identified publications, 13 studies fulfilled the inclusion criteria describing 14 brief interventions. Studies varied widely in the methods used, such as the perspective of economic analysis, intervention effects and outcome measures. The incremental cost of moving an inactive person to an active state, estimated for eight studies, ranged from £96 to £986. The cost-utility was estimated in nine studies compared with usual care and varied from £57 to £14 002 per quality-adjusted life year; dominant to £6500 per disability-adjusted life year; and £15 873 per life years gained.
Conclusions Brief interventions promoting physical activity in primary care and the community are likely to be inexpensive compared with usual care. Given the commonly accepted thresholds, they appear to be cost-effective on the whole, although there is notable variation between studies.
- Physical activity
- Economics
- Review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Physical inactivity leads to an increased risk of developing over 20 health conditions, including coronary heart disease (CHD), cancer, type 2 diabetes and stroke.1 ,2 In developed countries, these diseases and conditions attributable to physical inactivity account for 1.5–3% of total direct healthcare costs.3 In 2006–2007, the direct costs to the UK National Health Service (NHS) from treating the consequences of physical inactivity were estimated to be £0.9 billion.4 Physical activity not only improves physical health but also contributes to mental well-being.5 Incorporation of physical activity into individual lifestyles is known to lead to health benefits such as reduced risk of CHD, stroke and type 2 diabetes and the risk of premature death.6 ,7
In recent years, there has been substantial emphasis on efforts to promote physical activity along the continuum of individual-level and population-based interventions.8 The UK's Chief Medical Officers recommend that adults undertake at least 150 min of moderate-intensity activity each week.9 Despite the well-reported health and economic benefits of physical activity, results from the 2008 Health Survey for England, using self-reported measures, showed that only 39% of men and 29% of women achieved the recommended levels,10 a situation that had not improved by the time of the 2012 survey.11
This led to a substantial policy interest to raise the overall physical activity in the general population.12 A wide range of interventions increase physical activity across the life course.13 ,14 The National Institute for Health and Care Excellence (NICE) has published multiple pieces of guidance on physical activity promotion. In 2006, NICE published a guideline on four commonly used methods to increase physical activity (brief interventions in primary care, exercise referral schemes, pedometers and community-based exercise programmes for walking and cycling)15 supported by an economic analysis.16 More recently, NICE produced specific guidance on approaches to increase walking and cycling,17 and updated guidance on brief advice for adults in primary care18 and exercise referral schemes.19
There is an enthusiasm within government at national and local levels to support a wide variety of initiatives to promote physical activity, and reap the health, social and economic benefits.12 In times of particular budgetary restraint, there is an obvious need to look for low-cost initiatives. Brief interventions may be such a solution as they require less resources compared with more intensive interventions. Although they may have a small effect on an individual's behaviour, if sustained they could potentially have a significant population health impact.16
Current intervention strategies based in primary care or the community have provided the evidence that they can effectively increase physical activity.20–22 Moreover, recent systematic reviews and meta-analyses of randomised and non-randomised trials have shown that physical activity interventions such as brief advice, exercise on prescription and physician counselling significantly increase physical activity behaviour and fitness in the longer term.23 ,24
Although brief interventions are effective in promoting physical activity, for policymakers and health funders it is necessary to know whether they are cost-effective to set priorities and allocate finite public funds. Previous reviews of economic evaluations of physical activity interventions suggest that most of the current intervention strategies are cost-effective.25–28 However, these reviews evaluated the cost-effectiveness of physical activity in general, included intensive interventions such as supervised exercise sessions, workplace interventions and only covered the literature to 2010. In addition, the lack of economic evidence for brief interventions in physical activity has been recognised.29 ,30 Thus, we tailored our search to a specific question, that is, ‘What do we currently know about the cost-effectiveness of brief interventions delivered in primary care or community settings to increase physical activity?’
