Article Text

Abstract
Background and objective Low-load exercise training with blood flow restriction (BFR) can increase muscle strength and may offer an effective clinical musculoskeletal (MSK) rehabilitation tool. The aim of this review was to systematically analyse the evidence regarding the effectiveness of this novel training modality in clinical MSK rehabilitation.
Design This is a systematic review and meta-analysis of peer-reviewed literature examining BFR training in clinical MSK rehabilitation (Research Registry; researchregistry91).
Data sources A literature search was conducted across SPORTDiscus (EBSCO), PubMed and Science Direct databases, including the reference lists of relevant papers. Two independent reviewers extracted study characteristics and MSK and functional outcome measures. Study quality and reporting was assessed using the Tool for the assEssment of Study qualiTy and reporting in EXercise.
Eligibility Search results were limited to exercise training studies investigating BFR training in clinical MSK rehabilitation, published in a scientific peer-reviewed journal in English.
Results Twenty studies were eligible, including ACL reconstruction (n=3), knee osteoarthritis (n=3), older adults at risk of sarcopenia (n=13) and patients with sporadic inclusion body myositis (n=1). Analysis of pooled data indicated low-load BFR training had a moderate effect on increasing strength (Hedges’ g=0.523, 95% CI 0.263 to 0.784, p<0.001), but was less effective than heavy-load training (Hedges’ g=0.674, 95% CI 0.296 to 1.052, p<0.001).
Conclusion Compared with low-load training, low-load BFR training is more effective, tolerable and therefore a potential clinical rehabilitation tool. There is a need for the development of an individualised approach to training prescription to minimise patient risk and increase effectiveness.
- Blood flow restriction
- musculoskeletal
- strength
- rehabilitation
Statistics from Altmetric.com
Introduction
Muscle weakness is highly prevalent among the most clinical musculoskeletal (MSK) conditions worldwide. The degenerative effects of muscle atrophy can be seen with both acute and chronic MSK injuries that result in prolonged treatment or muscle immobilisation, such as fractures and ligament injuries.1 Loss of strength is a major risk factor for osteoarthritis (OA),2 3 the most common MSK disease responsible for reduced function3 and quality of life of sufferers,4 affecting around 250 million adults worldwide5 with a prevalence correlating with the increasing age of the population.6 Muscle weakness is increasingly evident in non-injured healthy populations such as older adults due to sarcopenia. This describes a loss of physical function due to the decrease in muscle mass and strength,7 vascular function8 and bone mineral density9 that occur with ageing. Sarcopenia appears to be underpinned by the reduced sensitivity of ageing muscle to anabolic stimuli such as resistance exercise.10 The consequences of progressive and injury-related loss of muscle strength can be life changing. Strength training is indispensable in clinical MSK rehabilitation, and clinicians are faced with the task of turning the growing body of research into effective clinical practice. For instance, greater quadriceps strength has been linked to a lower risk of symptomatic knee OA11 and reduced joint space narrowing,12 as well as reduced pain and positive changes in physical function.13 Heavy-load resistance training has been advocated to offset age-related loss in muscle strength and mass,14 and strength training post-immobilisation is essential to regain the strength lost as a result of muscle disuse atrophy.
Historically, heavy exercise loads of approximately 70% of an individual's one repetition maximum (1RM) have been deemed necessary to elicit muscle hypertrophy and strength gains.15 Recent research has demonstrated that low-load training to failure can stimulate muscle hypertrophy comparable in magnitude to that observed with heavy-load training after 616 and 817 weeks of training three times per week. However, strength adaptations were maximised with heavy-load training,16 17 and cross-sectional comparisons would suggest that hypertrophy and strength gains observed with low-load training are not as great as those achieved with heavy-load training.18 Nevertheless, from a clinical MSK rehabilitation perspective, training to muscular failure may provide one strategy to maximise hypertrophy when training using low loads in situations when using heavy loads is not feasible. Training with low loads may therefore be useful, as the early addition of muscle mass and function in rehabilitation may be beneficial for individuals who have suffered from atrophy.
