Article Text

Abstract
Background/aim This randomised controlled trial investigated if the usage of running shoes with a motion control system modifies injury risk in regular leisure-time runners compared to standard shoes, and if this influence depends on foot morphology.
Methods Recreational runners (n=372) were given either the motion control or the standard version of a regular running shoe model and were followed up for 6 months regarding running activity and injury. Foot morphology was analysed using the Foot Posture Index method. Cox regression analyses were used to compare injury risk between the two groups, based on HRs and their 95% CIs, controlling for potential confounders. Stratified analyses were conducted to evaluate the effect of motion control system in runners with supinated, neutral and pronated feet.
Results The overall injury risk was lower among the participants who had received motion control shoes (HR=0.55; 95% CI 0.36 to 0.85) compared to those receiving standard shoes. This positive effect was only observed in the stratum of runners with pronated feet (n=94; HR=0.34; 95% CI 0.13 to 0.84); there was no difference in runners with neutral (n=218; HR=0.78; 95% CI 0.44 to 1.37) or supinated feet (n=60; HR=0.59; 95% CI 0.20 to 1.73). Runners with pronated feet using standard shoes had a higher injury risk compared to those with neutral feet (HR=1.80; 95% CI 1.01 to 3.22).
Conclusions The overall injury risk was lower in participants who had received motion control shoes. Based on secondary analysis, those with pronated feet may benefit most from this shoe type.
- Foot
- Injury
- Running shoes
- Sporting injuries
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Several hundred running shoe models are currently available in the market. Notwithstanding the increasing focus on running shoe design, technologies and function, running-related injury incidence has not changed noticeably over the last few decades.1 Various biomechanical variables such as strike pattern,2 impact forces,3 foot posture or foot pronation,4 ,5 have all been proposed as injury risk factors. Footwear features such as cushioning technology, stability and motion control systems (motion control shoes), have been designed to mitigate against these risk factors and are extensively used as selling points by shoe manufacturers.
Foot posture is believed by some to be a risk factor for injury.5 This often results in attempts to match footwear to a runner's foot morphology, despite an absence of evidence to suggest this approach will reduce injuries.4–6 Specifically, motion control shoes are typically prescribed to runners with pronated feet, while neutral stability shoes are recommended to individuals with neutral feet and cushioned shoes to those with supinated feet. Several studies have been unable to demonstrate the benefit of the above-described prescription strategy,7–10 although they were either inadequately powered,9 or performed in a military population,7 ,8 limiting the applicability of findings to distance runners.4 Furthermore, a more pronated foot posture was reported not to be associated with injury risk in a prospective cohort study on over 900 novice runners,11 questioning the use of running shoes featuring motion control systems designed to reduce foot pronation. Running in shoes equipped with that technology increased the risk of experiencing running-related pain.9 Although these results are preliminary, it is worrying that a significant proportion of running shoes have motion control, a fact that many runners may not be aware of when buying their shoes.
Therefore, in this study, we (1) investigated whether running shoes equipped with motion control features modified injury risk in regular leisure-time runners and (2) if this influence depended on foot morphology. Our main hypothesis was that injury risk would be different when running in shoes with motion control compared with standard (neutral) shoes, while controlling for the potential confounders. Our secondary hypothesis was that the difference in injury risk would depend on foot morphology.
Materials and methods
Participants and study design
This randomised controlled trial (unregistered) recruited recreational runners, regardless of fitness level. Reporting of the study followed the CONSORT statement.12 Given an expected injury rate of 22% and 35% in the two groups,9 respectively, and a desired power of 0.8 and an α-level of 0.05, a total of 364 runners were required to test our main hypothesis. All participants received a full description of the study protocol and provided written informed consent for participation. All procedures were approved by the National Ethics Committee for Research (ref 201211/04). Participants were recruited via advertisements in local newspapers and on specialised internet sites from March to April 2014. Following online registration, participants were contacted by phone to verify inclusion criteria: healthy, aged 18–65 years, regular running (at least 1 session/week) for at least 6 months over the 12 months prior to the study, no contraindication to perform running activity, no prior (<12 months) surgery at the lower limbs or lower back region, and no use of orthopaedic insoles for running activities. Volunteers were also required to perform at least one running activity per week during the 6-month follow-up period (from June to December), to use the provided study shoes for all running activities, and to report, at least once per week, all sports activities and injury or pain experienced during the follow-up.