Methods
Definitions
For the purpose of this review, we used the NICE definition of brief interventions:15 “Brief interventions involve opportunistic advice, discussion, negotiation or encouragement. They are commonly used in many areas of health promotion, and are delivered by a range of primary and community care professionals. The interventions vary from basic advice to more extended, individually-focused attempts to identify and change factors that influence activity levels”. Brief interventions are typically conducted in face-to-face sessions with or without the addition of written materials, ranging from a single session of short duration (5–30 min) to multiple brief sessions or follow-ups.31
Data sources
We searched for articles published up to 20 August 2014 using the electronic databases MEDLINE, EMBASE, PsycINFO, CINAHL, EconLit, SPORTDiscus, Physiotherapy Evidence Database (PEDro), the Cochrane library, the NHS Economic Evaluation Database and the Tufts Cost-Effectiveness Analysis (CEA) Registry. In addition, the references of retrieved articles were examined manually after reviewing the title and abstracts to identify any economic studies alongside clinical trials and other pertinent studies. A cross-reference search was done using Web of Knowledge, and free text searching was performed using Google scholar. The search consisted of keywords and MeSH terms related to physical activity, exercise or fitness, brief or minimal intervention, and economic or cost analysis and was limited to the English language. Details of the search strategy used are described in online supplementary appendix 1.
Study selection
Studies were eligible for inclusion if they met the following three criteria:
Type of study—economic analyses alongside randomised controlled trials (RCTs) or non-experimental designs, or modelling studies of physical activity interventions which were based in either primary care or the community. Comparators could include usual care or other interventions.
Type of intervention—(a) interventions involving verbal advice, encouragement, negotiation or discussion, delivered face-to-face in a single session or multiple brief sessions, with or without additional non-face-to-face contacts (eg, leaflets or phone calls) or (b) interventions that were reported as ‘brief’ or ‘minimal’, and aimed to increase physical activity or fitness levels (or both) at the individual level (ie, brief interventions delivered to individuals or groups). Interventions were included if they were either the primary focus of the study or one of the comparator interventions, because physical activity interventions are often used in conjunction with or compared to other types of interventions (such as combined physical activity and dietary advice) for their physical well-being benefits.
Study populations—inactive adults aged 16 years or over. We excluded interventions where study populations were targeted or selected on the basis of pre-existing disease conditions (eg, osteoarthritis) because these populations require specialised interventions.
Data extraction and analysis
Initial screening of titles and abstracts against inclusion criteria was undertaken by one researcher (VGC) and potentially relevant articles were retrieved. Abstracted data were double checked by a second researcher (EW) and, if necessary, amendments were made after discussion. If there was insufficient information in the article on cost-effectiveness, we contacted the corresponding author. Included studies were assessed for methodological quality using Drummond's checklist32 for assessing economic evaluations. The checklist considers the following aspects: study question, selection of alternatives, form of economic evaluation, data collection (effectiveness data), benefit measurement and valuation, costing, modelling, allowance for uncertainty and presentation of results (table 1). On the basis of the number of Drummond's checklist criteria met, a rating of ‘high’ (9–10), ‘good’ (7–8), ‘fair’ (5–6) or ‘poor’ (1–4) was assigned.
Critical appraisal of included economic papers using Drummond et al's32 checklist
We used a standardised pro forma to extract data from full texts on the type of economic analysis and perspective, interventions and comparison, participants, follow-up duration, outcome and cost-effectiveness results. To compare the economic results of the individual studies, we converted all costs to 2011 pounds sterling (£) by applying the gross domestic product deflator index (GDP values) and purchasing power parities conversion rates using the Campbell & Cochrane Economics Methods Group (CCEMG)-Evidence for Policy and Practice Information and Coordinating Centre (EPPI-Centre) Cost Converter (V1.4).33 ,34 Cost-effectiveness results were grouped into those reporting intermediate outcomes such as the incremental cost of moving one inactive adult to an active category (ie, meeting the physical activity recommendations)9 and those reporting final outcomes such as the incremental cost per incremental quality-adjusted life year (QALY) gained, disability-adjusted life year (DALY) averted or life years gained (LYG).
Results
Literature search
The search identified 1840 potentially relevant articles. An additional four articles were identified through reference lists and grey literature search. Following the removal of duplicates and the review of titles and abstracts, we assessed the full text of 28 articles. Thirteen met the inclusion criteria and were included in the review (figure 1). Five studies originated from the UK (one of them in Scotland),35–39 four from New Zealand,40–43 two from Australia,44 ,45 and one each from Sweden46 and the Netherlands.47

PRISMA flow diagram of study selection.
