Article Text

Abstract
Objective To assess the relationships between golf and health.
Design Scoping review.
Data sources Published and unpublished reports of any age or language, identified by searching electronic databases, platforms, reference lists, websites and from consulting experts.
Review methods A 3-step search strategy identified relevant published primary and secondary studies as well as grey literature. Identified studies were screened for final inclusion. Data were extracted using a standardised tool, to form (1) a descriptive analysis and (2) a thematic summary.
Results and discussion 4944 records were identified with an initial search. 301 studies met criteria for the scoping review. Golf can provide moderate intensity physical activity and is associated with physical health benefits that include improved cardiovascular, respiratory and metabolic profiles, and improved wellness. There is limited evidence related to golf and mental health. The incidence of golfing injury is moderate, with back injuries the most frequent. Accidental head injuries are rare, but can have serious consequences.
Conclusions Practitioners and policymakers can be encouraged to support more people to play golf, due to associated improved physical health and mental well-being, and a potential contribution to increased life expectancy. Injuries and illnesses associated with golf have been identified, and risk reduction strategies are warranted. Further research priorities include systematic reviews to further explore the cause and effect nature of the relationships described. Research characterising golf's contribution to muscular strengthening, balance and falls prevention as well as further assessing the associations and effects between golf and mental health are also indicated.
- Golf
- Health
- Exercise
- Evidence based review
- Sport
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
The objective of this scoping review is to map the literature on golf and health and to examine the relationships and effects of golf on physical and mental health.
Golf is a sport usually played on a large open-air course, in which a ball is struck with a club, with the aim of taking the lowest number of shots possible to get the ball into a series of holes in the ground. Golf is played by around 55 million people1 in 206 countries worldwide2 representing 1/127 of the global population. This global reach, and appeal to persons of all ages and abilities has seen golf reintroduced in 2016 to the Olympic Games, with efforts ongoing to secure Paralympic status for disability golf. Further information about golf is shown in online supplementary appendix 1.
Supplementary appendix
Health is influenced by a range of individual behaviours and characteristics, and the physical, social and economic environment that people are subject to.3 There is compelling evidence that regular physical activity has longevity, physical and mental health benefits for people of all ages, genders, geographical and socioeconomic backgrounds, and can deliver economic benefits for communities, as well as national and international policymakers.4–6
Golf has potential to provide physical activity, and thus health and social benefits to persons of all ages. Golf is particularly popular among middle-aged and older adults, who are generally less active than younger adults.7 ,8 To date the review evidence on this topic is limited. Previous reviews,9 ,10 including a systematic review,11 have been undertaken to consider the relationships between golf and health with many of these focusing on the subject of golf-related injuries, while a further review of undocumented methodology12 focused on health benefits only. A recent systematic review of health benefits related to sport suggested that evidence was conclusive only for football (soccer) and running, noting further evaluation and research looking at other sports, including golf, was required.13 A clear need exists to comprehensively review the relationships between golf and health. We therefore undertook a scoping review that maps available evidence, in order to identify the existing gaps in evidence and document impacts of golf on health where these data were available.
Methods
We adopted the established five-stage scoping review process proposed by Arksey and O'Malley, incorporating adaptions from Levac et al, and the Joanna Briggs Institute14–16 as per our published protocol.17 The following summarises our approach to each stage.
Stage 1: Identify the research question
Considering the populations, concepts and contexts of interest enabled a broad research question to be formulated:What is known about the relationships and effects of golf on physical and mental health?
Stage 2: Identifying relevant studies
Inclusion criteria:
Research articles not limited by geographical location, language or setting.
All age groups and both sexes of participants.
Research that considers the general population, as well as specific population groups (with a specific physical or mental illness or condition).
All forms of golf (including but not limited to 18 holes, 9 holes, driving range, spectating).
Any physical and/or mental health condition.
Sources of information, including primary research studies, reviews, systematic reviews, scoping reviews, meta-analyses, guidelines, as well as grey literature to include unpublished and ongoing trials, annual reports, dissertations and conference proceedings.
Exclusion criteria:
Opinion pieces/opinions, magazine and newspaper articles, case reports, papers with no data.
Health and safety/occupational issues not related to playing or watching golf.
Studies focusing on biomechanics, or improved performance in golf.
Search strategies and databases
Step 1: An initial limited search
An initial limited search (September 2015) of SPORTDiscus and Google Advanced Search for review articles and ProQuest for dissertations was conducted as detailed in the published protocol.17
Step 2: Identify key words and index terms
The title, abstract and index terms used to describe the articles identified in step 1 were analysed. The research team identified golf as the only primary research term. For the health-focused databases, namely MEDLINE and PsycINFO, ‘golf’ was used as the only search term to maximise inclusivity. Secondary search terms included a broader set of keywords for SPORTDiscus, Web of Science and Google Scholar. Boolean terms AND and OR were used to extract relevant studies. All relevant articles from SPORTDiscus and Web of Science were reviewed, with the same search strategy applying to Google Scholar. A pragmatic decision to review only the Google Scholar articles with these terms in the title was taken following consultation with a research librarian.
A similar strategy was applied to the grey literature. The same search terms used for SPORTDiscus, Web of Science and Google Scholar were applied to search for theses in the ProQuest database. ‘Golf’ as the only search term was used for the WHO International Clinical Trials Registry Platform. The advanced search function on Google was used to look for relevant reports and articles from the World Golf Foundation, the Royal and Ancient, the British Journal of Sports Medicine, The American College of Sports Medicine and the Faculty of Sports and Exercise Medicine while representatives of these organisations were contacted for further information.
Step 3: Further searching of references and citations
A search was conducted of the reference list of the most relevant identified articles while authors of relevant primary comprehensive, scoping or systematic reviews were contacted for further information.