In recent years, research has demonstrated that augmentation of low-load resistance training with blood flow restriction (LL-BFR) to the active musculature can produce significant hypertrophy and strength gains,19–22 using loads as low as 30% 1RM.23 BFR training has been found to yield hypertrophy responses comparable to that observed with heavy-load resistance training;24 however, studies with such findings regarding muscle hypertrophy are not common among the present literature. Physiological adaptations in leg strength25 and vascular26 and pulmonary27 components have been reported with low-load aerobic exercise and BFR. From a mechanistic standpoint, it is hypothesised that an ischaemic and hypoxic muscular environment is generated during BFR to cause high levels of metabolic stress, alongside mechanical tension when BFR is used in tandem with exercise. Both metabolic stress and mechanical tension have been described as ‘primary hypertrophy factors’28 and theorised to activate other mechanisms for the induction of muscle growth. These proposed mechanisms include: elevated systemic hormone production,29 30 cell swelling,31 production of reactive oxygen species (ROS),32 33 intramuscular anabolic/anticatabolic signalling34–36 and increased fast-twitch fibre recruitment.37–39 However, at present these are mainly hypothetical and theoretical-based associations. Pragmatic and specific identification of these proposed mechanisms, including their magnitude of involvement and actual source of activation in BFR-induced hypertrophy is currently lacking and requires further exploration.
Nevertheless, these findings have important implications for individuals who cannot tolerate the mechanical stress of heavy-load exercise.40 LL-BFR strength training may be a clinically relevant MSK rehabilitation tool as it does not require the high joint forces associated with heavy-load exercise. Interest in the use of BFR training as a clinical rehabilitation tool is mounting,26 41 42 given the practicality that this training mode may offer in a clinical setting. To date, the effectiveness of LL-BFR training in clinical MSK rehabilitation has not been examined. It also remains unclear whether emerging research is informed by evidenced-based guidelines of implementing this novel training method to ensure safety and validity of findings.43 44
The main aims of this review were to conduct a meta-analysis to examine the effectiveness of LL-BFR training in clinical MSK rehabilitation, and a systematic analysis to examine study quality and reporting with a focus on safe and effective application of BFR. Thus, the objectives of this review were to (1) compare the effectiveness of LL-BFR training to both low- and heavy-load training without BFR; (2) systematically review studies examining LL-BFR training in clinical MSK rehabilitation and (3) from the results of the systematic analysis, examine and provide recommendations regarding safe and effective implementation of BFR training in clinical musculoskeletal rehabilitation.
Methods
Search strategy
This review was registered on the Research Registry database (reviewregistry91) and composed according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.45 A literature search to identify research papers examining BFR training in clinical MSK rehabilitation was carried out on the following databases for the time period of 1st January 1990 to 31st March 2016: SPORTDiscus (EBSCO), PubMed and Science Direct. The title and abstract of each study was screened; exercise training studies utilising BFR as a clinical MSK rehabilitation tool were selected. The reference list of relevant papers was also examined. The exact search terms were: ‘blood flow restriction’ OR ‘vascular occlusion’ OR ‘kaatsu’ AND ‘strength training’ OR ‘resistance training’ OR ‘exercise training’. This study received approval from the University’s ethics committee.
Inclusion and exclusion criteria
Exercise training studies involving individuals with a clinical MSK condition, published in English in a scientific peer-reviewed journal were included in the analysis. Studies were required to include BFR concurrently with exercise training. Only randomised controlled trials comparing LL-BFR training to either a low-load or high-load protocol without BFR were included in the meta-analysis. Any acute studies, case studies, single-arm studies or those not published in a scientific peer-reviewed journal in English were excluded from meta-analysis.
Study selection and data extraction
Studies were initially screened independently by two reviewers (LH and SDP) and those failing to match the inclusion criteria and any duplicates were excluded. From the remaining eligible papers, data were recorded relating to (1) study design; (2) clinical population characteristics; (3) rehabilitation protocol: type, frequency, occlusion characteristics, training load and duration of BFR training and (4) outcome measure: muscle strength and size, physical function and pain. Data regarding the safety of BFR implementation were obtained from the systematic analysis of the studies. Data were extracted using a custom spreadsheet composed by LH and SDP. For the meta-analysis, two comparisons were made: (1) LL-BFR training versus a matched protocol without occlusion and (2) LL-BFR training versus heavy-load training. Due to limited data regarding muscle size and physical function, the focus of the meta-analysis was on muscle strength. Risk of bias (figure 1) was calculated according to the Cochrane Collaboration guidelines.46

Analysis of risk of bias according to Cochrane Collaboration guidelines.46
Meta-analysis
Data analysis was performed by one author (LH) and reviewed by a statistician (CG). Data were extracted in the form of mean, SD and sample size for the meta-analysis. When insufficient raw data were provided, authors were contacted to provide raw data, or means and SDs were extrapolated from figures. Effect sizes were set at <0.40= small, 0.40–0.70=moderate and >0.70= large.47 All meta-analyses were conducted with the Comprehensive Meta-Analysis software V.2.2.064 (Biostat, Englewood, New Jersey, USA). Pooled data were analysed with a fixed-effect model to determine heterogeneity between studies using the I2 statistic, which determines the percentage of variability in effect estimates that is due to heterogeneity. Hedges’ g and 95% CI were used to calculate standardised mean differences for trials with sufficient data available. Significance level was set a priori p<0.05.