Individuals reported to the laboratory for eligibility check and baseline assessment. A questionnaire gathered information about age, sex, running regularity over the previous 12 months (months of practice), running experience (years of regular practice) and previous injury to the lower back or lower limbs preventing normal running activity during the preceding 12 months. Foot posture was assessed using the six-item Foot Posture Index (FPI), previously proven to be valid.13 ,14 Normative values presented by Redmond et al15 were used as references to categorise each foot into one of the five categories (highly supinated, supinated, neutral, pronated and highly pronated) based on their FPI score. Two previously trained appraisers performed all evaluations and assessed the first 50 participants together to optimise consistency. Subsequently, high inter-rater agreement for classifying the runners in one of the five categories was found based on a further 40 participants, with a Cohen's κ coefficient of 0.86. Since the unit of analysis is the participant, the classification into one of the five categories was based on the foot with the most extreme score.
Study shoes characteristics
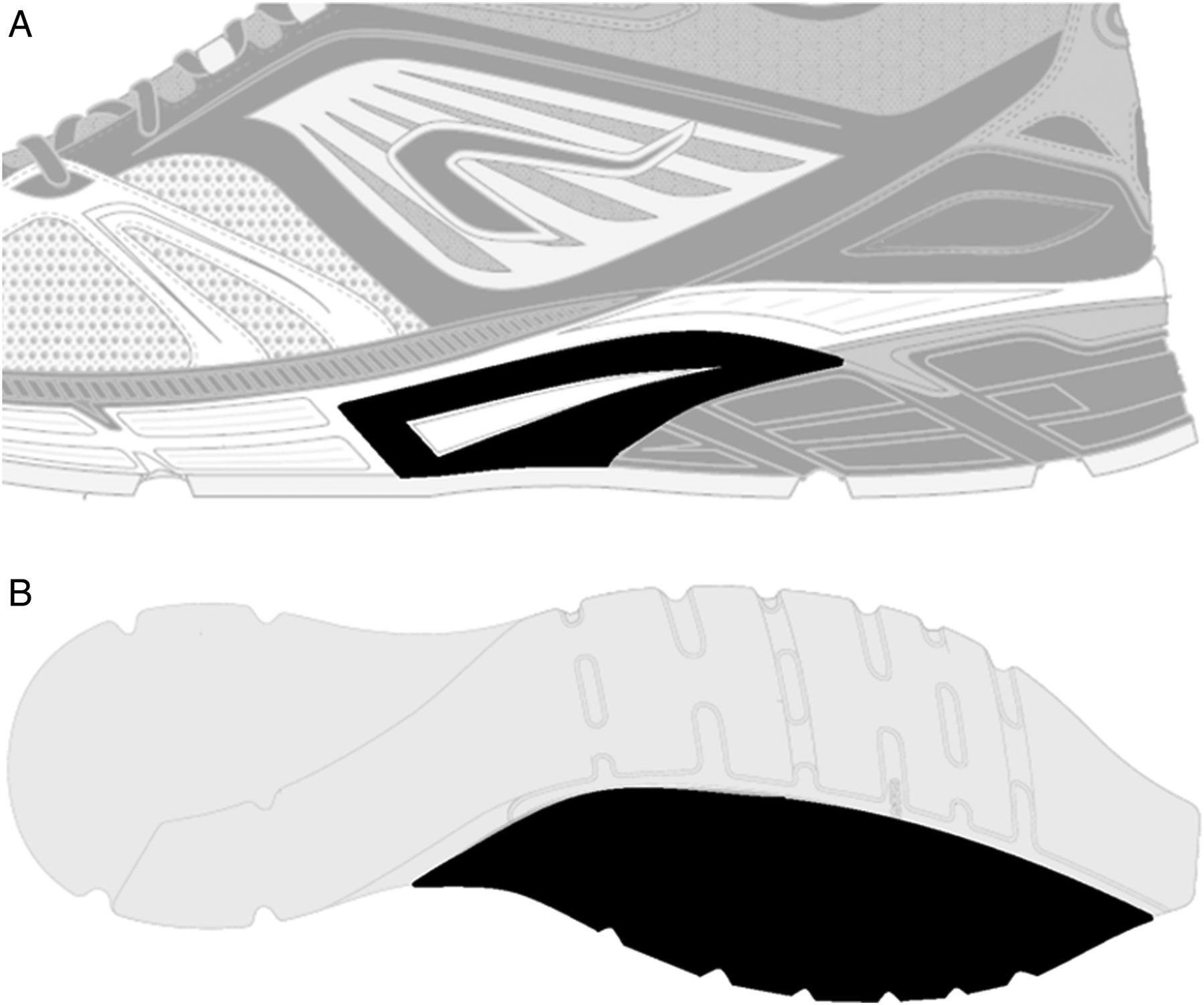
Two versions (motion control and standard) of a running shoe model were provided for the trial by a renowned sport equipment manufacturer. Shoes were de-identified so the study participants did not know which brand they were given. The motion control shoes and standard shoes both had a heel-to-toe drop of 10 mm and were derived from a commercially available model. Motion control shoes were characterised by (1) a thermoplastic polyurethane structure located at the medial part of the midfoot and (2) a dual-density ethyl-vinyl-acetate (EVA) midsole located at the forefoot (figure 1). Apart from these features, the two versions were identical, so participants did not know which type of shoe they used.

