Article Text

Abstract
Objective A systematic review of factors that might be associated with, or influence, clinical recovery from sport-related concussion. Clinical recovery was defined functionally as a return to normal activities, including school and sports, following injury.
Design Systematic review.
Data sources PubMed, PsycINFO, MEDLINE, CINAHL, Cochrane Library, EMBASE, SPORTDiscus, Scopus and Web of Science.
Eligibility criteria for selecting studies Studies published by June of 2016 that addressed clinical recovery from concussion.
Results A total of 7617 articles were identified using the search strategy, and 101 articles were included. There are major methodological differences across the studies. Many different clinical outcomes were measured, such as symptoms, cognition, balance, return to school and return to sports, although symptom outcomes were the most frequently measured. The most consistent predictor of slower recovery from concussion is the severity of a person’s acute and subacute symptoms. The development of subacute problems with headaches or depression is likely a risk factor for persistent symptoms lasting greater than a month. Those with a preinjury history of mental health problems appear to be at greater risk for having persistent symptoms. Those with attention deficit hyperactivity disorder (ADHD) or learning disabilities do not appear to be at substantially greater risk. There is some evidence that the teenage years, particularly high school, might be the most vulnerable time period for having persistent symptoms—with greater risk for girls than boys.
Conclusion The literature on clinical recovery from sport-related concussion has grown dramatically, is mostly mixed, but some factors have emerged as being related to outcome.
- Concussion
- sex differences
- outcome
- moderators
- age
- sports
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Concussions can have large adverse effects on cognitive functioning and balance in the first 24 hours following injury.1 2 Injured athletes report diverse physical, cognitive and emotional symptoms during the first week following injury,1 2 and a greater number and severity of symptoms after a concussion are predictors of a slower recovery.3–6 There is tremendous interest in identifying factors that might influence outcome from sport-related concussion.1 7–18
For most injured athletes, cognitive deficits,11 19 balance20 21 and symptoms21 improve rapidly during the first 2 weeks following injury. The return to play timeframe is often reported to be within 10 days.20 22–26 However, this tends to be based on group-level findings only, not clinical outcomes from individual athletes, and group statistical analyses can obscure subgroup results and individual differences. Some athletes might return to play while still symptomatic,27 28 well before clinical recovery. During the past 10 years, there has also been accumulating evidence suggesting that a sizeable minority of high school and collegiate athletes take much longer than 10 days to clinically recover and return to sports.29–31
The longer recovery times might partially reflect changes in the medical management of concussion,32 33 with adoption of the gradual return to play recommendations from the Concussion in Sport Group statements from the conferences in Prague34 and Zurich.35 36 These return to play recommendations include no same-day return to play and a sequential progression through a series of steps prior to medical clearance for return to sports. In contrast, from 1995 to 1997, 31% of concussed high school and collegiate athletes returned to play during the same game that they sustained a concussion.28 Those sustaining grade 1 concussions returned on average 4 days following injury and those sustaining grade 2 concussions returned, on average, 8 days following injury.28
However, the translation of the Prague and Zurich return-to-play recommendations into clinical practice has likely been gradual. There is clear evidence that from 2005 to 2008 many concussed high school athletes in the USA were returned to play prematurely, in a manner not consistent with the practice recommendations.37 Studies conducted in the past few years seem to reflect a change in clinical management. For example, in a study conducted between 2012 and 2014, of the 1429 concussions reported among youth, high school and college-level athletes, 3.1% returned to play within 24 hours of injury.38
At present, it is reasonable to conclude that the large majority of injured athletes recover, from a clinical perspective, within the first month following injury.39–43 Neurobiological recovery might extend beyond clinical recovery in some athletes.44–47 Clinicians know that some student athletes report persistent symptoms for many months following injury, there can be multiple causes for those symptoms and those individuals are more likely to be included in studies conducted at specialty clinics.48 49
A range of preinjury individual differences, initial injury severity indicators, acute clinical effects or subacute clinical effects or comorbidities might influence outcome from concussion. Genetics,50 sex differences,1 16 18 51–53 younger age,1 7 12 38 54 neurodevelopmental factors such as attention deficit hyperactivity disorder (ADHD)55 56 or learning disability,57 personal57 or family history of migraine,58 or a personal14 58 or family history of mental health problems58 might also be predictors or effect modifiers of clinical recovery from concussion. Having a past concussion is a risk factor for having a future concussion,59 and having multiple past concussions is associated with having more physical, cognitive and emotional symptoms prior to participation in a sporting season.60 61 There have been inconsistent findings regarding whether specific injury severity characteristics, such as loss of consciousness, retrograde amnesia or post-traumatic amnesia, are associated with greater acute effects or prolonged recovery.5 15 56 62 Numerous postinjury clinical factors, such as the initial severity of cognitive deficits,4 63 64 the development of post-traumatic headaches or migraines,5 65 experiencing dizziness,48 66 difficulties with oculomotor functioning48 and experiencing symptoms of depression,67 have also been associated with worse outcomes after concussion.