The complete final search strategy is shown in online supplementary appendix 2.
Stage 3: Study selection
Supplementary appendix
Relevant titles and abstracts were evaluated against the eligibility criteria by one reviewer (ADM). A second reviewer (LD) completed the same process on a random sample of 10% of titles and abstracts, with concordance >97% regarding inclusion/exclusion decision. Where a consensus was not reached, the study proceeded to full-text review.
Scoping reviews are typically iterative, as reviewers become increasingly familiar with the research and evidence.14 We wished to focus on the relationships and effects of golf on physical and mental health. To enhance this focus, ‘studies focusing on biomechanics, or improved performance in golf’ was added to the existing exclusion criteria stated in the scoping review protocol.17
Full-text articles meeting the inclusion criteria were sourced. Translations by University staff and associates who were fluent speakers of Chinese, French, German, Italian, Japanese, Korean, Spanish and Thai to English were undertaken. Despite searching the University of Edinburgh library databases, using interlibrary loans and contacting authors, 318–20 of 365 papers could not be found and were excluded.
Stage 4: Charting the data
Extracting the results
Charting tables to record and assimilate extracted data from included studies were developed. A priori categories were charted as were emergent themes. Three reviewers (ADM, LD and EJ) undertook data extraction duties. A sample data extraction form is shown in online supplementary appendix 3. ADM extracted data from 90% of included studies and LD/EJ extracted data from 10% of studies. LD/EJ checked 10% of ADM's data extractions for accuracy and vice versa. Any discrepancies were discussed at group meetings. Concordance was >97% regarding inclusion/exclusion.
Data extraction categories
Author(s).
Year of publication.
Origin (where the study was published/conducted).
Aims/purpose.
Study population and sample size (if applicable).
Methodology/methods.
Intervention type, comparator, details of these.
Duration of the intervention.
Outcomes and details of these (eg, how measured).
Key findings that relate to the scoping review research questions.
Supplementary appendix
Stage 5: Collating, summarising and reporting the results
Methods employed in the protocol17 enabled us to collate existing knowledge on this broad topic and summarise and report as
A descriptive analysis, mapping the data, showing distribution of studies by period of publication, country of origin, study method and theme/focus.
A thematic summary, describing how identified research relates to the research question and aims, and the main findings from these organised by theme.
In this study, we aim to:
Map the evidence and key concepts available for golf and health.
Summarise and share existing research findings in a useful way for policymakers, practitioners and other relevant stakeholders.
Identify research gaps in the existing literature on golf and health.
Results and discussion
Descriptive analysis
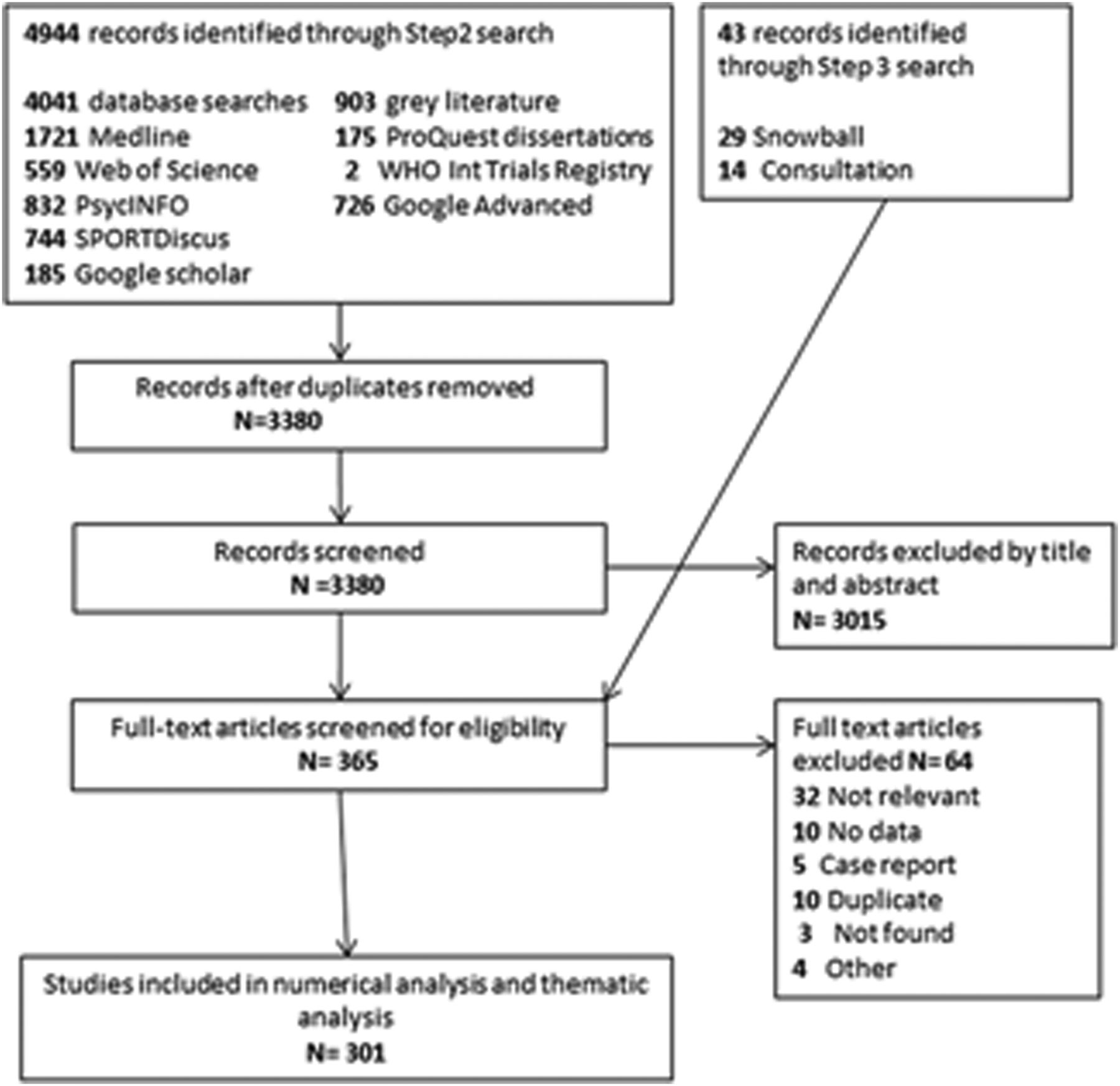
A review flow diagram (see figure 1) details the results from the search, and study selection processes.