Of the 15 excluded studies, six reported more intensive interventions and/or did not include a face-to-face component (eg, supervised exercise sessions, mail or telephone contact);48–53 four included a combined intervention targeting multiple behaviours (eg, physical activity and diet);54–57 two were exercise referral schemes (referral to a physical activity specialist or service);58 ,59 two did not report a physical activity or cost-effectiveness outcome60 ,61 and one study evaluated the cost-effectiveness of a subsidy programme for general practitioner (GP) involvement in physical activity.62
Characteristics of included studies
Across the 13 studies, 30 intervention strategies or scenarios were evaluated, of which 14 met the definition of brief interventions. These were grouped into: brief exercise advice, exercise on prescription, pedometers and motivational interventions (table 2).
Overview of interventions
Four studies performed economic evaluation alongside controlled trials,39 ,41–43 and two were based on quasi-experimental designs.36 ,38 Seven studies performed economic modelling using data from a single trial,40 ,44 ,46 a meta-analysis of RCTs,37 ,44 ,47 a systematic review of randomised and observation studies,35 or a cross-sectional and observational study.45 Four studies reported intermediate outcomes in terms of the cost of making one additional inactive person active;36 ,39 ,41 ,42 five reported final outcomes in terms of incremental cost per DALY44 or QALY40 ,47 or LYG46 or incremental net health benefit (NHB)37 and four reported both intermediate and cost-utility outcomes.35 ,38 ,43 ,45
The 13 studies that met the inclusion criteria are described in table 3. The follow-up of RCTs ranged from 12 months to 2 years. One study had a short follow-up (3 months).36 Nine studies were of good or high quality. Modelling studies adopted a lifetime horizon. The measurement of physical activity was different across studies. The studies reporting a time-based outcome used a target of ≥5×30 min/week of moderate or ≥60 min/week of vigorous-intensity activity. In pedometer-based interventions, a common threshold measure used was ≥10 000 steps/day except for one study39 which used a target of a weekly increase of ≥15 000 steps. Six studies36 ,39–42 ,45 reported the duration of brief interventions (face-to-face), which lasted from 4 to 30 min. Most (10) of the included studies evaluated each intervention in comparison with usual care or current practice, which approximates a ‘do nothing’ scenario.
Characteristics of included studies
Studies reporting intermediate outcomes
The cost of converting one inactive adult to an ‘active’ category was estimated for eight studies and ranged from £96 to £986 (figure 2). An ‘active script programme’ (an organised approach to exercise counselling by GPs) evaluated by Sims et al45 appeared to be the most cost-effective of the interventions considered (£96 per additional active participant compared with usual care). Boehler et al36 evaluated the cost-effectiveness of two recruitment strategies for the delivery of brief exercise advice (disease register screening vs opportunistic patient recruitment). They reported the incremental cost of converting one inactive adult to an active state as £986 in disease register screening compared to opportunistic screening. Elley et al41 reported the cost-effectiveness of ‘enhanced green prescription’ (nurse delivered exercise counselling and written prescription with telephone follow-up) at both 12 and 24 months postintervention, which showed decreasing cost-effectiveness over time of follow-up (£308 at 12 months vs £630 at 24 months).