There is a need to synthesise evidence regarding the relationship between demographic and clinical preinjury, injury-related and postinjury factors and clinical recovery after concussion. Therefore, this systematic review will assess numerous factors that might be considered intermediary, effect modifying, predictor or confounding variables in relation to clinical recovery from concussion. Clinical recovery is defined functionally as a return to normal activities, including school and sports, following injury. Operationally, it encompasses a resolution of postconcussive symptoms and a return to clinically normal balance and cognitive functioning.
Methods
The review protocol was prospectively registered in the PROSPERO database for systematic reviews (protocol ID: CRD42016041479). The broad initial review questions provided by the scientific leadership committee of the Concussion in Sport Group were: (1) What are the key modifiers of concussion outcomes? (2) What factors are associated with a poorer prognosis or future risk following concussion? (3) How do we best quantify the role of these modifiers? (4) How many concussions are too many? (5) How do sex differences impact concussion management? Given the breadth of the initial questions, we narrowed the focus of this review to predictors of clinical outcome.
We defined outcome as ‘clinical recovery and return to activities and sports’. We examined different types of predictor variables. Effect modification occurs when the magnitude of the effect of concussion on clinical recovery (ie, the association) differs depending on the level of a third variable (ie, the effect modifier variable). Intermediary variables are factors involved in the causal pathway between exposure (injury) and outcome (clinical recovery). Confounding variables are factors independently associated with the outcome (clinical recovery), and independently associated with the exposure (concussion), but they are not involved in the causal pathway between exposure and outcome. Confounding variables have a bidirectional association with both the exposure (concussion) and the outcome (clinical recovery).
Search strategy
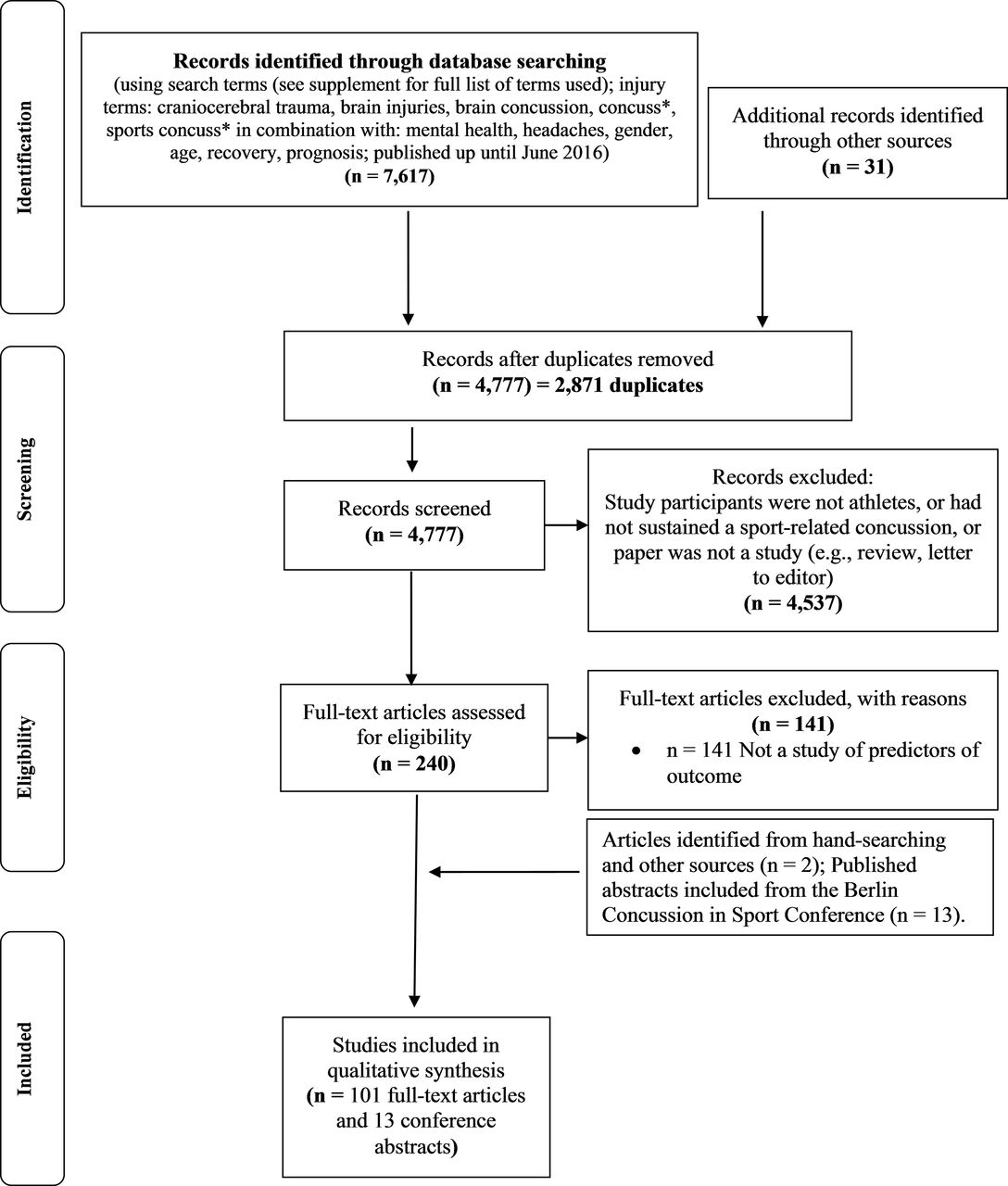
Articles were retrieved via online database searching, hand-searching reference lists and performing cited reference searches (see figure 1). We searched PubMed, PsycINFO, MEDLINE, CINAHL, Cochrane Library, EMBASE, SPORTDiscus, Scopus and Web of Science for articles published in English, from database inception to June 2016. Two general categories relating to (1) sport and athlete-related terms and (2) brain concussion-related terms were used as key search terms (refer to PROSPERO online registration (protocol ID: CRD42016041479), or see the online supplementary table, at the end of the table, for the specific search terms used). The search strategy initially included terms relating to imaging and biomarkers. However, after the search, these neuroimaging studies (as well as the results of serum biomarker studies) were determined to be beyond the scope of this review. The reference lists of articles retrieved for inclusion in the review were hand searched to identify other relevant articles. Key articles retrieved via online databases and through hand-searching reference lists were also used for further searches using the Web of Science Cited Reference function.