Scoping review flow chart.
Our initial search identified 4944 studies. Of these, 4041 were identified searching databases/search platforms, and 903 from grey literature. After duplicates were excluded, 3380 records remained. A further 43 eligible studies were identified by snowballing or via expert consultation during the step 3 search.
In total, 362 articles underwent full-text screening, 3015 records being excluded after abstract screening with a further 3 articles excluded as full text was unavailable.
Overall, the scoping review identified 301 eligible studies relevant to the aims and research question ‘What is known about the relationships and effects of golf on physical and mental health?’ and these are included in the analysis.
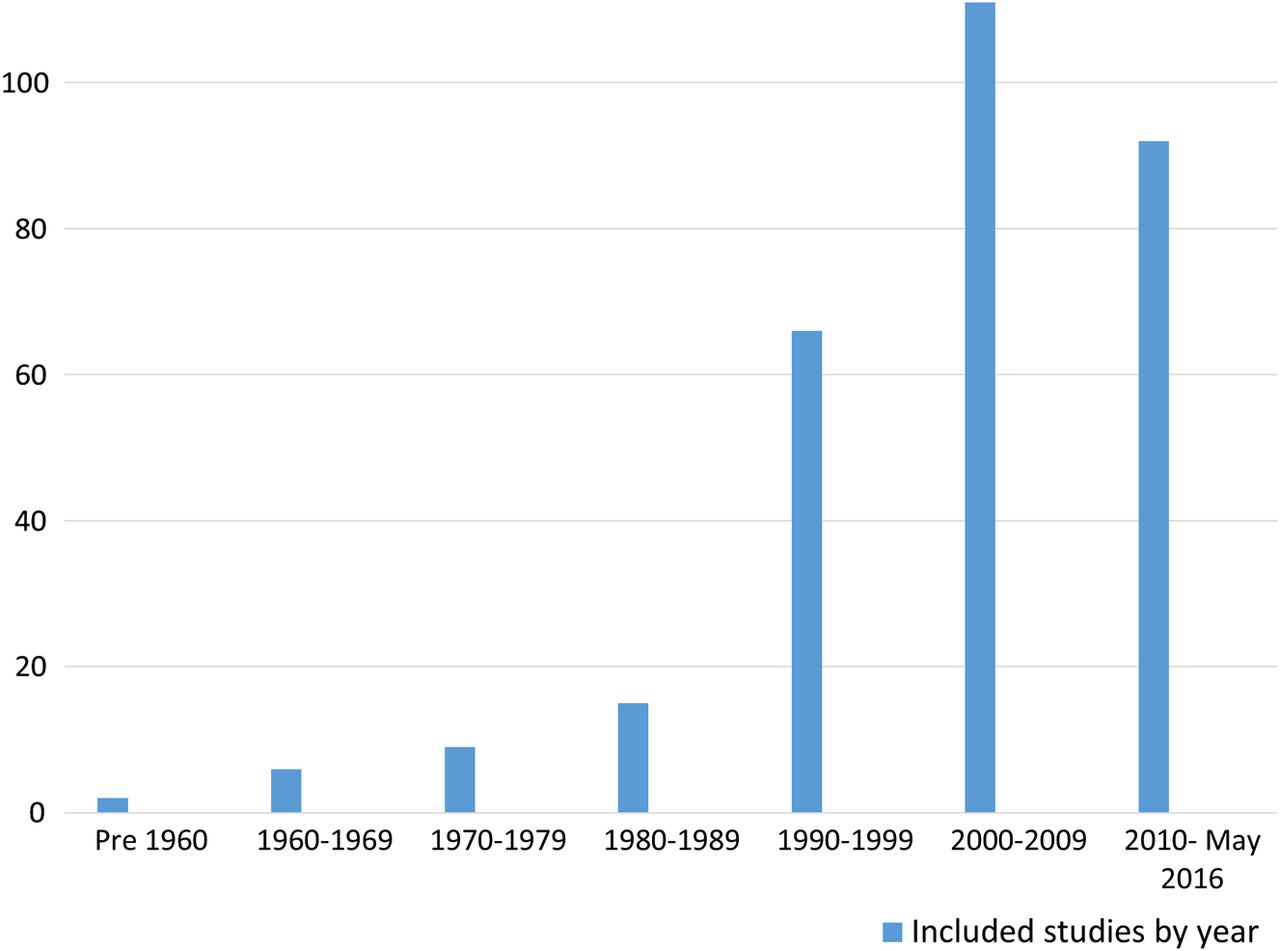
Included studies by year of publication
In keeping with wider bibliometric trends in sport and health research, figure 2 highlights a substantial chronological increase in the number of papers relating to golf and health, with an associated increase in the range of study designs and research questions.