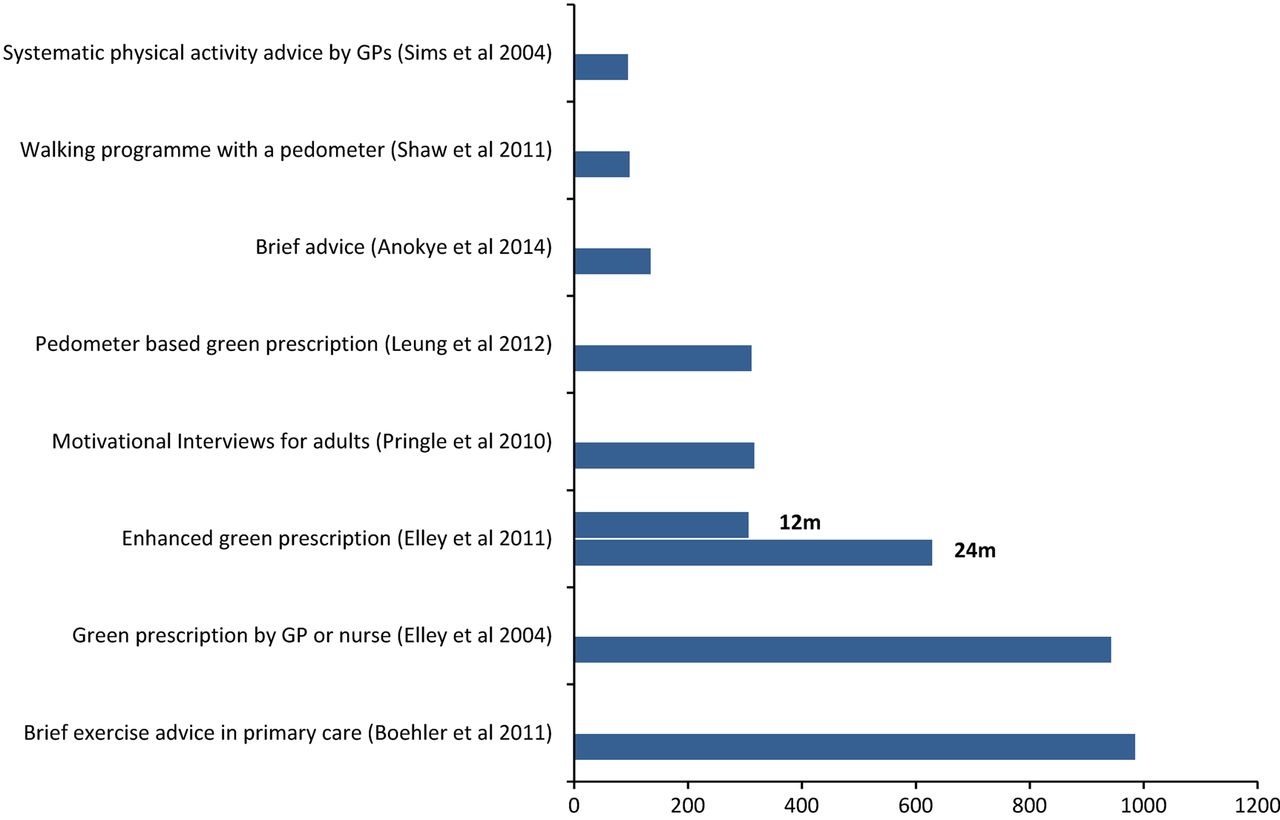
Incremental cost of converting one sedentary adult to an active category (2011 equivalent £ sterling; GP, general practitioner).
Studies reporting final outcomes
Figure 3 summarises the results in terms of incremental cost utility, that is, per QALY or DALY or LYG. Pedometer-based brief interventions appeared likely to yield health gains at a lower cost. Pedometers (either as a motivational tool or in combination with exercise advice) were dominant as they were both cost saving and more effective when compared with usual care44 or standard ‘green prescription’ (oral or written exercise advice by a GP or practice nurse with telephone follow-up).43 GP counselling in combination with a pedometer when compared with current practice had a cost-utility of £8858/QALY.47

Cost-effectiveness ratios (cost per DALY or QALY or LYG) for different physical activity interventions (2011 equivalent £ sterling; DALY, disability-adjusted life year; GP, general practitioner; LYG, life years gained; QALY, quality-adjusted life year).
Pringle et al38 evaluated the costs and cost-effectiveness of seven broad categories of community-based interventions. Among these, only motivational interviews are relevant to the scope of this review. The analysis was conducted alongside a pre-intervention and post-intervention design and hence no ‘usual care’ or ‘do nothing’ control group was considered. Cobiac et al44 compared six intervention strategies, each against ‘do nothing’, of which pedometers and exercise on prescription are relevant to this review. They reported that the use of pedometers was more cost-effective than other interventions. Likewise, Lindgren et al46 modelled the cost utility of three interventions of dietary and exercise advice of which exercise advice by a physician was relevant to this review. The estimated cost utility of exercise advice by a physician was £15 873/LYG when compared with usual care.