Study quality and reporting
Individual studies were assessed using the ‘Tool for assessment of study quality and reporting in exercise’ (TESTEX).48 TESTEX is a 15-point assessment scale, consisting of five available points for study quality and 10 for study reporting. For study quality, a point is awarded for: (1) eligibility criteria specification; (2) randomisation specification; (3) group allocation concealment; (4) presentation of baseline characteristics with no group differences and (5) blinding of an assessor to at least one primary outcome measure. For study reporting, points are awarded for: (1) at least 85% patient adherence; (2) reporting of adverse events; (3) reporting of exercise attendance; (4) intention-to-treat analysis; between-group statistical comparisons for a (5) primary and (6) secondary outcome measure; (7) use of point estimates; 8) control group activity is controlled and presented; (9) adjustment of exercise load and (10) if exercise volume and energy expenditure can be calculated. Data concerning reporting of adverse events and adjustment of exercise load, along with occlusive pressures, were used to address aim three of examining the safety and effectiveness of BFR implementation. Higher scores reflect better study quality and reporting. Any discrepancies in scores between reviewers were resolved by a third party (CG).
Results
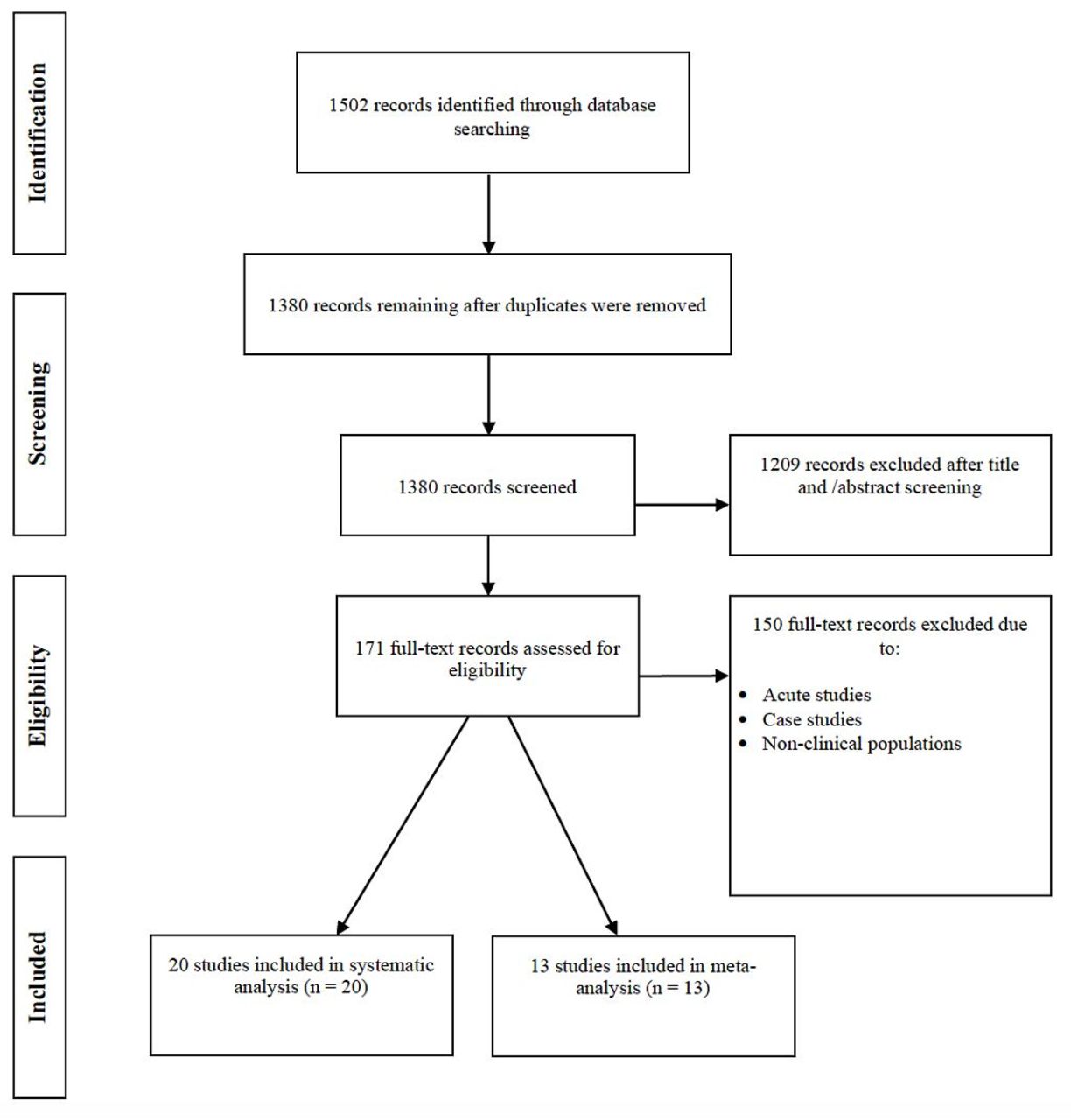
The database search yielded 1502 articles. After initial title and abstract screening, 171 were assessed for eligibility. Regarding clinical MSK conditions, a total of 30 articles were identified, including 20 exercise training studies, 6 exercise training case studies and 4 acute studies. From this selection, 20 and 13 studies were included in the final systematic and meta-analyses, respectively (figure 2). An overview of the studies is summarised in table 1. The main findings from the risk of bias assessment was that the majority of studies could not blind participants or conceal group allocation, and sequence generation was largely unclear (figure 1).