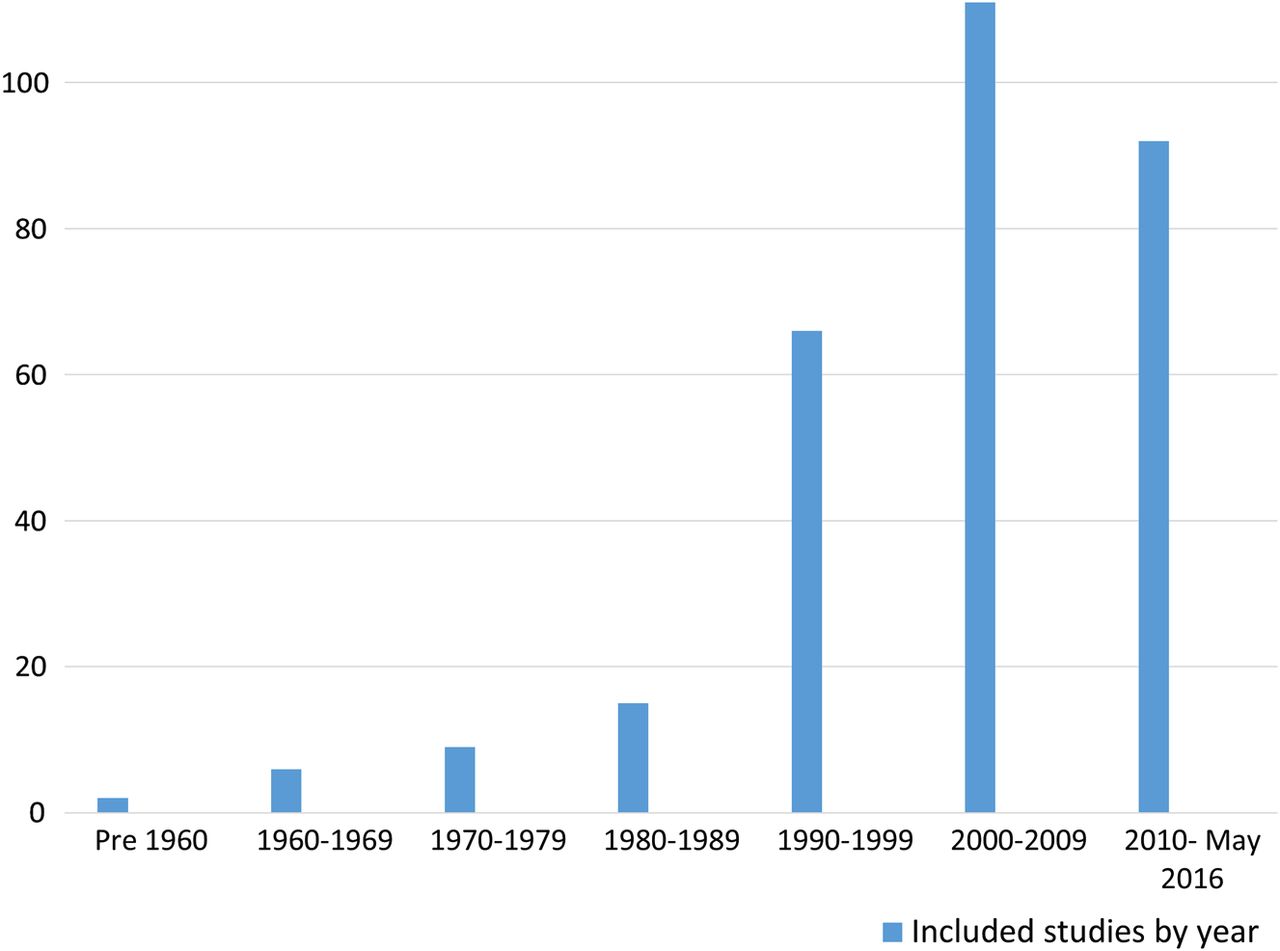
Included studies by year of publication.
Geography of included studies
Research studies were identified from 24 countries and in 9 languages. Table 1 demonstrates the percentage of included studies per country. The majority (53.8%) of included studies were from the USA, where almost half of the world's golfers live.2 Studies from North America (57.1%), Europe (22.3%) and Oceania (10.0%) are relatively well represented, as they are generally for research publications on physical activity.21 There were fewer included studies per golfing facility (eg, golf course, driving range and practice facilities) from Asia (10.0%) and Africa (0.3%), and none included from South America.
Geography of included studies
Type of study
Study design
The studies varied considerably in terms of study design and primary focus. No formal quality assessment of included studies was performed as scoping reviews are intended to provide a map of what evidence has been produced as opposed to seeking only the best available evidence to answer a narrow policy or practice-related question.15 A taxonomy of research designs included by the scoping review is shown in figure 3.

Taxonomy of research designs for included literature.
One hundred and seventy-eight (59.1%) were primary research, while 89 (29.5%) were secondary studies and 34 (11.3%) were grey literature.
Of the primary literature, 118 (66.3%) studies had a cross-sectional design, with 14 (7.9%) longitudinal and 46 (25.8%) experimental. The majority of the experimental studies quantified golf parameters, for example, steps taken or calories burned while playing golf. Overall 16 of 301 studies conducted a primary assessment of health outcomes in relation to golf, while only 4 conducted interventions principally aiming to promote behaviour change in relation to golf and health.
The vast majority of secondary studies were reviews. Only six of these were systematic reviews. The systematic reviews each focused on a narrow aspect of the broad topic of golf and health.
The grey literature comprised 17 published conference proceedings, 11 theses and 6 organisational reports.
Theme of the study
The primary focus of the included studies fitted broadly into four key themes, namely
Physical activity and golf (N=49).
Golf and physical health (non-injury/accident) (N=49).
Golf and injury/accident (N=135).
Golf and mental health/wellness (N=29).