Supplementary Material
Supplementary Table 1
{kind=link}
Systematic literature search.
Article selection
Two reviewers conducted the initial screening of the titles and abstracts of articles identified in the search. We included articles that examined factors that may be associated with outcome from concussion and were conducted with humans. We excluded articles that addressed acute outcome in the initial days following injury, but did not address clinical recovery time or risk for persistent symptoms. Where there was uncertainty about whether a study should be included based on the review of the title and abstract, the full article was retrieved. To supplement the electronic database search, we examined the reference lists from previously published reviews and systematic reviews and the published abstracts that were presented as posters and oral presentations at the Fifth Conference on Concussion in Sport in Berlin in October of 2016.
Data extraction
For the included articles, all authors participated in the extraction of the first author, year of publication, the PubMed identification number, number of participants, proportion of female participants, age, setting, clinical outcome, predictors that were significant, predictors that were not significant and the period for assessing the clinical outcome. The level of evidence was rated using the Oxford Classification for Evidence-Based Medicine. Two or three reviewers independently extracted data from and rated each article. A third reviewer was sometimes needed to resolve discrepancies. Studies were sorted based on the specific predictor variables that were analysed.
Results
We found 7617 articles in the database search (figure 1). After duplicates were removed, 4777 were screened further by title and abstract for eligibility. Of the 4777 articles, 4537 were excluded on the basis that they did not examine athletes who had sustained a sports concussion, or the citation was not an original study (ie, the citation was a review article, editorial, letter to the editor or commentary). The PDFs of 240 articles were retrieved and reviewed. We included 101 articles and 13 abstracts from the Berlin Concussion in Sport Conference for review (figure 1). In the online supplementary table and in boxes 1–3, we report variables that had a significant independent association with outcome. There were major methodological differences across the studies (see online supplementary table). Some of these differences are listed below.
Research designs were diverse, including retrospective, prospective, case–control, inception cohort and epidemiological studies.
Many different clinical outcomes were measured, including symptoms, cognition, balance, return to school and return to sports.