Flow chart of study selection process.
Overview of studies included in the systematic and meta-analyses
Meta-analysis
Eight studies meeting the inclusion criteria and comparing LL-BFR training to the same training without BFR had data extracted for meta-analysis. LL-BFR training had a moderate effect on increasing muscle strength in individuals suffering MSK weakness (Hedges’ g=0.523, 95% CI 0.263 to 0.784, p<0.001; figure 3). The I2 statistic of 49.8% represented moderate heterogeneity in the results. Five studies had data extracted for meta-analysis comparing LL-BFR training to heavy-load training. Heavy-load training had a moderate effect on increasing muscle strength compared with LL-BFR training (Hedges’ g=0.674, 95% CI 0.296 to 1.052, p<0.001; figure 4). The I2 statistic revealed minimal heterogeneity in the results (0%).
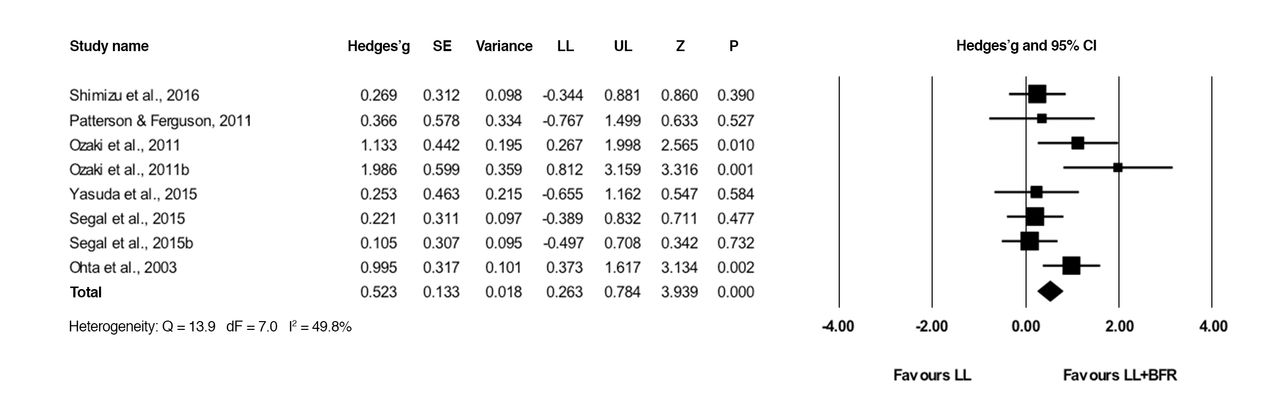
Forest plot illustrating the comparison of low-load training with blood flow restriction (BFR) to low-load training alone. Squares indicate individual study Hedges’ g and the lines represent 95% CIs. The size of the square corresponds to the weight of the study. The diamond represents the overall Hedges’ g, with its width representing the 95% CIs. LL and UL represent the lower and upper limit of 95% CIs, respectively. df, degrees of freedom.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot illustrating the comparison of low-load training with BFR, blood flow restriction (BFR) to heavy-load training. Squares indicate individual study Hedges’ g and the lines represent 95% CIs. The size of the square corresponds to the weight of the study. The diamond represents the overall Hedges’ g, with its width representing the 95% CIs. LL and UL represent the lower and upper limit of 95% CIs, respectively. df, degrees of freedom.