These themes were formed from merging of the a priori categories identified. Additional studies from emergent themes were classified into a further category ‘other and general’ (N=39) to include studies of golf participation, implications for policy, legal implications or studies that focus evenly on more than one of these areas. Articles focusing on injuries and accidents relating to golf were the most frequent, comprising nearly 44.9% of included studies despite the exclusion of articles with a biomechanical/performance focus. Figure 4 shows the primary focus of included studies.

Primary focus of included studies.
Thematic summary
Key concepts and evidence available
Participation
Golf is a sport played by 55 million people in 206 countries, by males and females across the life-course.1 ,2 Globally, this compares to 250 million direct participants in football (soccer),22 75 million tennis23 and 5 million rugby union players.24 Gaining health benefits and exercise are powerful motivators for persons to play sport, and golf in particular.25–27 Golfers more frequently continue to play into middle age compared with participants in sports like football and rugby.28 ,29 Golf is played by people of all backgrounds, but participation is stronger in males,8 ,30 higher socioeconomic groups7 and more affluent countries.2
Golf and physical activity
Golf can contribute to physical activity as a leisure time or recreational activity, while work and occupation yields physical activity for modest numbers of professional players and caddies.31
The relative contribution of golf to population physical activity increases in older adults,27 ,31 a group that are typically less physically active than younger adults,32 but for all ages remains considerably less than recreational walking, which is highly accessible and often bears zero cost.31
Individual differences in energy expenditure can be large, depending on individual and golf-related factors, but golf can provide moderate intensity physical activity. Moderate intensity physical activity is recommended for children, adults and older adults for the longevity, physical and mental health effects it brings.33–35 Golf typically involves a mixture of exercise intensities. Golf can help persons and populations meet, and exceed minimum health and government recommendations for Moderate to Vigorous Physical Activity.36 ,37
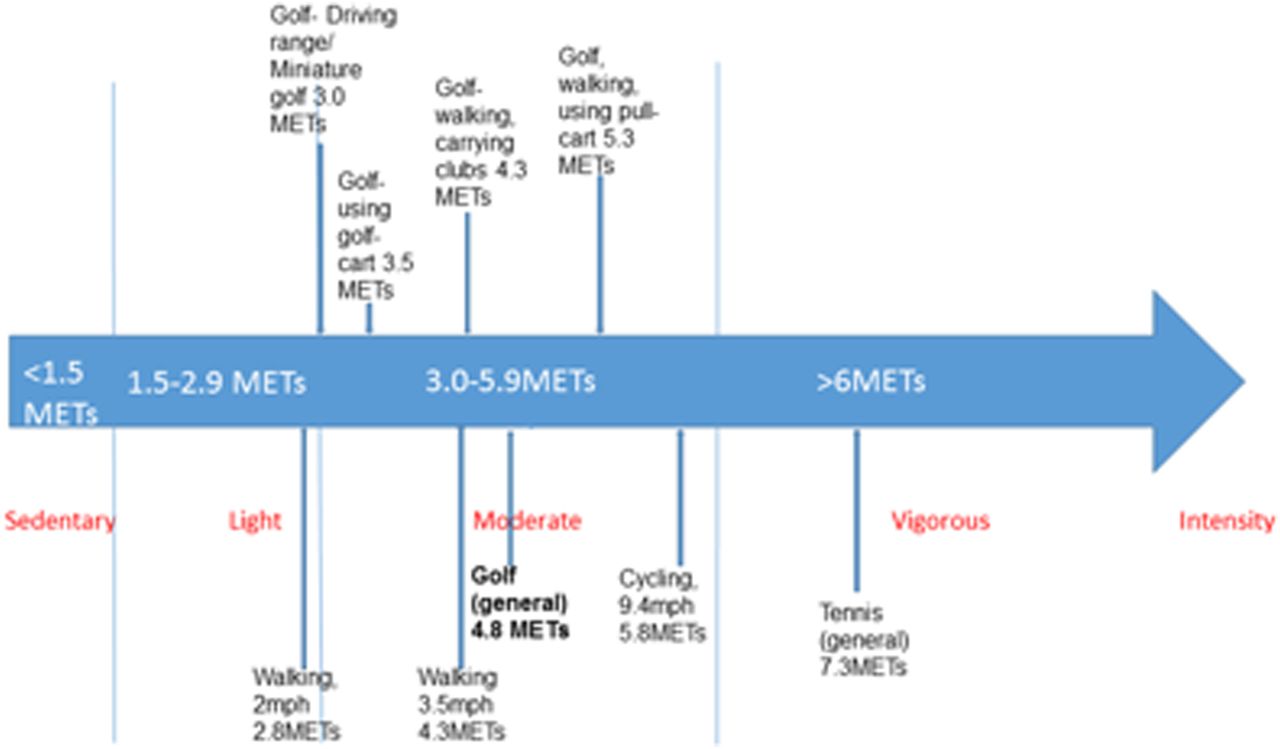
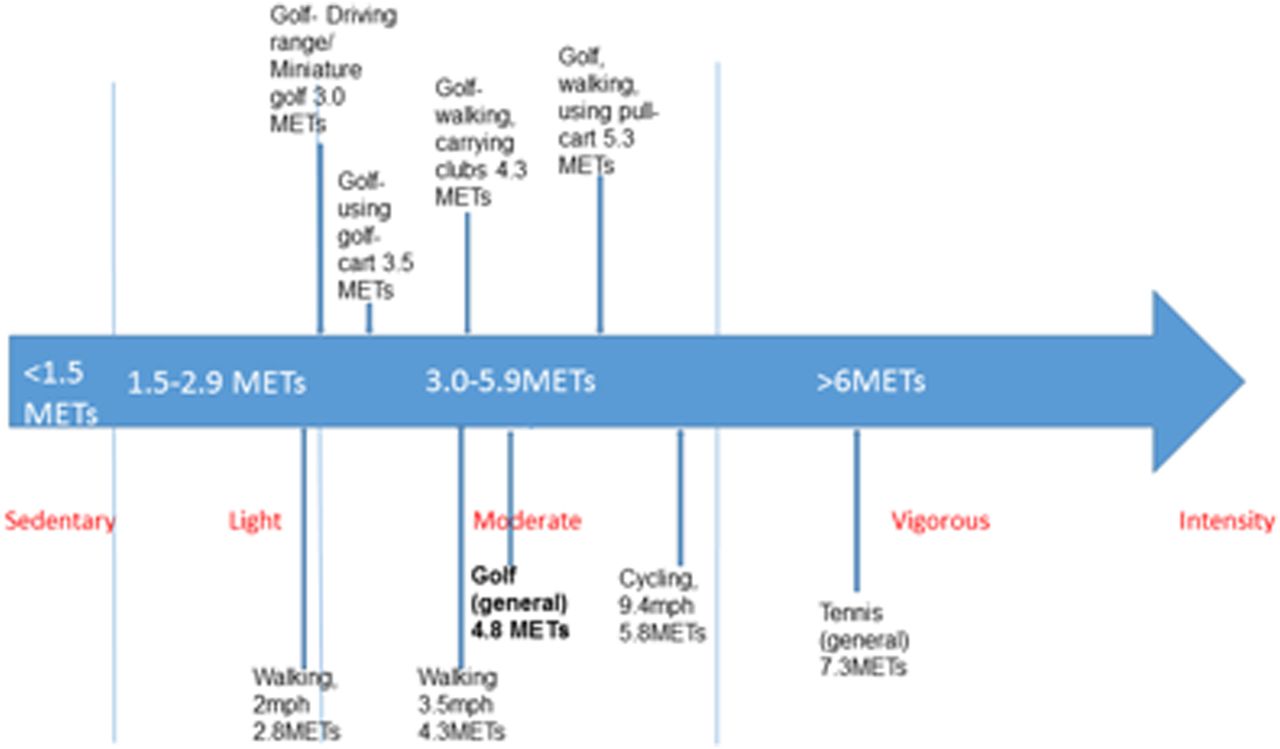