Illustration of the two technical features (coloured in black for illustration purposes) designed to limit the pronation movement of the runners. (A) Represents a piece of rigid plastic (thermoplastic polyurethane) located on the medial side, under the midfoot at the midsole edge. (B) Area of the harder midsole EVA (ethylene-vinyl acetate) foam. These elements were not recognisable on the shoe version distributed.
A subset of each version was characterised regarding midsole hardness difference between the medial and the lateral part of the midsole, using an Asker-C durometer according to the standard JIS K 7312 protocol for hardness characterisation of viscoelastic polymers (average value of 5 independent measures/shoe; 12 shoes tested/model). The measure was taken perpendicularly to the frontal plan, with the shoes cut at the level of the first metatarsal head.
Participants were randomly allocated to one of the two shoe models in accordance with stratification by potential confounders (age and body mass index (BMI); cut-off values are medians)16 and foot morphology. Participants and assessors involved in the shoe distribution and participant follow-up were both blinded regarding the shoe allocation. Each shoe pair was coded by a coworker not involved in the study prior to the distribution. The code was broken after completion of data collection.
Data collection during follow-up
A dedicated internet-based platform (http://www.tipps.lu, Training and Injury Prevention Platform for Sports) was used to collect all information of the participants pertaining to their sports participation and any adverse events (injuries, pains and illnesses).17–19 Training sessions were characterised by the type of activity, context, duration, subjectively perceived intensity measured using the Borg CR-10 scale,20 distance covered, running surface and shoes worn. Whether participants experienced any pain during the session forcing him/her to reduce volume or intensity, or to interrupt the practice, was also reported. The response to each item was mandatory for every declared training session or competition and could be selected from a predefined list.