There was considerable variability in when outcomes were measured.
The setting in which the study was conducted also likely influenced outcomes; recovery times were faster in studies conducted in educational institutions21 53 compared with emergency departments57 68 or specialty clinics.69
Summary of relationship between clinical recovery after concussion and preinjury, injury-related and postinjury factors
We extracted statistically significant predictors as well as predictors that were not significantly different (see online supplementary table). Some studies examined single variables, such as age70 71 or sex.31 52 72 73 Most studies, however, examined multiple variables. In the online supplementary table and in boxes 1–3, we report variables that had a significant independent association with outcome. It is important to appreciate that when multivariable analyses are conducted, many univariate significant findings drop out.56 57 68 For example, Zemek and colleagues found 47 variables that were independently associated with persistent symptoms after 1 month, but in multivariable analyses only nine remained significant predictors.57
Numerous studies have reported that younger age is associated with worse outcome, whereas many have not (see box 1). Age effects were examined statistically in different ways across the studies. Moreover, some studies reporting no age effects sometimes had fairly restricted age ranges.74–77 There were, however, large studies that did not find meaningful age effects.21 78 Prior studies have usually shown a gradient effect, with professional athletes returning to sports faster than collegiate athletes, then followed by high school athletes. Some recent studies have not shown a difference in recovery time between high school and collegiate athletes, however.21 78 Many studies have reported an association between female sex and worse clinical outcome (see box 1). A comparable number of studies have not reported significant sex differences in outcomes. However, large-scale observational studies indicate that girls and young women are at greater risk for having symptoms that persist for more than a month.57 79 80
Many studies have found an association between prior concussions and worse clinical outcome, but it is interesting to note that a greater number of studies have not found this association (box 1). Several studies have examined the association between mental health history and outcome, with nearly all showing an association with worse outcome. Most research to date does not support an association between ADHD or learning disabilities and clinical outcome. Nearly all studies do not show an association between a personal history of migraine and worse clinical outcomes (box 1). However, one large multisite prospective study reported that a history of migraine was associated with risk for symptoms lasting more than 4 weeks.57 There was consistent evidence that acute and subacute postinjury headaches were associated with worse clinical outcomes (box 3).
Some studies have reported that loss of consciousness is associated with worse clinical outcome, but most have not (box 2). Similarly, some studies have reported that ‘amnesia’ and post-traumatic amnesia are associated with worse clinical outcomes after concussion, but most studies have reported negative findings (box 2). There was strong evidence of a relationship between acute or subacute symptom burden and worse clinical outcome, although a few studies have not found this association (box 3).
Preinjury characteristics associated with recovery
Younger age:
Yes: Chermann81; Field82; Terwilliger83; Covassin84; Majerske85; Pellman86; Zuckerman71
No: Lau87; Hang30; McDevitt88; Nelson21; Asplund89 ; Chrisman75; Vargas74; Morgan58; Meehan42; Meehan90; Meehan6; McCrea91; Lee70; Baker92; Greenhill93; Nelson78; Corwin48; Preiss-Farzanegan94; Heyer80; Kontos67; Kriz77; Miller56, Ellis95; Gibson96
Female sex:
Yes: Baker31; Berz97; Henry29, Kostyun79; Bock49; Zuckerman98; Covassin84; Covassin73; Covassin53; Majerske85; Colvin99; Eisenberg68; Ellis95; Miller56; Preiss-Farzanegan(in adults)94 ; Heyer80; Zemek57
No: Chermann81; Moor100; Hang30; Nelson21; Mayers101; Asplund89; Black72; Chrisman75; Zuckerman102; Zuckerman103; Vargas74; Terwilliger83; Morgan58; Frommer52; Baker92; McDevitt88; Nelson78; Lax104; Ono105; Preiss-Farzanegan (in children/adolescents)94; Covassin106; Kontos67; Wasserman41; Yang107 ; Meehan90; Gibson96; Meehan6