Studies quantifying golf by Metabolic Equivalent of Task (MET) value generally agree it offers moderate intensity aerobic activity,36 ,38–46 although with a wide range of MET values quoted (2.5–8.0) some studies classify it as low intensity47 ,48 or high intensity.49 ,50 The mean of the range of estimates is 4.5 METs. Figure 5 shows MET values attributed to different modes of golf and, for comparison, other physical activities suitable for all ages, by the Compendium of Physical Activity.38
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
MET values attributed to different modes of golf and other physical activities. MET, Metabolic Equivalent of Task.
Studies assessing calorie expenditure during golf typically classify golf as a moderate intensity physical activity with energy expenditure of 3.3–8.15 kcal/min,41 ,42 ,51–56 264–450 kcal/hour51 ,52 ,56 and a total energy expenditure of 531–2467 kcal/18 holes.36 ,42 ,43 ,47–49 ,51–53 ,56–59 Golfers walking 18 holes take between 11 245 and 16 66736 ,49 ,60 ,61 steps, walking 4–8 miles,36 ,48 ,49 ,51 ,57 ,60 ,62 while those playing and riding a golf cart accrue 6280 steps61 or just under 4 miles.51 There is poor agreement in the literature assessing intensity of golf by heart rate, with a majority classifying golf as low intensity,47 ,58 ,63–65 but others quantifying it as moderate to high intensity.36 ,57 ,66 ,67
Intensity of physical activity playing golf is higher for those walking rather than riding a golf cart,51 ,58 ,59 ,65 ,68 those playing a hillier course,55 ,67 older adults,66 heavier players,49 ,56 ,69 males36 and those of low baseline fitness. Intensity further varies depending if a player is swinging a club, walking or standing.69
Knowledge of the contribution of golf to muscle strengthening and to the balance aspects of physical activity recommendations is limited, and a priority for a review and further primary research. Studies suggest that golf may improve proprioception, balance, muscle endurance and function particularly in the elderly,57 ,70–74 while in younger players, no increase in muscle mass or bone mineral density has been seen.75
Sedentary behaviour is characterised as ‘any waking activity characterised by an energy expenditure over 1.5 METs and a sitting or reclining posture’.76 Time playing golf without riding a golf cart is non-sedentary time,36 ,38–45 ,47–49 and although golfers riding a golf cart do gain some health-enhancing physical activity, golfers walking the course gain more.