Injury was self-reported and defined as any physical pain located at the lower limbs or lower back region, sustained during or as a result of running practice, and impeding planned running activity for at least 1 day (time-loss definition). The online injury questionnaire has been previously described.21 Injuries were classified according to consensus guidelines on sports injury surveillance studies.22 ,23
Self-reported data on every injury were systematically checked by the principle investigator for completeness and coherence. Participants who did not complete their entire running calendar with weekly information were contacted by one of the investigators to ensure that injury was not the reason for non-compliance. A participant was considered as dropping out of the study when no data had been uploaded in the system for more than 2 weeks despite an automatic email reminder and a phone call from the research team. At the end of the study (December 2014), the participants were invited for a final visit to check all injury data, compliance and shoe use.
Statistical analyses
Descriptive data for the shoe properties, as well as the personal and training-related characteristics are presented as count and percentage for dichotomous variables, and as mean and SD, or as median and range, respectively, for normally and abnormally distributed continuous variables. Average sport-related characteristics were computed for each participant over their specific period of observation. Lateral and medial midsole densities of both models were analysed using a Student's t test.
To address the first objective, unadjusted Cox proportional hazard regressions were performed to present the crude estimates of hazard ration (HR) for shoe version and other potential risk factors. Date at inclusion (shoe distribution date) and date at injury or at censoring were basic data used to calculate the time at risk. A participant was right-censored, yet included in the analyses, in case of severe disease, non-injury causing a modification of the running plan or at the end of follow-up (shoe return date), whichever came first. Time at risk was expressed in hours spent running and used as the time scale. To validate the statistical model, the assumption of proportional hazards was evaluated by log-minus-log plots. The variables with a p value <0.200 were included in the adjusted Cox regression analysis to determine if the use of motion control shoes is associated with injury risk, regardless of runners’ foot morphology, and controlling for potential confounders. The recommendation of using at least 10 injuries per predictor variable included in the Cox regression analysis was strictly followed.24
To address the second objective, a stratified analysis was performed to investigate the interaction between shoe version and foot morphology. HRs and their 95% CIs were determined for different foot morphology strata, with a single reference category (the stratum of runners with neutral feet, using neutral shoes).25 ,26 HR and the corresponding 95% CI were computed within strata of foot type to determine the effect of the shoe model within each strata. Significance was accepted for p<0.05. All analyses were performed using SPSS V.20.
Results
Participants
A total of 423 eligible volunteers came to the laboratory for the initial visit and shoe order. Thirty-seven participants did not retrieve their running shoes because of injuries (n=11) or other health problems (n=5) during the production period, lack of interest to participate (n=17) or withdrawal for personal reasons (n=4). A total of 386 pairs of running shoes were thus distributed. After shoe distribution, 14 participants were excluded from the analysis because they did not upload any training data (n=8), had not used the study shoes for more than 2 sessions (n=5) or had health problems unrelated to running (n=1). In total, 51 participants (figure 2) with similar demographics and foot type distribution to those of the final sample were excluded from the analyses (see online supplementary table S1).

{kind=link}
{kind=link}
Flow chart of volunteers and study participants.
A total of 12 558 running sessions were recorded for a distance of 116 723 km and 12 094 h run. Table 1 illustrates the characteristics of the two study groups, which both had a high compliance regarding the use of the provided study shoes. The average data uploading delay was 4 days. Since there were few participants with hyperpronated and hypersupinated feet, these categories were merged with those of pronated and supinated feet, respectively.
Participants’ characteristics and sport participation pattern for both study groups
Shoe characteristics
In motion control shoes, the midsole hardness was 15% higher (p<0.001) in the medial part compared to the lateral part (Asker C values 60±2 and 51±2, respectively), while there was no difference in standard shoes (51±3 and 51±2, respectively).
Injuries
An injury was sustained by 93 participants (25%) during the follow-up. The overall incidence was 7.69 injuries/1000 h of exposure (95% CI 6.28 to 9.41). There were 32.4% of participants injured in the standard shoe group and 17.6% in the motion control shoe group (RR=0.54, 95% CI 0.37 to 0.79). More details on the first-time injury characteristics are presented in table 2.