Clinical populations and BFR training interventions
Studies involved individuals with knee OA41 49 50 (n=3), ligament injuries42 51 52 (n=3), sporadic inclusion body myositis53 (n=1) and older adults susceptible to sarcopenia26 27 54–64 (n=13). The average age was 58±14 years for a sample range of 10–41 participants. BFR was used in combination with low-load resistance training,41 49 50 53 55 57 59 63 64 elastic band resistance training60 61 and low-moderate intensity walk training.26 27 56 58 62 BFR training was also used in conjunction with body weight exercises42 52 54 and individually without any exercise.51 BFR exercise training load ranged from 10% to 30% 1RM for resistance exercise, and 45% of heart rate reserve to 67 m/min−1 for aerobic and walking exercise. BFR was achieved using either pneumatic cuffs, hand-pumped blood pressure cuffs or elastic wraps ranging from 3 to 18 cm in width. Occlusive pressure across studies ranged from 60 to 270 mmHg. Studies either selected a pressure based on previous research, on total limb occlusive pressure or on systolic blood pressure. The duration of the BFR training intervention ranged from 2 to 16 weeks, with a frequency of 2 to 6 training sessions per week. Some studies did repeated sessions on the same day when BFR was used in isolation51 and in combination with simple muscle exercises.52
Outcome measures
Muscle strength was assessed by measurement of maximal isotonic strength,26 41 49 50 53–55 57 60–63 with a large majority of studies using the 1RM test.41 45–49 53–55 57 60 62 63 A number of studies examined maximal isometric27 42 56 57 61 and isokinetic27 41 42 49 56 57 strength. Muscle size was assessed by examining muscle CSA,26 27 42 51–53 56 59 61–63 muscle mass,56 muscle volume,27 41 muscle thickness58 60 and fat cross-sectional area (CSA).59 Studies that assessed physical function included tests of reaction time,54 stair climb power,41 single leg balance,54 timed stands,53 10 m walking time,54 maximum step distance,54 functional reach test,54 chair stand26 56 and the timed up and go test.26 50 53 54 56 A number of studies reported the presence or absence of any adverse events relating to BFR.41 49 53–55 57 59 63 64
Study quality and reporting
Median values regarding criteria matching were 2 (1–5) for study quality and 5 (3–7) for study reporting. Overall, studies had a median score of 7 out of the 15 possible points (range 4–12). The lowest scoring study scored 4,58 with the highest scoring 12.41 49 Studies scored highly for clear specification of inclusion and exclusion criteria (n=20)26 27 41 42 49–64; reporting of between-group statistical comparisons (n=19)26 27 41 42 49–52 54–64; and the use of point estimates and comparison of baseline measures (n=20).26 27 41 42 49–64 In contrast, a large majority of studies failed to meet criteria such as specification of the randomisation procedure26 27 51–63; blinding of participants (n=16)26 27 42 50–53 56–58 60–64 and assessors (n=15)27 42 51 53–64; and reporting of exercise session attendance (n=15).26 27 42 50–52 55 56 58–64 A number of studies did not monitor control group physical activity and present these data (n=19)26 27 41 42 49–63; report any or no adverse events to the BFR training (n=11)26 27 42 50–52 56 58 60–62 or adjust exercise load throughout the training period to account for muscular adaptations (n=9).26 27 42 50–53 55 57 59 60 62 63 An overview of the scores is presented in table 2.
TESTEX assessment of the quality and reporting of exercise training studies examining BFR in clinical MSK rehabilitation
BFR, blood flow restriction; MSK, musculoskeletal; TESTEX, Tool for the assEssment of Study qualiTy and reporting in Exercise.
Discussion
Meta-analysis
There is a growing interest in the use of LL-BFR training as a clinical MSK rehabilitation tool; however, the effectiveness of this novel training modality in clinical MSK rehabilitation has not been examined. Therefore, this review has provided insight into its effectiveness as a clinical rehabilitation tool for muscular weakness. The results indicate that augmentation of low-load rehabilitative training with BFR can produce greater responses in muscular strength compared with low-load training alone. At present, the strength gains appear to be smaller in magnitude to those achieved with heavy-load training. However, LL-BFR training is a more effective alternative to low-load training alone and may act as a surrogate for heavy-load training. Thus, LL-BFR training may be used as a progressive clinical rehabilitation tool in the process of return to heavy-load exercise.