Unlike most other sports, golf spectating offers the opportunity to walk around the field of play, rather than being restricted to a seat. Spectators from North America and South Korea have highlighted ‘exercise’ as a reason for attending golf events, which can attract in excess of 500 000 spectators per week.77–79
Golf and longevity
Physical inactivity is a determinant of excess mortality, killing >3 million,5 and perhaps in excess of 5 million people annually.4 The 2010 Global Burden of Disease study highlights that physical inactivity is one of the top five causes of death in North America, Western Europe and in Australasia,5 three regions where golf is frequently played.2
The best available evidence suggests that playing golf may contribute to reduced mortality and increased life expectancy. When a Swedish study compared 300 818 golfers to non-golfers, they found a 40% lower mortality rate, although the study design and limitations meant that this could not be directly attributed to golf-related physical activity.80 The authors of that study speculate that this corresponds to a 5-year increase in life expectancy regardless of gender, age or socioeconomic status. This increase will also have further contributing factors, including other lifestyle factors. Playing sport several times per week is likely to benefit health more than playing one to two times per week.81 An association, but not causal relationship, is demonstrated between golf and life expectancy in Swedish and US studies.80 ,82
Golf and physical health
In providing moderate intensity physical activity, it is biologically plausible that golf could be expected to have beneficial effects in the prevention and treatment of chronic diseases, including ischaemic heart disease, type 2 diabetes, stroke, and colon and breast cancer.4 ,83 A review commissioned by the World Golf Foundation concluded that participating in golf can ‘yield a number of positive health and fitness effects’12 although methods were not stated and only health benefits were described. Frequent golfers perceive their physical health to be better than infrequent golfers.84
Cardiovascular system
Golf is associated with improvements in known risk factors for cardiovascular disease, including physical inactivity,38 blood lipid and insulin–glucose levels,57 ,66 ,85 body composition57 ,85 and aerobic fitness,57 although direct evidence and longitudinal trials assessing the medium-term and long-term impact of golf on coronary heart disease or cerebrovascular disease are lacking. Golf is reported as providing suitable exercise for patients with cardiac43 ,86 ,87 and stroke rehabilitation.88
Golf can provide a sufficient stimulus to improve aerobic fitness, but higher intensity exercise generates significantly improved cardiovascular adaption compared to playing golf.43 ,57 ,69 The effects of a season of golf on systolic blood pressure showed no significant difference in a controlled trial,57 while no consistent effect has been found measuring blood pressure during golf.64 ,67 ,86
There is an increased incidence of acute cardiac events during participation in sport89 and golf in particular.90–92 Golf players with new or unstable cardiac symptoms should consult a doctor.90 There is contradictory and inconclusive evidence regarding the effectiveness and cost-effectiveness of automatic external defibrillators situated at golf courses.93–96 An extremely rare mechanism of ischaemic stroke linked to golf has been described.97
Respiratory system
Regular participation in golf may improve lung function and maintain it in older adults.69 ,98 Separate golf and swimming interventions decreased hospital admission rates and symptom severity, while improving quality of life and parent satisfaction in a randomised trial of children with asthma.99
Metabolic health
Quasi-experimental studies are united in describing overall positive effects on lipid profile.53 ,57 ,67 ,85 Statistically significant effects of a season of golf on body composition (body weight, body mass index, waist-to-hip ratio and some skinfold thicknesses) are described in controlled trials,57 ,85 while a smaller study showed no effect on body composition.69 Blood glucose levels decreased during golfing activity in Swedish and Japanese studies.53 ,66
Cancer risk
An inverse relationship is demonstrated regarding physical activity and colon/breast cancer.4 Five ultraviolet radiation dosimetry studies report exposures that place golfers at higher risk of skin cancer than non-golfers.100–104 A cross-sectional study of female professional and amateur golf players highlighted increased numbers of non-melanoma skin cancers.105 Appropriate sunscreen, protective clothing and shade availability are suggested.100 ,106
Musculoskeletal health
Golf is associated with musculoskeletal benefits as well as accident and injury. Older golfers may gain improved balance,70 ,71 ,73 muscular function72 and strength74 compared to controls, but no lower limb bone mineral density increase was found in male professional golfers.75 Female caddies show better bone health than the general female population.107 ,108
Golf and injury
Injuries and accidents related to golf comprise the largest group of studies identified by the scoping review. A 2009 systematic review and other reviews describe golf as overall a moderate risk activity for injury compared to other sports.11 ,26
Prospective and retrospective epidemiological studies quote the incidence of injury in amateur golfers annually to be between 15.8% and 40.9%109–114 and lifetime injury incidence between 25.2% and 67.4%.10 ,115–118 Prospective longitudinal studies report very low injury rates compared to other sports, at 0.28–0.60 injuries per 1000 hours in amateurs.57 ,109 ,119 Professionals play more, and are injured more frequently, with annual injury rates of between 31.0% and 90.0%,115 ,120 and quoted lifetime incidence of 60.0–88.5%. Overall, the incidence of injury is moderate, and the rate of injury per hour played is low.
The most frequent cause of injury in amateur and professional golfers is volume of repetitive practice,113 ,114 ,116 ,117 ,121 while suboptimal swing biomechanics are a frequent115–117 ,122 and perhaps even leading109 cause in amateurs. Attention to these factors, and to an adequate warm up,26 ,123–128 and physical conditioning11 ,26 ,129 ,130 reduces risk of injury.
Regarding limb injuries, the lead side (the left arm and leg in a right-handed golfer) is more often injured than the trail (right side in a right-handed golfer).11 ,26 ,113 ,131 ,132 The mean length of missed practice or competition quoted is 4.0–5.2 weeks.116 ,117 The spine and particularly the lower back account for the greatest overall incidence of injury in amateur golfers (18.3–36.4%).109 ,115–117 ,133 The elbow (8.0–33.0%), the wrist and hand (10.0–32%) and shoulder (4.0–18.6%) are other frequently injured anatomical regions in amateur golfers.10 ,11 ,109 ,110 ,115–117 ,133
Golf is an infrequent cause of head and particularly ocular injury, but these injuries can be severe particularly in children.134–145 Injuries in children most often occur when struck by a club,134 ,140–142 while adults are more frequently hit by a ball. Most paediatric golf-related injuries occur away from a golf course134 ,143 with authors urging preventative strategies targeting improved education and supervision of children and safe storage of golf equipment.11 ,134 ,135 ,138 ,140
Although still infrequent, golf is reported to be the sport with the highest incidence of lightning strike in the USA146 with deaths,147 ,148 and prevention strategies for players and courses outlined.147
Golf cart-related injuries, including from falls, collisions or limb entrapment, can occur11 ,149 ,150 and can be severe.139 ,149–152 The US National Safety Council reports over 15 000 golf cart-related injuries per year, noting that not all are related to golf.149 Authors suggest regulation and instruction around safe golf cart use,150 ,151 as well as improvement and standardisation of safety features—for example, speed limiters, seat belts and front wheel brakes.149 ,150
Golf and mental health/wellness
No consistent evidence for the associations or effects of golf on mental illness was reported. Golf is associated with positive impacts on mental wellness.35 ,153 ,154 A wide range of methodologies, including qualitative interviewing, cross-sectional surveys and longitudinal studies, were used.