Race (non-white):
No: McDevitt88; Asplund89; Morgan58; Yang107; Eisenberg68
Genetics:
No: McDevitt109
Prior concussions:
Yes: Hang30; Nelson21; Guskiewicz110; Castile39; Chrisman (football only)75; Zuckerman102; Morgan58; Covassin111; Kerr112; Colvin99; Meehan (binary)6; Meehan113; Miller56; Wasserman41; Slobounov114; Benson115; Corwin48; Bruce116; Eisenberg (if <1 year ago)68; Zemek57
No: Asken117; Barlow69; Moor100; Brown118; Lau87; Mautner55; McDevitt88; Vargas74; Terwilliger83; McCrea91; Meehan (number of injuries)6; Erlanger119; Majerske85; Baker92; Ellis95; Field82; Makdissi120; Pellman86; Gibson96; Heyer80; Miller56
ADHD:
Yes: Miller56
No: Asken117; Lau87; Mautner55; Hang30; Terwilliger83; Morgan58; Nelson78; Miller56; Eisenberg68; Zemek57
Learning disability:
Yes: Zemek57
No: Asken117; Lau87; Hang30; Asplund89; Morgan58; Nelson78; Eisenberg68
Prior psychiatric history:
Yes: Asken117; Morgan58; Eisenberg68; Ellis95; Yang107; Corwin48; Zemek57
No: Terwilliger83
Family psychiatric history:
No: None
Migraine (preinjury personal history):
Yes: Zemek57
No: Lau87; McDevitt88; Morgan58; Ellis95; Nelson78; Miller56; Eisenberg68; Meehan90; Meehan6
Family history of migraine:
Yes: Morgan58
Headache history:
Yes: Register-Mihalik121; Heyer80; Meehan6
No: Terwilliger83; Lau87; Nelson78; Meehan90
Note: First author and reference citation. Five studies by Iverson63 and Lau and colleagues (refs. 4, 66, 64 and 87) used the same cohort of football players and thus findings relating to specific predictors in boxes 1-3 are represented by only one of these five studies.
Injury severity characteristics associated with recovery
Loss of consciousness:
Yes: Chermann81; Pellman122; Guskiewicz110; Asplund89; McCrea91; Miller56; Benson115; Heyer80; Zemek57
No: Brown118; Guskiewicz123; Hinton-Bayre124; Nelson21; Bock49; Corwin48; Zuckerman102; Terwilliger83; Morgan58; Erlanger119; Lau4; McCrea25; Ellis95; Makdissi120; McDevitt88; Nelson78; Merritt5; Meehan6; Gibson96; Chrisman75; Collins 125; Meehan90
Post-traumatic amnesia/‘amnesia’:
Yes: Benson115; Chrisman75 (males only); Guskiewicz110; Heyer80; McCrea91; Lovell126; Collins125; Meehan6; Zuckerman102
No: Brown118; Guskiewicz123; Hinton-Bayre124; Nelson21; Asplund89; Bock49; Terwilliger83; Meehan90; Lau66; McCrea25; Ellis95; Makdissi120; Nelson (2016)78; Merritt5; Eisenberg68; Gibson96
Retrograde amnesia:
Yes: Asplund89; McCrea91; Zuckerman102; Nelson78; Pellman122
No: Lau66 ; Merritt5; Heyer80; Collins125; Nelson78;
Delayed removal from play/or additional head trauma:
Yes: Asken117; Terwilliger83; Heyer80
No: None
Note: First author and reference citation.
Acute clinical characteristics associated with recovery
Greater acute/subacute symptoms:
Yes: Chermann81; Brown118*; Hang30; Resch127; Castile39; Chrisman75; Zuckerman102; Meehan6*; Meehan*90; McCrea91; Benson115; Ellis95*; Greenhill93; Makdissi120; Nelson78; Merritt5; Heyer80; Iverson63; Collie128; Pellman122; Zemek57
No: Barlow69*; Moor100*; Morgan58
Acute headache:
Yes: Asplund89; Register-Mihalik129; Kontos130; Mihalik131; Benson115; Merritt5; Mihalik65 (acute ‘migraine’); Register-Mihalik121; Lau4; Zemek57
No: Mihalik65 (acute ‘headache’); Chrisman75
Acute dizziness:
Yes: Lau66; Erlanger119; Corwin48; Zemek57
No: McDevitt88; Benson115; Merritt5; Chrisman75; Pellman122; Makdissi120
Poor initial balance (objective):
Yes: Zemek57
No: Barlow69; McDevitt88; Nelson78; Lau66
Acute neuropsychological deficits:
No: Barlow69; Hang30; Nelson78; Pellman26
Note: First author and reference citation. *Some of these studies included both acute and subacute time periods, with most subjects being in the subacute time period.
Discussion
Most children, adolescents and young adults who experience a sport-related concussion will recover, from a clinical perspective, within 1 month.39 41–43 132 However, it is important to appreciate that the subgroup of children and adolescents who are taken to the emergency department following a sport-related concussion is at much greater risk for symptoms lasting beyond a month.57 68 In a multisite Canadian study, 30% of these children and adolescents reported persistent symptoms after 4 weeks.57 Both within and beyond the first month following injury, it is well understood in research and clinical practice that there are individual differences in recovery trajectories. In general, the literature is complex, mixed and difficult to interpret definitively.