The incremental cost-effectiveness ratio (ICER) for exercise advice or exercise on prescription (vs usual care) ranged from £1104 to £14 002/QALY,35 ,37 ,40 and from £2542 to £6500/DALY.44 ,45 Motivational interviews had the lowest ICER (£57/QALY).38 In a primary care setting, GP counselling in combination with a pedometer47 had a lower cost-effectiveness ratio than a GP's advice or counselling with written materials37 (£8858 vs £14 002/QALY); both were compared with usual care.
These economic modelling studies used either a multistate life-table modelling approach44 or Markov chain35 ,37 ,46 ,47 or a decision tree.38 Effectiveness data used in these modelling studies had a follow-up duration of up to 2 years.
Discussion
The studies identified in this review suggest that brief interventions can result in a meaningful increase in physical activity at reasonable costs. When the longer term costs and health benefits are considered, brief interventions are cost-effective compared with the NICE threshold of £20 000–£30 000/QALY gained.
Successful interventions—‘bright spots’
Exercise advice,35 ,45 pedometer-based walking,39 pedometer-based ‘green prescription’43 and motivational interviews38 had similar cost-effectiveness ratios for converting one inactive person to an active state. The ‘active script programme’ evaluated by Sims et al45 had the lowest cost-effectiveness in terms of cost per additional active person. However, their economic model had rather optimistic assumptions regarding the uptake of physical activity by intervention and control group patients, and the time horizon of the study was not clear. From the reviewed studies, we observed that in the absence of continued contacts, some of the gains in physical activity experienced by participants are likely to be lost over time, resulting in the intervention becoming less cost-effective over a longer time horizon, as was evident in the analysis of ‘enhanced green prescription’.41
Promoting pedometer use,44 pedometer in combination with exercise on prescription,43 motivational interviews,38 GP advice or counselling on exercise40 ,45 and brief advice35 were the most cost-effective intervention strategies with respect to cost utility. Both Leung et al43 and Cobiac et al44 found the cost-effectiveness of their pedometer intervention to be dominant, indicating that the pedometer intervention is more effective and less costly than comparators. However, note that Leung et al43 compared pedometer-based ‘green prescription’ with standard ‘green prescription’ rather than with usual care. In contrast, Over et al47 reported a considerably higher ICER for pedometer intervention compared to current practice (£8858/QALY). Although the effectiveness data for both the Cobiac et al44 and Over et al47 studies were based on a meta-analysis by Bravata et al,63 the higher possible health gains in Cobiac et al44 may be a consequence of the much larger proportion of inactive people in the Australian population compared to the Dutch population, and of the reported programme cost per participant being lower in the Australian estimates than in the Over et al studies.47
Anokye et al35 modelled the cost-effectiveness of brief advice in primary care using meta-analysed data, but the underlying primary evidence included both RCTs and non-randomised studies. A primary care nurse delivered ‘enhanced green prescription’41 had a more favourable ICER than a GP delivered ‘green prescription’42 (£308 vs £938 for converting one additional inactive adult to an active state over a 12-month period). The ‘enhanced green prescription’ had a slightly higher proportion of people who increased their activity at 12 months than just ‘green prescription’, which was most likely attributable to the extra telephone support and 6-month face-to-face, nurse-led follow-up. Three studies40 ,42 ,44 evaluated the cost-effectiveness of ‘green prescription’ using data from a cluster RCT.20 However, they reported different cost outcomes—cost per DALY,44 QALY40 or the intermediate outcome.42
Some of the modelling studies adopted previously reported economic models. For example, Pringle et al's38 model was informed by the NICE cost-effectiveness model,16 while Over et al47 used the Dutch National Institute for Public Health and the Environment (RIVM) Chronic Disease Model to estimate the long-term effects of increase in physical activity. The particular disease states included in a model affect the long-term estimates of cost and health outcome. Lindgren et al46 included only CHD conditions in their model while others included multiple conditions (type 2 diabetes, CHD, breast and colorectal cancers and depression).