The total Hedge’s g of 0.52 indicates that with the addition of BFR to low-load training, 69% of the population will experience greater gains in muscular strength.65 Mechanical tension would likely be similar between these modalities, and at present there is no literature to identify a clear mechanism to explain how LL-BFR training stimulates greater increases in strength compared with low-load training in clinical populations.41 It may likely be driven by hypertrophy and neural adaptations similar to those observed with heavy-load training, and the underlying mechanisms are also likely similar. However, with BFR exercise, these mechanisms may be activated by the combination of tension and hypoxia. It is important to note that this review indicated the strength gains observed with LL-BFR training were smaller in magnitude than those observed with heavy-load training. The total Hedge's g of 0.67 suggests that in the comparison of these two training modalities, 76% of the population will experience greater gains in strength with heavy-load training;65 this is in line with previous research.36 62
Although there was insufficient data to examine an effect size for muscle size in the meta-analysis, individual studies have demonstrated greater muscle volume26 and CSA in both lower26 27 42 and upper limbs61 alongside strength increases following LL-BFR training. This reflects findings in the literature involving healthy and athletic cohorts, where LL-BFR training has been shown to elicit greater increases in muscle size compared with low-load training alone.20 21 23 24 Furthermore, studies comparing LL-BFR training to heavy-load training in individuals with clinical MSK weakness reported similar increases in muscle CSA,60 62 63 which is in agreement with previous research.40 A number of factors have been propounded to have a potential role; again, however, no clear mechanism for BFR-induced hypertrophy is known. There appears to be a similarity between LL-BFR and heavy-load exercise in terms of molecular factors that lead to muscle growth. Therefore, the hypertrophy pathway may be similar between these two exercise modalities but possibly in response to different triggers due to, in large part, the characteristics of the exercise.
Systematic analysis
Results of the systematic TESTEX analysis of all exercise training studies examining BFR in clinical MSK rehabilitation demonstrated that a large majority of studies do not report on any or no adverse events to BFR,26 27 42 50 52 56 58 60–62 and many are not adjusting and individualising the occlusive stimulus and training load.26 27 41 49 54 56 58 61 64 Examination of extracted data regarding MSK and functional outcome measures revealed that LL-BFR training is effective at improving physiological aspects aside from muscle strength26 27 35 55 57 64 66 and may even be used without exercise to prevent muscle atrophy in early immobilisation.51 Furthermore, addition of BFR to low-load training does not appear to worsen condition or exercise-related pain;41 49 however, at present, there is a lack of investigation as to how muscular adaptations impact on an individual’s physical function.
Safety concerns of blood flow restriction training
Despite concerns of disturbed haemodynamics and ischaemic reperfusion injury,67 68 BFR training has been reviewed in depth69 70 and correct implementation has been affirmed to present no greater risk than traditional exercise modes.71 An epidemiological study in Japan reported low occurrence of any of the above adverse effects other than skin bruising.72 At present, there are no complete standardised recommendations for use even in healthy populations. Recently, cases of rhabdomyolosis have emerged73 74 despite a reported incidence of 0.008% in the aforementioned study. Most recently, this was reported in an obese Japanese male after only three sets of 20 reps of BFR exercise;74 however, no information regarding the exercise load or occlusive pressure was available, and the individual had been sedentary for a number of years. It is more likely that the cause was the stress of unaccustomed exercise on a sedentary body or the inappropriate use of BFR. However, another study by Iverson et al 73 reported rhabdomyolosis in a 31-year-old ice hockey player after one session of low-load BFR exercise.
This review illustrates that the majority of studies do not report on the presence or absence of adverse events. Although injury resulting from this type of training seems rare,44 the risks of adverse events may be exacerbated in clinical populations. Although muscle damage is common in BFR exercise75 and is necessary for training effects/adaptations, the possible risks of rhabdomyolosis occurring during BFR exercise may be heightened in cases of muscular disuse atrophy. It is important that practitioners rule out potential causes of rhabdomyolosis, such as infections and prolonged immobilisation76 before implementing training, and include measures of muscle damage markers (eg, serum creatine kinase) throughout the training period. This also emphasises the need for an individualised approach to BFR training when selecting cuff pressure for both safety and effectiveness.
Effective implementation of BFR training
Despite evidence of the effectiveness and tolerability of LL-BFR training in a clinical setting, various issues must be considered during implementation. Within the current literature, there is a lack of individualised prescription of BFR training. First, the occlusive pressure used is one aspect that should be individualised in the pursuit of safe and effective application. Research in healthy individuals has identified thigh circumference as an important predictor of occlusion pressure,43 with larger limbs requiring a higher pressure to reach the same level of occlusion as smaller limbs.77 Therefore, set pressures across a whole clinical cohort may not restrict blood flow to the same extent in all individuals. This may result in adverse cardiovascular outcomes,78 particularly if selected pressures result in complete arterial occlusion. It may also influence the effectiveness of the BFR stimulus, partially explaining discrepancies in study findings. For instance, the same LL-BFR protocol used in OA women by Segal et al 41 did not augment any increases in strength observed in the low-load exercise group in the same study in men.49 Men tend to have greater thigh circumference than women; therefore, it is conceivable that the same BFR pressure provided an insufficient hypertrophic stimulus in the male study.