Six key considerations when interpreting this review
There are baseline (preinjury) differences in student athletes’ experiences with, and reporting of, concussion-like symptoms, and these baseline differences can complicate our understanding of the relationships between predictors and clinical outcome. Prior to injury, girls and young women report more symptoms than boys and young men in most studies.10 60 People with pre-existing developmental or health problems, such as ADHD,60 133–135 learning problems,60 134 135 a history of mental health60 or substance abuse problems,60 a history of treatment for headaches61 or migraines,60 or multiple prior concussions60 61 129 report more symptoms than people who do not have these conditions.
Student athletes with ADHD 133 136–139 or learning problems136 have a greater lifetime history of concussion, and individuals with a prior history of concussion are at increased risk for a future concussion.59 There might be important interactions between neurodevelopmental problems, multiple prior concussions and clinical recovery from a future concussion. In large-scale multivariate analyses of baseline preseason symptom reporting in adolescents, past concussion history is a significant predictor of baseline symptoms, but the magnitude of its relationship to symptom reporting is less than the factors such as ADHD, past mental health problems and a personal history of migraine.60 61
Student athletes with no known developmental or health problems, and no prior history of concussion, also report some non-specific concussion-like symptoms in their daily lives.60 These symptoms can be related to stress,140 depression,141 insufficient sleep141–143 and a variety of other factors.
The results for nearly all the potential predictors are mixed, and for the most-often studied predictors (eg, age, sex and prior concussion history) there are many studies that do not show a significant association. The quality of included studies was variable, and the methodologies varied considerably, and this might influence the strength of evidence. We suggest not simply relying on a summary count of the number of studies in boxes 1–3 that showed an association versus not, because the studies varied tremendously in when and how they measured outcomes, in sample sizes and statistical power, sport population representativeness and methodological quality (see online supplementary table for details regarding the methodological differences in these studies).
Extracting non-significant findings from empirical studies can be difficult because authors often emphasise significant findings and do not always report negative findings. It was not always clear whether a predictor was statistically examined and whether it was a negative finding. Therefore, it is likely that the number of negative findings presented in the boxes is an underestimate (ie, there is a risk for publication bias).
Many past studies on the topic of predictors examine athletes only in the first 1–2 weeks following injury. In recent years, there have been quite a few studies that have examined predictors of those who are slow to recover and have persistent symptoms beyond a month.
Relationship between age and clinical recovery
Age is one of the most frequently studied preinjury demographic and health factors that might be related to outcome. There is some, but not definitive, support for a gradient age and level of play effect with clinical recovery being fastest in professional athletes, followed by college athletes, followed by high school athletes. In a large prospective multicentre study57 of children and adolescents presenting to the emergency department, the rates of those having persistent symptoms beyond 4 weeks, stratified by age group, were as follows: 5–7=17.9%, 8–12=26.3% and 13–17=39.9%. This suggests that the teenage and high school years might represent the greatest age period of vulnerability for slow recovery. However, younger children have less ability to conceptualise and verbalise their symptoms—whereas teenagers have an emerging ability to think more abstractly and they have a greater vocabulary for symptoms—so part of the difference in symptom rates might actually reflect developmental differences in how children and adolescents experience and report symptoms. Adolescents might also be more vulnerable to the social psychological effects of having sustained a sport-related concussion or have different motivational factors influencing their recovery. More research in these areas is needed.
Relationship between sex and clinical recovery
The literature on recovery time and persistent symptoms is mixed, but overall supports that females, on average, take longer to recover—and they are more likely to have symptoms that persist for more than a month.49 56 57 68 Sex differences, such as differences in neck strength,144–147 injury biomechanics148 and injury rates149 in females compared with males, and the fact that women report more symptoms, as a group, both before and after sustaining an injury,10 might help to account for this finding.