Characteristics of self-reported first-time running-related injuries for each study group (n=93)
Primary analysis
Overall, the injury risk was lower among the participants who had received motion control shoes (p=0.005; table 3). Both the unadjusted and the adjusted model revealed that previous injury was a risk factor (p<0.001). Additionally, BMI, running regularity and mean session distance were associated with injury risk, but only in the unadjusted model. Both models yielded very similar estimates for the shoe version. Thus, crude estimates were used in the secondary analyses.
Results of the unadjusted and adjusted Cox regression models for the variables tested
Secondary analysis
In the subgroup of runners with pronated feet (n=94), the rate at which the injuries occurred was significantly lower among the participants using the motion control shoes (HR=0.34; 95% CI 0.13 to 0.84; bottom line of table 4). This difference was not observed in runners with neutral (HR=0.78; 95% CI 0.44 to 1.37) or supinated feet (HR=0.59; 95% CI 0.20 to 1.73). No difference was found between the strata regarding the principle confounders (see online supplementary table S2). Interestingly, among the participants who received standard shoes, the rate at which the injuries occurred was significantly higher in the group of runners with pronated feet compared to runners with neutral feet (HR=1.80, 95% CI 1.01 to 3.22). In the group of participants with pronated feet, 25 had one foot classified as neutral. A sensitivity analysis showed that reclassifying these runners into the group with neutral feet did not affect the results.
Stratified analysis of the effect of shoe version according to foot morphology (n=372)
Discussion
This is the first large-scale prospective cohort study to investigate the effectiveness of motion control shoes on injury risk among regular leisure-time runners. We found that running in shoes with motion control was associated with a significantly lower overall injury risk, thus confirming our main hypothesis. However, in accordance with our secondary hypothesis, this general protective effect of motion control shoes was demonstrated only in runners with pronated feet, while those with neutral or supinated feet did not benefit from this technology. In addition, the stratified analysis revealed that, among the runners who received the standard shoes, those with pronated feet had a higher injury risk than those with neutral feet (table 4). Nevertheless, these secondary findings must be viewed as preliminary and need to be verified by further research including a larger sample size.
Matching running shoes to foot type?
The injury incidence reported in the present study (7.7 injuries/1000 h of running) was consistent with previous results from our laboratory and a meta-analysis (6.7 and 7.7 RRI/1000 h, respectively).26 ,27 The influence of shoe technology on injury risk in our study may appear inconsistent with some prior research. However, differences in study design, population and shoe characteristics must be considered. Previous studies in military populations6–8 and female runners9 have investigated the effectiveness of matching running shoes according to foot shape, but none found evidence for pronating runners to be advised to wear antipronation shoes.
Importantly, however, the study series by Knapik et al6–8 focused on military populations where recruits are exposed to high training loads during activities other than running, meaning findings may not necessarily be extrapolated to recreational runners. The study by Ryan et al9 involving female runners analysed the effect of three levels of footwear stability on pain outcomes. However, the participants were not blinded and their final sample size was small (n=81). Additionally, the study groups were not equivalent regarding body mass and running experience, two potential confounders. Furthermore, the ‘neutral’ running shoe used in their study (Pegasus, Nike) actually possesses motion control features, including a thermoplastic midfoot shank and a lateral sole flare. This illustrates that shoes from different brands presented as neutral may not be identical, and that care must be taken when drawing conclusions from studies that have used different shoe models.
A large prospective cohort study (DANORUN) in novice runners using neutral shoes previously questioned the belief that a pronated foot posture is a risk factor for injury.11 Indeed, that study revealed that runners with pronated feet were at a similar risk of injury compared to those with neutral feet. Contrastingly, we observed a higher injury risk in our subgroup possessing a more pronated foot posture. However, our target population (more experienced and regular runners) and shoe brand used were different. Since the DANORUN and the present study are currently the only ones to investigate the association between foot morphology and injury risk, further research is required to explain this apparent discrepancy and to reach a final conclusion.