Methodological issues to take into account
Some of the studies failed to report sources for unit costs, and some potentially relevant costs were being excluded from the analysis. For example, Dalziel et al40 included only programme costs, but excluded the healthcare cost implications of downstream health events. Similarly, Pringle et al38 did not include out-of-pocket expenditures which might be significant and could influence the intervention attendance levels (apart from the cost-effectiveness of the intervention).
The model-based economic evaluations of brief interventions differ mainly in terms of the quality of evidence used, structure and outcome measure. Use of data on the effect of interventions in economic modelling using a systematic review and meta-analysis of RCTs is proposed as the least biased source of data.64 LYG is a pure measurement of life expectancy whereas DALYs and QALYs adjust life expectancy for morbidity, using disability and quality-of-life weighting, respectively.65 ,66 The ICERs for both QALY and DALY outcomes varied between studies—primary care-based exercise advice evaluated by Dalziel et al40 had a lower cost utility (£1104/QALY) than Gulliford et al's37 study (£14 002/QALY). Gulliford et al37 used effectiveness data from a recent systematic review and meta-analysis of RCTs23 and evaluated two scenarios of universal strategy to promote physical activity. Their model was more comprehensive than Dalziel et al's40 model in terms of inclusion of disease conditions (16 single disease or multi-disease states), model structure and intervention effects.
Sensitivity analysis
Eight studies included in this review35–37 ,40 ,43 ,44 ,46 ,47 properly characterised decision uncertainty by using probabilistic sensitivity analysis while the remaining studies used scenario-based or one-way sensitivity analysis. Four studies39 ,41–43 were based on ‘piggybacked’ economic evaluations conducted alongside rigorous RCTs. These provide a source of evidence on resource use and health effects from well-designed studies with high internal validity. However, they are often constrained in terms of the range of outcome data collected or the length of follow-up, introducing difficulties in extrapolating the intervention effectiveness beyond the trial period.67 For example, the assumptions around the maintenance of physical activity levels beyond brief interventions determine how cost-effective the intervention is. In addition, it should be recognised that economic analysis in three studies36 ,38 ,45 was based on evidence from non-experimental studies or theoretical scenarios.
Comparison with previous reviews
Three previous economic reviews of physical activity interventions were identified. A recent systematic review commissioned by NICE29 reported that brief advice in primary care was cost-effective (when usual care was used as the benchmark). However, the evidence was limited to three studies. Garrett et al28 reviewed the cost-effectiveness of physical activity interventions in primary care and the community, and included 13 RCTs. The review also included intensive interventions but did not include modelling studies. They reported that most interventions were cost-effective, especially where direct supervision or instruction was not required. The cost-effectiveness ratios for moving one inactive person to an active stage at 12 months varied from £262 to £3144, and the cost-utility estimated in nine studies varied from £276 to £68 798/QALY gained (2011 prices). Another review by Muller-Riemenschneide et al25 included eight studies (6 RCTs, 1 cross-sectional and 1 economic modelling) covering a broad range of interventions promoting physical activity. The review concluded that behavioural interventions targeting sedentary healthy adults can achieve the recommended level of physical activity at a cost of £662 per participant over a 12-month period (2011 prices). However, their review included workplace-based physical activity and environmental interventions.
These reviews either considered the cost-effectiveness of physical activity interventions in general and were not specific to brief interventions25 ,28 or did not include other kinds of brief interventions for physical activity (eg, pedometer-based interventions).29 Although six studies included in our review were also included in the previous reviews (figure 4), we include seven additional studies and looked specifically at the cost-effectiveness of brief interventions promoting physical activity in the general population.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Venn diagram showing overlap of studies with previous reviews.
Strengths and limitations of the review
To the best of our knowledge, this is the most comprehensive economic review to date of brief interventions for physical activity. We assessed the efficiency of brief interventions in terms of cost-effectiveness ratios, and report both intermediate (ie, incremental cost of converting one inactive adult to an active category) and final outcomes (cost per DALY or QALY or LYG). The current review includes both economic evaluations alongside RCTs and economic modelling, summarising the results of economic evaluation studies of brief interventions in primary care and community settings.