Relationship between history of concussion and clinical recovery
Prior history of concussions was not related to clinical outcome after concussion in most studies. However, because prior history of concussion is a risk factor for future concussions,59 prior concussions are associated with greater preinjury symptom reporting in some athletes,60 61 and some large-scale studies show an association between concussion history and increased risk for symptoms lasting more than 4 weeks,48 56 57 we consider concussion history an important variable. More research is needed to determine whether the risk for future concussion is greater primarily in those who had slower recovery from a past concussion.57
Relationship between neurodevelopmental disorders, mental health, migraine and clinical recovery
Children with neurodevelopmental disorders, such as ADHD and learning disabilities, have a greater lifetime history of concussion,136 150 perform more poorly, as a group, on neuropsychological testing134 135 139 and report more concussion-like symptoms in their daily lives,60 133–135 in the absence of injury. The literature to date suggests that those with ADHD or learning problems may have different baseline scores on symptom and neurocognitive measures but they are not clearly at greater risk for worse outcome or slow recovery following injury.
Preinjury mental health problems,58 particularly depression,57 68 are a risk factor for persistent symptoms in a small number of studies. A preinjury history of migraine was not related to outcome in most studies, but it was related in one large multicentre, prospective, well-powered study.57 Studies typically rely on self-reported headache history on a questionnaire, and many adolescents and young adults might have difficulty differentiating ‘headache’ from ‘migraine’, which could contribute to the mixed findings. Acute and subacute postinjury headaches of any type are a risk factor for persistent symptoms in some studies. Therefore, having a history of migraine might confer increased risk for slower recovery, but more research is needed to definitively establish this association.
Relationship between surrogate measures of injury severity and clinical recovery
There is a long-standing interest in whether injury severity factors, such as loss of consciousness, retrograde amnesia and post-traumatic amnesia, are related to clinical outcome. The literature is mixed regarding these variables. Most concussions are not demarcated by loss of consciousness,42 and loss of consciousness is not a strong predictor of outcome in most studies. Therefore, we consider it a weak predictor. Post-traumatic amnesia was not related to outcome in most studies. Retrograde amnesia has more consistently been associated with short-term outcome15 than loss of consciousness and post-traumatic amnesia, but fewer studies show an association between retrograde amnesia and slower recovery time.89 91 102
The initial injury severity indicators are less important than the early clinical consequences (ie, symptom burden) of the injury. Many studies have illustrated that greater severity of acute and subacute symptoms following injury are associated with slower recovery (see box 3). A small number of studies indicate that greater acute cognitive deficits are associated with slower recovery.63 119 These are intuitive findings because greater acute cognitive impairment likely reflects greater adverse effects of injury on neurobiology, and greater acute symptom reporting likely reflects the combined effects of neurobiology, adverse acute psychological reactions and greater preinjury propensity towards experiencing symptoms.
Limitations
This systematic review has several methodological limitations. First, we did not rate risk of bias or the methodological quality of the articles. We simply extracted details regarding the methodology, results and rated the level of evidence (online supplementary table). Second, there is a potential for publication bias in our conclusions because we only reviewed published articles; studies with negative findings are less likely to be published. Third, there is potential for language bias influencing our conclusions because we only included English language articles. Fourth, we could not pool data across studies and meta-analyse individual predictors or multiple predictors in combination. Finally, conducting a best evidence synthesis would have allowed us to better weight the quality of evidence when making overall summary statements about the relationship between individual predictor variables and clinical recovery.
Conclusions
The strongest and most consistent predictor of slower recovery from concussion was greater severity of a person’s acute and subacute symptoms following injury. Having a low-level of symptoms in the first day or two following injury was a favourable prognostic indicator. The development of subacute problems with headaches or depression are likely risk factors for persistent symptoms lasting greater than a month. Children, adolescents and young adults with a preinjury history of mental health problems or migraine headaches appear to be at somewhat greater risk for having symptoms greater than 1 month. Those with ADHD or learning disabilities might require more careful planning and intervention regarding returning to school, but they do not appear to be at substantially greater risk for persistent symptoms beyond a month. The teenage years, particularly high school, might be the most vulnerable time for having persistent symptoms—with greater risk for girls than boys.
What is already known?
Concussions can have large adverse effects on cognitive functioning and balance in the first 24 hours following injury.
Athletes report diverse physical, cognitive and emotional symptoms acutely and subacutely.
A greater number and severity of symptoms after a concussion are predictors of a slower recovery in some studies.
A large percentage of injured athletes recover clinically within 10 days, and the large majority appear to recover within 1 month.
Injury severity characteristics, such as loss of consciousness, retrograde amnesia and post-traumatic amnesia are not consistent or strong predictors of recovery time in some studies.
What are the new findings?
For the majority of predictors, the literature is mixed with positive and negative findings.
Preinjury mental health problems and prior concussions appear to be risk factors for persistent symptoms.
Greater acute and subacute symptoms are a consistent predictor of worse clinical outcome.