Mental health
A small experimental study enrolling nine persons with severe and enduring mental illness tentatively reported a number of mental and social benefits for participants.155 There is conflicting evidence relating to the effect of golf and other sports on mood and anxiety, with positive156 and negative62 mood changes noted. Improvement in stress and anxiety was reported by two studies156 ,157 highlighting stress-busting qualities, verbalised as a ‘sense of cool control’ and a ‘release of aggression’.157 Conversely, studies describe anxieties relating to performance on the golf course.62 ,157 Increased heart rates are noted prior to tournament play, consistent with prematch tension.86
Mental wellness
Quantitative and qualitative studies have described benefits related to self and group identity157–161 and social connections, many of which have been cultured long term.84 ,161 ,162 Golf facilitated opportunities for intergenerational interaction,163 ,164 and created opportunities to rebuild social connections86 ,161 and confidence165 during and post illness.
Self-efficacy, self-worth and physical activity levels improved after a golf intervention in 814 participants with a disability in the USA.166 In addition, self-worth in golfing populations158 ,161 and self-esteem156 ,167 in sporting populations that include golfers show positive change. An initial analysis of ‘The First Tee’—an at-scale US sport-based development programme—suggests that participants and parents noted improved confidence, interpersonal skills and emotional control.168 Finally, sunshine, fresh air and kinaesthetic pleasure were identified through qualitative interview responses as contributing factors to potential wellness162 benefits related to golf.
In summary, a number of qualitative and quantitative studies describe improved wellness in golfers, but there are few controlled studies looking at golf and mental health.
Further research priorities
This study has identified research gaps in the existing literature on golf and health with future research priorities outlined in table 2.
Research priorities related to golf and health
Limitations
Scoping reviews are comprehensive, but not exhaustive in identifying literature16 recognising the balance between the breadth and depth of analysis.169 Our search was subject to older but relevant sources being less available via databases, search platforms and search engines. Scoping reviews are broad in nature and provide an overview of existing literature regardless of quality, providing a broader and more contextual overview than systematic reviews. Formal assessment of methodological quality is not undertaken when conducting a scoping review,14 ,15 ,169 and synthesis of the literature quantitatively, nor demonstration of a cause and effect nature for the found relationships is not possible. Golfers are likely different to non-golfers in many ways, with confounding factors a challenge to identify and adequately control. Documented attempts were made throughout the design and conduct of this study to appraise and report evidence in an objective way.17 Rigorous and reproducible methods have been applied and authors are committed to publish all findings whether findings were positive, negative or not significant.
Conclusions
This scoping review identified over 300 studies investigating the relationship between golf and health. Golf has been shown to provide moderate intensity aerobic physical activity and therefore could be expected to have the same beneficial effects on longevity, physical health, mental health and wellness associated with physical activity.170 The scoping review cannot demonstrate causative effects, but reports evidence that is biologically plausible and relatively consistent, highlighting positive associations between golf and physical health, and mental wellness. The best available evidence suggests that golf may contribute to reduced mortality. The existing evidence supports efforts to promote golf as a sport with overall health benefits. To maximise health benefits, golfers should walk the course rather than riding a golf cart.
Research assessing golf's contribution to muscle strengthening recommendations, the relationships of golf on mental health, golf spectating and health, and the influencing of health behaviours in golfers, have been identified as priorities for further study. Systematic reviews to further explore health effects of golf on specific conditions are also required.
What is known?
Scoping reviews provide a useful framework to collate and summarise information on a broad topic.
Golf is played by over 50 million people of all ages worldwide.
What this study adds?
Playing golf can provide moderate intensity physical activity and has overall positive associations with physical health and mental wellness, while golf may contribute to increased longevity.
Disbenefits include (mostly overuse) injuries; accidents are rare, but deleterious consequences of them can be high.
Priority areas for future research include the associations and effects of golf on mental health, golf's contribution to muscle strengthening, balance and falls prevention, and influencing health behaviours among golfers and potential golfers. Systematic reviews to further explore the cause and effect nature of the relationships described are merited.
Acknowledgments
The authors wish to thank Marshall Dozier, the head librarian for population health at the University of Edinburgh, representatives of the World Golf Foundation, the Royal and Ancient, and the European Tour for their support in identifying suitable studies, and Maria Stokes, Evan Jenkins, Scott Murray and Ruth McQuillan for their advice regarding methodological considerations.
References
Footnotes
Twitter Follow Andrew Murray at @docandrewmurray, Paul Kelly at @narrowboat_paul and Nanette Mutrie at @nanettemutrie
Contributors All authors have contributed to the development of the research questions and study design. AM, EG and NM identified the method, whilst AM and DA identified existing scoping review frameworks to develop this scoping protocol. AM and LD developed and conducted the search strategy and data extraction. All authors developed the first and subsequent drafts of the manuscript. All authors reviewed and approved the manuscript.
Funding This work was supported by the Medical Research Council (MRC; MR/K023209/1), the Chief Scientific Office and an unrestricted grant from the World Golf Foundation.
Competing interests ADM and RAH received an unrestricted grant from the World Golf Foundation to fund this research. The World Golf Foundation agreed to publish findings whether positive, negative, or no associations or effects were found. RAH and ADM are remunerated for clinical work for the European Golf Tour.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Infographics