In general, the assessment of the cost-effectiveness of different brief interventions was challenging. They vary widely in terms of the methodology used in their cost-effectiveness or cost-utility analyses, including the perspective of the economic analysis, and the discounting of future values of cost and health outcomes. The reviewed modelling studies have their own limitations: the assumptions underlying the models can differ considerably, for instance, as regards the assumptions on the proportion of people becoming active as a result of the brief intervention, outcome measures and on the decay in intervention effect over time. Such methodological differences between the studies as well as other context characteristics (eg, the variability in funding mechanism, health system and cost structures) limit the generalisability of the cost-effectiveness results across different settings.68 In addition, some of the studies included in this analysis lack intervention details, for example, time duration and/or delivery method (eg, type of provider and individual vs group delivery), making it difficult to determine whether or not the interventions were truly ‘brief interventions’ according to the NICE definition. It is important to describe interventions in sufficient detail,69 such as the duration of ‘brief interventions’, as it affects cost-effectiveness. In this review, we included brief physical activity interventions that had at least one (initial) face-to-face contact and acknowledge that there is a need for economic reviews of non-face-to-face physical activity interventions which constitute a fast growing research area.
It would be more appropriate to compare each intervention in an iterative manner taking an account of dominance and extended dominance to determine the most cost-effective intervention.70 The interventions included in this review were typically compared with a usual care (do nothing) intervention that compromises the ability to rank interventions. What is required in order to make this comparison is a single framework (ie, decision analytic model) to transform the short-term costs and intermediate (‘disease specific’) outcomes into longer term final outcomes (namely QALYs), in order both to identify the most cost-effective intervention strategy and to quantify the associated decision uncertainty.
Summary
Brief interventions delivered at the individual level by a GP, practice nurse or other healthcare professional can increase physical activity in healthy inactive adults at a reasonable cost to convert one inactive adult to being ‘active’. Our findings suggest that it is possible to deliver a brief intervention for less than £15 000/QALY gained. On the basis of the cost-utility analysis, the use of pedometers and motivational interviews had the lowest cost-effectiveness ratio. Heterogeneity in interventions, study participants and study design compromises the comparability of the results across studies. It is thus difficult to rank and prioritise intervention strategies based on cost-effectiveness ratios, though most of these interventions are considered cost-effective when measured against the current NICE threshold of £20 000–£30 000/QALY.71
We conclude that brief interventions are likely to be inexpensive, but we have limited knowledge on the longer term costs and consequences of these interventions.30 Thus, economic modelling from studies with a longer follow-up will improve estimates of the longer term costs and consequences of brief interventions for physical activity in primary care or community settings.
What is already known on this topic
Brief interventions for physical activity in primary care or community settings are considered to be effective in increasing individuals’ physical activity. However, the evidence on the cost-effectiveness of such interventions is sparse.
What this study adds
Some brief interventions increase individuals’ physical activity at reasonable costs and are cost-effective, given commonly accepted thresholds. An economic evaluation of brief interventions with a longer follow-up will improve the estimates of the longer term costs and benefits of physical activity.
Acknowledgments
The authors would like to thank Dr Dan Mason and Ms Laura Lamming for their comments on the initial version of this manuscript, and the author(s) of studies included in our review who responded to requests for clarification or further information about study data. This study was conducted on behalf of the Very Brief Interventions Programme team (see http://www.phpc.cam.ac.uk/pcu/research/research-projects-list/vbi/vbi-research-team for team members).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Twitter Follow Ed Wilson at @edcfwilson
Contributors EW and VGC contributed to the design of the review. VGC executed the search strategy with inputs from EW and MS, reviewed the references found, assessed studies for inclusion, appraised and extracted the data from each of the included studies, and also performed the analysis and prepared the first draft. EW double checked the extracted data for the included studies. EW, MS, SS and WH provided critical comments on quality assessment and data analysis. All authors contributed to the critical revision of the manuscript and approved the final version of the manuscript.
Funding EW is funded by the NIHR Cambridge Biomedical Research Centre. This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research Programme (Grant Reference Number RP-PG-0608-10079). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. The funder had no role in study design, data collection, data analysis, data interpretation, the writing of the manuscript, and decision to submit the manuscript for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.