The teenage years might be a particularly vulnerable time for having persistent symptoms—with greater risk for girls than boys.
References
Footnotes
Contributors GLI and AJG wrote the first draft of the review. All authors participated in conceptualising the review, designing the search terms, reviewing the literature and extracting data from articles, reviewing drafts of the manuscript and approving the final draft for submission.
Competing interests GLI has been reimbursed by the government, professional scientific bodies and commercial organisations for discussing or presenting research relating to mild TBI and sport-related concussion at meetings, scientific conferences and symposiums. He has a clinical and consulting practice in forensic neuropsychology involving individuals who have sustained mild TBIs (including professional athletes). He has been a principal investigator and coinvestigator on federal and industry grants on topics relating to mild traumatic brain injury, neuropsychological assessment and depression. He has received consulting fees from pharmaceutical companies. He receives royalties for books and one neuropsychological test. He has received research funding from several test publishing companies, including ImPACT Applications, Inc., CNS Vital Signs and Psychological Assessment Resources (PAR, Inc.). He acknowledges unrestricted philanthropic support from the Mooney-Reed Charitable Foundation and ImPACT Applications, Inc. He previously served as a contractor in the area of TBI research through General Dynamics for the Defense and Veterans Brain Injury Center within the US Department of Defense. He receives salary support for chairing the Brain and Behavior committee for the Harvard Integrated Program to Protect and Improve the Health of NFLPA Members. AJG has a clinical practice in neuropsychology involving individuals who have sustained sport-related concussion (including current and former athletes). He has operated as a contracted concussion consultant to the Australian Rugby Union (ARU) from July 2016. He has received travel funding from the Australian Football League (AFL) to present at the Concussion in Football Conference in 2013. Previous grant funding includes the NSW Sporting Injuries Committee, the Brain Foundation (Australia), and the Hunter Medical Research Institute (HMRI), supported by Jennie Thomas. He is currently funded through the HMRI, supported by Anne Greaves, and the University of Newcastle’s Priority Research Centre for Stroke and Brain Injury. JLP is an employee of Monash University and Epworth Healthcare and conducts a private practice conducting assessments for forensic purposes. She has received funding from the Rehaklinik Bellikon and Suvacare to present on the management of concussion in Zurich in 2013. She frequently presents on TBI-related topics at brain injury conferences and has received funding from the International Neuropsychological Society, the International Brain Injury Association and World Federation of NeuroRehabilitation, Federation of European Neuropsychological Societies, British Psychological Society, Norwegian Neuropsychological Society and various hospitals to do this. She has received grant support from the National Health and Medical Research Council, Institute for Safety Compensation and Recovery Research, Victorian Neurotrauma Initiative, the Australian Research Council, the William Buckland Foundation, Epworth Research Institute and Monash University for studies involving people with traumatic brain injury. AKS is a full-time employee of the Vanderbilt University Medical Center. He is an unpaid consulting neurosurgeon to the NHL Nashville Predators, the MiLB Nashville Sounds, Vanderbilt University athletics and Mississippi State University athletics. He serves as unpaid member of the Medical Committee for the International Equestrian Foundation (FEI) and on the NCAA Concussion Protocol Committee. He is section editor (unpaid) for Sports and Rehabilitation for the journal Neurosurgery. He also receives compensation to serve as Unaffiliated Neurotrauma Consultant for the National Football League. He receives no direct grant or research support for concussion research. DKB is a full-time employee of the University of Virginia School of Medicine. Clinically, she evaluates primarily high school and collegiate athletes who have sustained sports concussions. She is a member of the Concussion Committee for the National/Women’s Basketball Association (NBA/WNBA) and is president of the Sports Neuropsychology Society, but receives no compensation for either activity. She has received grant support towards her salary on sports concussion-related research from the US Department of Defense, NIH/NHLBI and the National Athletic Trainers Association Research and Education Foundation. She has received speaking honoraria for scientific presentations on sports concussion. GSS is a full-time employee of the Vanderbilt University Medical Center. He is a consulting neuropsychologist for the NHL Nashville Predators, NFL Tennessee Titans, University of Tennessee Athletics and Tennessee Tech Athletics, with all fees paid to institution. He is also a member of the ImPACT Scientific Advisory Board and receives expense reimbursements for attendance at board meetings. He has received speaking honoraria for presentations at scientific meetings related to concussion in sports. He receives some grant support from the Department of Defense (non-TBI related).
Provenance and peer review Not commissioned; externally peer reviewed.