A recent technique has emerged whereby calculation of total arterial limb occlusive pressure (LOP) allows for selection of a pressure at a percentage of LOP to standardise the level of occlusion across cohorts. This is used by the Association of Perioperative Registered Nurses to calculate required tourniquet pressures to restrict blood flow during surgery to minimise the risk of adverse events.79 LOP-based cuff pressures are lower than commonly used pressures but produce an effective surgical environment.80 Recent research employing this technique during BFR exercise demonstrated that higher LOP pressures are not required for greater facilitation of muscular responses to exercise compared with lower pressures.22 Furthermore, 40% LOP produced similar increases in muscle size, strength and endurance after 8 weeks of training to that of 90% LOP but without the high ratings of discomfort that were reported with the latter pressure.81 Lower and more tolerable pressures may elicit sufficient MSK adaptations while minimising the risk of adverse events and pain, highlighting the need for individualised prescription of clinical BFR training.
Individualisation of training prescription tools must also be considered, as this may effect progression and timescale of MSK adaptations. Although pronounced hypertrophy and strength gains have been reported after 4 weeks,23 2 weeks21 and even only 6 days82 of LL-BFR training, conflicting research demonstrated that BFR did not accelerate strength adaptations following 4 weeks of low-load training,49 suggesting longer training durations may be necessary.24 Progression of training load by re-evaluation of training prescription tools such as the 1RM is necessary for continued MSK adaptations to occur. A lack of this may compound the effects of the training stimulus and partially explain any insufficient MSK adaptations observed in longer duration training. The TESTEX analysis in this review revealed a lack of training progression in almost half of the studies, which may partially explain discrepancies in findings of MSK outcomes.41 49
A recent review advocated that for clinical populations, two to three LL-BFR training sessions per week with progressive overload is sufficient for enhanced strength adaptations.44 A previous meta-analysis of healthy cohorts demonstrated that this training frequency maximised adaptations to LL-BFR training.24 Progression of training may be difficult in certain clinical contexts, particularly post-surgery and during immobilisation. A progression model for using BFR in early rehabilitation through to high-load resistance training has been proposed by Loenneke et al, 83 which encompasses a four-step approach: (1) BFR alone during periods of bed rest; (2) BFR combined with low-workload walking exercise; (3) BFR combined with low-load resistance exercise and (4) LL-BFR training in combination with high-load exercise. Considering evidence from this review, a progressive model of BFR training may provide an effective rehabilitation tool from early ambulation to return to heavy-load exercise.
Other physiological adaptations to BFR training
Findings from the systematic review of all exercise training studies utilising LL-BFR training in clinical MSK rehabilitation identifies adaptations aside from muscle strength. In older adults who are increasingly susceptible to sarcopenia, LL-BFR training was shown to stimulate mTORC1 signalling and muscle protein synthesis in older men.35 Research has demonstrated increased serum concentrations of bone alkaline phosphatase66 and increased bone turnover following 6 weeks of LL-BFR training, suggesting an impact on bone health. Low-load walk training with BFR has been demonstrated to increase knee extensor and flexor torque,55 carotid arterial compliance,26 peak oxygen uptake,27 peak post-occlusive blood flow57 and vascular endothelial function and peripheral nerve circulation64 in older individuals. LL-BFR training can attenuate the effects of sarcopenia and may be effective at improving bone health. It may also be applicable for other clinical populations who suffer from MSK weakness and bone degradation (eg, patients with osteoporosis, rheumatoid arthritis, multiple myeloma and lymphoma). In premature situations when individuals suffering from muscle weakness are not able to begin even low-load exercise (eg, postoperative immobilisation), BFR alone can be used as an early rehabilitation intervention. Research has demonstrated effective attenuation of muscle atrophy51 and muscle strength84 using an occlusion protocol even at a low pressure of 50 mmHg,85 suggesting that BFR per se is effective at minimising atrophy. As high pressures can sometimes cause an uncomfortable dull ache,86 the notion of utilising lower pressures is clinically relevant. A definitive mechanism behind such adaptations to BFR per se, despite the absence of mechanical tension, has not been identified as yet. However, muscular responses to ischaemia and hypoxia induced by BFR such as increased ROS production,87 cell swelling31 and other intramuscular metabolic changes28 may play a role in promoting tissue growth in these situations.