Clinical implications
Runners have used cushioned shoes for only four decades, which contrasts with the long-term anatomical and neuromotor adaptations brought about by millions of years while running barefoot or in minimal footwear.3 One of the main characteristics of modern shoes is their cushioning properties aiming to increase the comfort and decrease the impact force at touchdown.28 However, the softer the sole of the shoe, the greater the risk of overpronation movement.29 A previous study already suggested that a certain degree of additional stability may be beneficial even for those individuals with neutral foot posture.9 This could be especially true for shoes with soft midsoles. The shoes used in the present study had an overall stiffness that was probably located within the lower 10–15% range of commonly available models, according to data from Shorten and Mientjes30 and those from our previous study.18
One might speculate that runners with pronated feet were insufficiently stabilised with the current standard shoe version and that additional motion control could be achieved with the motion control shoe version. The fact that motion control shoes are effective in controlling foot pronation, especially footwear with dual midsole materials used in this study,31 supports this argument. We observed that runners with pronated feet were protected when running in motion control shoes and that they were exposed to a greater injury risk when using the standard shoes. Unfortunately, in the absence of biomechanical data, the mechanisms involved in the injuries observed in our study are unclear. Future research should investigate what degree of motion control is needed in our modern cushioned shoes with regard to foot morphology and other footwear properties.
Strengths and limitations
Strengths of this study include the randomised controlled design with participant and assessor blinding, a stratified randomisation and a prospective follow-up over 6 months, plus the fact that the two running shoe versions were strictly similar except for the motion control features. A major limitation is that too few runners with highly supinated or highly pronated feet participated in the study, thus not allowing analyses of these subgroups. Additionally, the absence of significant results for runners with supinated and neutral foot types may be due to the low sample size, since the study was not powered for these secondary analyses. This limitation is highlighted by the small number of events observed in the stratum of runners with supinated feet, indicating that these results should be considered with caution (table 4). Given that the participants were asked to use the study shoes for all their running sessions, those runners preferring to use more than one shoe pair may have been reluctant to register. Thus, the volunteers included in this study may not represent all recreational runners. Another aspect of this study is that only one shoe model was tested regarding the effect of motion control technology. Therefore, our results may not be generalisable to other shoe models or brands.
Summary
The overall injury risk was lower among the participants who had received motion control shoes. Based on secondary analysis, it appears that runners with pronated feet may benefit most from this shoe type.
What are the new findings?
In recreational runners, the use of motion control shoes was associated with lower injury risk compared to standard shoes.
Among the runners using standard shoes, those with pronated feet were at a higher risk of injury compared to those with neutral feet.
Runners with pronated feet may benefit most from shoes with motion control.
How might it impact on clinical practice in the future?
With cushioned running shoes, some motion control may be necessary to limit injury risk in recreational runners.
Recreational runners with pronated feet using neutral shoes may be at an increased risk of injury.
Runners with pronated feet may be advised to try motion control shoes for running.
Acknowledgments
The authors would like to thank Dr Stephen Senn for preparing the randomisation, and Mr Daniel Karels and Mrs Romy Primc for their precious assistance with data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors LM, NC, ND, NG, AU and DT contributed to the study conception and study design; LM was responsible for the acquisition and analysis of the data. NC was responsible for shoe testing. LM and DT were responsible for data interpretation and manuscript drafting. LM, NC, ND, NG, AU and DT contributed to critical manuscript revision and approval. LM and DT were responsible for the overall content.
Funding This study was co-funded by Decathlon, Movement Sciences Department, Villeneuve d'Ascq, France.
Competing interests A research partnership agreement was signed between Decathlon and the LIH. ND, NC and NG are employed at Decathlon Group.
Patient consent Obtained.
Ethics approval National Ethics Committee for Research (CNER; ref 201211/04).
Provenance and peer review Not commissioned; externally peer reviewed.