An interesting observation in this systematic review is that the addition of BFR to low-load strength training does not appear to worsen condition or exercise-related pain. In women present with symptomatic factors of knee OA, Segal et al 41 found that the greater muscle strength increases observed after 4 weeks of LL-BFR (30% 1 RM) resistance training did not exacerbate knee pain throughout training, assessed using the Knee Injury and Osteoarthritis Outcome Score tool. The same study in men49 also found that BFR did not worsen knee pain. Research has shown that perceived exertion is higher during acute LL-BFR exercise compared with low-load exercise without BFR (both 30% 1RM).88 This was also demonstrated in a study involving older adults,89 alongside higher reported values for ratings of perceived pain during BFR exercise. However, such reported values for perceived exertion and pain are not necessarily high, and comparison of perceptual responses to LL-BFR (30% 1RM) versus heavy load (70% 1RM) exercise demonstrates that these responses are lower in LL-BFR compared with an equivalent form of exercise at a higher intensity.90 In addition, research has demonstrated a similar time course of adaptation to perceptual responses between LL-BFR and heavy-load exercise.91
This was recently reflected in clinical research when comparing this novel training modality to heavy-load training in patients with OA.50 The authors actually observed less knee pain during exercise across the training period in the LL-BFR group, likely attributable to the lower exercise load, alongside similar increases in muscle size and strength to the heavy-load group. Considering this and the findings from Hollander et al, 90 individuals may be able to tolerate perceptual changes during LL-BFR to a better extent due to lower joint forces and stress. In addition, such research advocates that LL-BFR training may potentially be comparable in effectiveness but more tolerable as a MSK rehabilitation tool compared with heavy-load exercise; however, the current research base for this is limited.
In clinical MSK rehabilitation, much emphasis is placed on an individual’s physical function and their quality of life. In this systematic review, it was evident that the majority of current research does not examine how MSK adaptations to BFR training transfer to these aspects. The few studies examining this demonstrated alleviation of condition-related pain41 50 and changes in various tests of functional ability.26 47 50 However, more investigation is needed to determine how MSK adaptations to BFR training are linked to changes in physical function and recovery of different clinical conditions.
Conclusion and recommendations
Strength training is important for many clinical populations during MSK rehabilitation. The clinical relevance of this review is the demonstration that LL-BFR training can provide a more effective approach to low-load and more tolerable approach to heavy-load rehabilitation. Individualised LL-BFR training prescription may provide a comparable surrogate for heavy-load training while minimising pain during training.41 50 51 92 This review has discussed some parameters of BFR training necessary to facilitate safe and optimal implementation, allowing clinical practitioners to make more informed decisions on the application of LL-BFR training as a clinical rehabilitation tool. BFR may facilitate early engagement in low-load strength training with limited joint stress in a broad range of clinical populations; therefore, it’s use in clinical rehabilitation warrants further study. As discussed in this review, future research should adopt an individualised and progressive approach to facilitate the effectiveness and safety of BFR training. And finally, future research must focus on identifying how various training adaptations impact physical function and quality of life during rehabilitation.
What is already known on this topic
A number of meta-analyses have demonstrated that low-load blood flow restriction (BFR) training can elicit substantial muscular hypertrophy and strength gains in healthy and athletic populations. The low-load nature of BFR training marks its potential as a clinical rehabilitation tool; however, the effectiveness of BFR training as such a tool has not been systematically examined.
What are the findings?
This study synthesises the available literature examining low-load BFR training in clinical populations, demonstrating its effectiveness in attenuating strength loss and facilitating strength rehabilitation in clinical populations suffering from musculoskeletal (MSK) weakness. Furthermore, low-load BFR training can have a positive impact on muscle size and numerous other physiological adaptations, and may act as a surrogate for heavy-load strength rehabilitation training in a broad range of clinical populations. Finally, this study provides recommendations regarding: developing a more effective individualised approach to BFR training, safe application of BFR training in a clinical setting and potential clinical conditions where BFR training may be beneficial.
How might it impact on clinical practice in the near future
This manuscript has discussed issues surrounding BFR and provided recommendations regarding the safe and effective implementation of BFR training in clinical MSK rehabilitation.
This paper may inform clinical practitioners of the many benefits of low-load BFR training and it’s use as a clinical MSK rehabilitation tool. BFR training is an emerging ‘hot topic’ in the UK and all around the world at present—this manuscript provides the first evidence base and guidelines within clinical MSK rehabilitation in the National Health Service and private healthcare setting.
References
Footnotes
Contributors LH and SDP participated in protocol design, data extraction, data analyses and manuscript preparation. CG participated in data analyses and manuscript preparation. BR and BP participated in protocol design and manuscript preparation. All authors have read and approved the final manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.